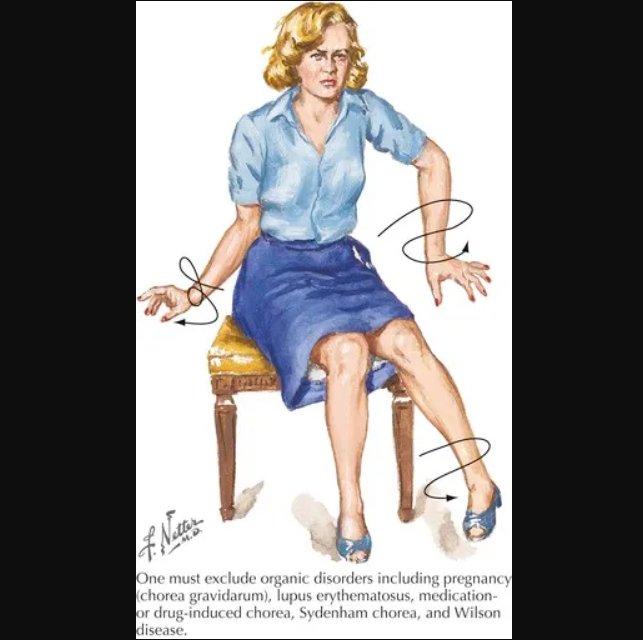
Tourette’s syndrome and similar tic-like behaviors are common, and can range from mild to very severely manifesting between afflicted patients. The overall prevalence of Tourette’s syndrome is estimated to be approximately 0.1-1% in the population, whereas cervical dystonia occurs much less frequently at mere 5-30 cases out of 100 000 (NIH, Swain 2005, Deik 2023). Chronic cough, on its side, has an overall prevalence of up to 10% of the population (Song 2015).
The scope of this article is not to detail the differential diagnoses and aetiologies of conventional knowledge, such as stroke, metabolic or autoimmune causes of movement disorders — these things should be excluded before one proceeds to presume musculoskeletal origins. This article will, rather, aim to shed light on differential diagnoses within the musculoskeletal system that can lead to these syndromes.
Pioneering work done by orthodontists Brendan Stack and Anthony Sims, first published in 2008, provided an opening for the notion of compressive neuropathy of cranial nerves as a precursor to spasmodic torticollis and other movement disorders (Sims & Stack 2008). What they found, was that compression of the auriculotemporal nerve in patients with temporomandibular joint disorder, symptomatic or asymptomatic, could generate a plethora of symptoms that far surpassed the conventional consensus. Within expert circles, it is known that TMD can cause trigeminal nerve symptoms such as facial burning and tinnitus (Beyers 1952, Freese 1959, Costen 1934). What had previously been unknown, however, was how compressive neuropathy of the trigeminal nerve’s branches, especially the auriculotemporal nerve, could induce movement disordes as seen in Tourette’s syndrome, and even myoclonic and spasmodic nerve disorders such as spasmodic torticollis / cervical dystonia, or generalized dystonia. They found that decompressive treatment for the temporomandibular joints would relieve compression of the auriculotemporal (again, the trigeminal) nerve, and subsequently and consistently provide relief of symptoms in a great number of patients.
What Stack & Sims postulated, as a theory to why this mechanism could provide relief for such seemingly unrelated symptoms, was that demyelination of the trigeminal nerve with compressive (ie. mechanical) origin could cause Epaphtic cross-talk between the trigeminal nerve and adjacent nerves within the brainstem, causing abnormal behavior of various networking nerves.
The lower portion of the spinal tract of V is called the subnucleus caudalis, and this is where the afferent “C” fibers synapse, cross and turn superiorly through the anterior trigeminothalamic tract to the thalamus. Interestingly, cranial nerves VII, IX, and X also transmit fibers through the subnucleus caudalis (Figure 1). There are mechanoreceptors and proprioceptive input (A-beta and A-alpha) fibers located within the spinal tract of V. Nociceptive pain is caused by the stimulation of peripheral nerves with A-delta and Cpolymodal pain receptors. Electrical connections can occur between adjacent demylelinated axons. These are referred to as ephapses.28-30 Epaphtic cross talk may result in the transfer of nerve impulses from one axon to another. Cross talk between A and C fibers develops in the dorsal root ganglion.
Another frequent finding in TS is throat clearing and sniffing. Examining the anatomy of the trigeminal nerve, we see that within the spinal tract of V, which ends in the subnucleus caudalis, there are connections within the subnucleus caudalis to the glossopharyngeal nerve, CN IX, which contains general sensory fibers and provides sensation from the posterior 1/3 of the tongue, tonsil, skin of the external ear, internal surface of the tympanic membrane, and the pharynx (Figure 3). When this nerve is chronically stimulated, the cough/gag reflex becomes paramount. If the primary chronic stimulus was not from the CN IX, but was from chronic stimulation within the subnucleus caudalis where CN IX and CN V decussate, would not the cough/gag reflex be stimulated? A well-documented finding in many movement disorder patients with TS is echolalia (the spontaneous utterance of sounds). Examining the anatomy within the subnucleus caudalis, one can see that the vagus nerve, CN X decussates within the spinal trigeminal nucleus as does CN V. – Sims & Stack, 2008
Following up on this work, in my own research, I have found that compression of several nerves can lead to tic-like symptoms and movement disorder. Moreover, I have found that the trigeminal nerve can be irritated at more than one site, ie. there are several branches of the trigeminal nerve that can be afflicted in TMD. Three different sites, overall, are to be considered:
- Temporomandibular joint and auriculotemporal nerve impingement (Costen’s syndrome (Costen, 1934))
- Buccal nerve entrapment within the lateral pterygoid muscles (Larsen 2017)
- Accessory, vagus or glossophargyneal nerve impingement between the C1 transverse process and skull’s styloid process (Larsen 2017)
The temporomandibular nerve is a small branch of the of mandibular division (3rd division) of the trigeminal nerve (5th cranial nerve), which is also the largest cranial nerve. The trigeminal nerve controls various processes in the head, on a broad spectrum, such as innervation of major cranial vasculature, facial sensation incl. heat and cold perception, mastication, autonomic ocular processes incl. the corneal reflex (elicits blinking), contributes to the typanic plexus of the middle ear, and more. Dysfunction of the nerve can lead to pain, but also dysfunction of its main and secondary processes. As we have already learned, it can also have a bleed-over effect and lead to diffuse symptoms such as tics and dystonias. The auriculotemporal nerve is compressed due to the mandibular condyle being situated too far back and up in the socket, and symptoms will typically exacerbate with high stress, bruxism, talking and chewing. Costen’s syndrome, and TMD as such, can be treated either conservatively through means of the protocol outlined in my TMD article (link), or combined with splint therapy that protracts the mandible. It is imperative to understand that the splint must be designed in a way the decompresses the joint; “bite balancing” splints are usually an expensive waste of time and can even make the patient worse.
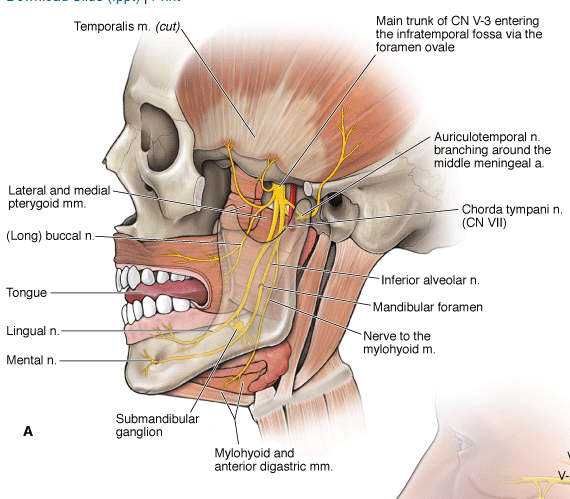
Figure 1: The auriculotemporal nerve emerges posterior to the mandibular condyle, and can becomme impinged at this site
The buccal nerve is yet another small branch of the mandibular divsion of the trigeminal nerve, and passes between the heads of the lateral pterygoid muscles. Severe weakness and subsequent myofascial fibrosis can cause entrapment of the nerve as it traverses through the muscle and lead to symptoms as described above in the auriculotemporal paragraph. Symptom exacerbation Treatment of this problem is slightly different than for the condylar compression, as decompression of the actual joint tends to produce fairly rapid relief, or at least improvement of symptoms when done properly. However, buccal nerve entrapment is caused by severe pterygoidal weakness and will improve slowly as the muscles heal with strengthening rehabilitation. One must absolutely refrain from botox and continuous massage and dry needling treatments, as this will make the muscle much worse in the long run (although it often causes short term relief!). Strengthening of the muscle must be done carefully one to twice weekly, gentle stimulus followed by muscle rest, allowing it to gradual regenerate. Symptom exacerbation would be expected for a few days following rehabilitation, which would provide increased diagnostic certainty in addition to the therapeutic effect. I detail the protocol in the TMD article that was referenced above.
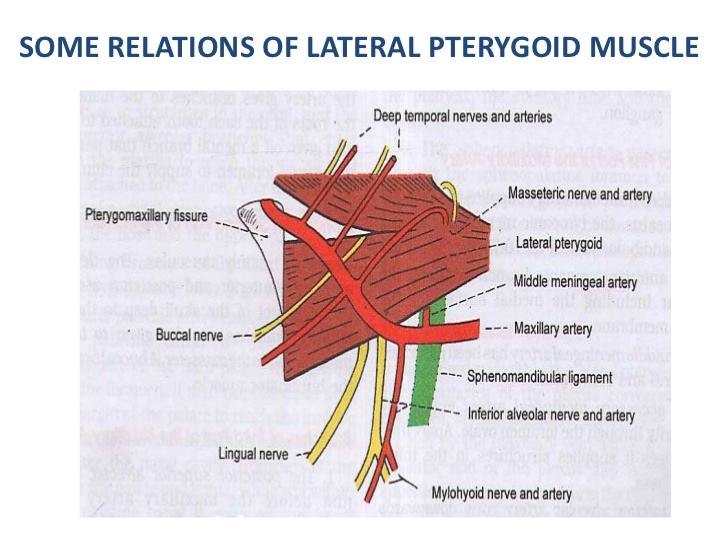
Figure 2: The buccal nerve passes between the lateral pterygoidal heads and can become entrapped at this site
Compression of the emerging nerves from the jugular foramen, or jugular outlet syndrome (I have an upcoming research paper on this topic), is another common cause of tic-like symptoms and movement disorders. The glossophargyneal, vagus and accessory nerves, also known as the 9th, 10th and 11th cranial nerves, pass through a bony passage between the C1 transverse process and the styloid process of the temporal bone of the skull. Approximation of these bones and impingemen of the traversing nerves and jugular veins can occur in prolonged severe postural dysfunction or post-traumatic cervical instability (Larsen 2017, Larsen 2018), as well as in hypermobility syndromes such as Ehler-Danlos and Marfan syndromes. Other congenital factors, such as the transverse process’ width and angulation of the styloid process will also be predisposing factors for passage narrowing (Gweon 2011).

Fig. 3: CT scan in flexion extension that shows approximation of the styloid when the patient tucks his chin. The jugular vein is crushed as a result. Passing along the internal jugular veins, as stated, are the 9, 10 and 11th cranial nerves.
Regarding cervical dystonia and myoclonias, it is already well known and accepted that cranial nerve compression can cause myoclonus. What is much less known, is the “bleed over”-effect that Sims & Stack was referring to. Nonetheless, facial myoclonus, by example, is a highly recognized disorder of facial muscle spasm (hemifacial spasm) that is caused by facial nerve compression, usually by tumor or aneurysm intracranially. Likewise, impingement of the accessory nerve can cause refractory spasm of the muscles innervated by the accessory nerve (trapezius and sternocleidomastoid muscles), which is known as spasmodic torticollis and cervical dystonia. Compression of the glossopharyngeal nerve is known to cause throat and anterior neck pain, but it can also affect the vocal cords via the anastomosis with the laryngeal nerves, as well as the tongue. Oromandibular dystonia or myoclonus can follow. This can also have bleed-over effects to the hypoglossal and facial nerves that pass adjacent to these, and can cause dystonia of the platysma muscles as well as hemifacial dystonia, both uni- and bilaterally. Compression of the vagus nerve can cause a vast array of symptoms that, really, only God knows the true potential extent of. The vagal nerves innervate all organs and is the largest and most expansive nerve to carry parasympathetic signals. It innervates numerous functions that exceed the scope of this article. However, within scope, it innervates the vocal cords, gag reflex, cough reflex, and eustachian tubes. Chronic coughing, gagging, throat clearing, ear popping, and other Tourette-like and myoclonic and dystonic symptoms can follow.
Diagnostic workup
Depending on what your actual problem is, always make sure to exclude conventional causes of movement disorders such as autoimmune, craniovascular disorders and drug-iatrogenesis. Drug induced akathesia, for example, would typically elicit with starting or stopping a certain drug, whereas musculoskeletal causes of movement disorders and other tics would be expected to trigger at least partially through mechanical factors, eg. positional posture.
The most efficient way to arrive at diagnostic acceptable certainty regarding compressive neuropathy as the cause of the disorder at hand, is to find a consistent mechanism that causes either inequivocal worsening or improvement of symptoms, every single time. Once the mechanism of induction of symptoms is identified, a treatment strategy can be employed. It is futile to render treatment strategies when no proven mechanism of symptom induction has been determined, as one is unaware of what is causing what one is attempting to treat!
For the jaw, I tend to ask the patient questions regarding any history of TMD symptoms, such as clicking in the jaw joint, temple or facial pain, or jaw joint pain. I also ask if their symptoms change (better or worse) with a lot of talking or chewing. I then try to worsen or improve their symptoms, first with jaw compression (retraction of the mandible, as this increases joint compression) — look for timely worsening, or transient improvement (due to nerve numbness) followed by aggressive worsening (minutes or hours later). If the symptoms are already bad, I may try decompression first, which is simply slight protraction of the mandible. Hold it there for at least 15 minutes (sometimes this might not suffice), look for decrease in symptoms. As mentioned, improvement or worsening would suggest that the symptoms are influenced by the jaw, which enables you to know what to start treating. If compression / decompression does not influence the symptoms, or the patient’s history simply does not suggests a joint origin (I usually check anyway), then consider the upper neck or lateral pterygoids. A TMJ MRI may frequently show articular disc thickening, disc subluxation or condylar deformation and flattening.

Figure 4: Bent and flattened condyle with posterior subluxation of the artiuclar disc
The lateral pterygoids will usually feel a little better after working them, but then get worse the day after. In very aggressive cases, the symptoms can come days after doing the exercise and here it is important to NOT increase the load until one is sure, to avoid future nuclear storms. Either way, perform the lateral pterygoid exercise carefully, as instructed in my TMD article and look for improvement or worsening.
If the jaw does not seem to be involved, then consider upper neck. Upper neck is as common, if not more common as a culprit of these disorders. Look for chin tucking and weak neck-throat angles (fig. 5, right) and, in grown men, prominent adam’s apples. Don’t pay attention to the fat, look at the angle and an apparent mimicking shortness of the mandible. These are all indications of extremely poor upper neck postures. Place the patient into the cervical hinge, and pull the chin down and back, without making the neck long (“long neck” increases the space for the nerves, (Larsen 2018)). See if you can induce worsening during or after the test. If the patient gets better in this test position, it is usually because you’ve made the nerves numb, and it will come back with a vengeance afterward. Do not mistake this for genuine improvement, as holding this position will make things much worse. Now, the “long neck” position as I teach in my atlas article (link) and also as seen on youtube, will distance the styloid from the C1 transverse process and thus decompress the nerves. Look for improvement. Position may need to be held for some time until improvement is seen, not everyone will see immediate effects. A CT scan, best done without a head pillow, will show narrowing of the atlantostyloidal interval. A head MRI can visualize the transverse process, which is helpful, but does not reliably demonstrate the styloid.
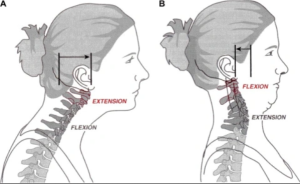
Figure 5: Chin tucking will worsen this condition as it draws the styloid process towards the C1 lateral mass
As said, improvement or worsening by specific protocols would implicate the region of interest in the mechanism of induction of symptoms, which is crucial information when attempting to solve syndromic mysteries such as these.
Case 1:
Oromandibular dystonia. A 45 yo. male patient contacted me for strange syndromic behavior that he claimed worsened in certain postures. The symptoms were described as uncontrollable mouth opening and closing with tongue protrusion that could go on for hours and even days, making me suspect some sort of myoclonic disorder. He said he would wake up better, but through the day or during stress, especially during exercise, his symptoms would flare. He was okay when the consultation started, so I wanted to find a specific way to trigger his symptom. If, and I wasn’t sure, they were mechanical, then the right trigger should be possible to find. The patient had no imaging done and had no diagnosis. He told me that no one had any idea what was going on with him, but it seemed strange to me that not even a brain MRI had been done.
Regardless, I suspected cranial nerve compression simply based on the description of his symptoms. I asked him to clench and grind his jaw, and open it repeatedly. This didn’t seem to cause any improvement nor worsening of symptoms. I then had him hinge on his neck and tuck backwards, as this draws the c1 transverse process and styloidprocess together and increases, if present, the compression of the jugular vein and its accompanying nerves. I had him hold the position for 90 seconds. Within a minute after performing this test his symptoms aggressively reproduced and would continue throughout the rest of the session; aggressive and bizzarre. His plastysma muscles also started spasming, suggesting affection of the hypoglossal and facial nerves predominantly, considering the tongue protrusion, plastysmal and supra-hyoidal muscle myoclonias.

Figure 6: Oromandibular dystonia triggering aggressive after the cervical tucking test.
Case 2:
Sudden, “out of the blue” onset of Tourette’s lik tics after prolonged iPad use while a 8-year old autistic child was living with his grandmom. The symptoms started with mild repeated utterances such as “uh” with head jerking, and uncontrolled swallowing. It then progressed to throat clearing and coughing, and then more aggressive body movements. He had been diagnosed with Tourette’s syndrome. I checked the boy’s jaw muscles for excessive tension, both the suprahyoids, masseter and temporalis muscles, but they seemed fine. He also had no clicking in the jaws nor any complaints of TMD, but again, he was young, and sometimes the TMJ is asymptomatic in these patients. I moved on to palpate the upper neck, and could feel the right transverse process of the atlas being situated excessively anterior compared to the opposite side. This was somewhat surprising, because the boy was young, physically healthy and and no known history of neck injury nor hypermobility. He didn’t seem hypermobile to me. It is possible that he has hurt his neck without the parents knowledge. I corrected his neck posture and taught his parents how to replicate it, and started him on exercises for the suboccipitals and levator scapulae muscles. The parents provided me a photo of his iPad use position, and it was exactly the hinge-neck position I use for provocation of these cases. I set him in this position for 10 minutes, and his tics reproduced and remained refractory for the next three days. I told the patients to be careful not to allow him time in that position and to do his exercises twice per week. Over the course of the following three months I saw them three times, and the symptoms gradually decreased until they disappeared. He would still get sporadic recurrence of symptoms if they let him stay on his iPad with poor posture, but it would again disappear with reimplementation of the protocol.
Case 3:
A 39 yo. female patient and her husband visited me for her refractory cervical dystonia. The left sternocleidomastoid muscle was affected, and her head was completely turned to the right. The muscle was palpably engaged and spasmic, and had been this way for the last three years. I asked her about history of jaw tension, popping or pain, but she denied this. She had already tried some dental treatments cf. what had been a popular topic for discussion on online social media groups for cervical dystonia, but this had not relieved her sympoms at all. Now, any type of dental treatment will not be guaranteed to work for this problem, it must be a treatment that decompresses the joint. Regardless, she also had no symptoms of TMD and she denied worsening of symptoms with chewing or prolonged talking. She did say, however, that falling asleep in awkward neck positions would make it worse and sometimes, certain positions might make it better, but she was unable to find a clear pattern. I looked at her neck posture and witnessed a conspicuous “neck hinge” with a weak chin to throat angle, usually suggesting that the patient’s head is resting overly posteriorly. Had brain MRI showed the transverse process anterior to the jugular foramen on a vertical line. In cases like this, it is often difficult to see immediate results, but in this case we were.
I had to forcibly place her into the proper cervical position, and within about a minute the contraction of the left sternocleidomastoid muscle would cease. I let her go back into her hinge-neck posture, and it would return, every single time. I attempted to teach the husband how to perform the correction, but it was difficult for her to hold. I also provided exercises for the suboccipitals and levator scapulae. In a case like this, a followup CT and potential styloidectomy and transversectomy to liberate the nervous impingement would be best. That said, for very motivated patients, the conservative protocol can definitely ameliorate this problem, as shown in my upper cervical article that was linked previously in this article.

Figure 7: A weak chin-throat angle is usually mislabled as double chin or just poor genetics. The mandibular length can certainly be genetic, and can also come secondary to poor craniofacial development during childhood. However, the chin-throat angle is a postural phenomenon and suggests cranial retraction on the upper neck.
Case 4:
Mild Tourette syndrome resolved within minutes of mandibular protraction. A 23 year-old tennis player came to me with elbow pain, but also said that he had mild Tourette’s disorder that manifested in arm tics. It was fairly mild and did not cause dramatic limitations to his life nor quality of life. I had no imaging, but I asked him about triggers and factors of improvement. He said that stress was a common precursor, but that a lot of talking and chewing could also trigger it. I did ask him about jaw symptoms as well, and he said that he had some clicking in both joints, but no pain. He also had ADHD. I suspected that the trigeminal nerve might be causing his tics and taught him how to decompress the jaw, which is, in essence, holding the jaw forward. Within a minute his tics were completely gone. He was hesitant to believe it at first, and put his jaw back into a retracted position. I told him to push the jaw back with force. This made the symptoms even worses than they were initally, confirming my suspicion. Once we pulled the mandible forward again, ie. decompressed the temporomandibular joint, within minutes, it went away.
Treatment
The treatment for these problems will depend on the cause. Identify the cause cf. my instructions above, and proceed with treatment of the temporomandibular joint, lateral pterygoid muscles or upper cervical spine as elaborated upon in the relevant articles that have already been reference in the main text.
References
- NIH, web article. Tourette syndrome. Available from: https://medlineplus.gov/genetics/condition/tourette-syndrome
- Deik A, Hurtig HI, Eichler AF. Cervical dystonia: Etiology, clinical features, and diagnosis. Wolters Kluwer publishing, 2023.
- Swain JE, Leckman JF. Tourette syndrome and tic disorders: overview and practical guide to diagnosis and treatment. Psychiatry (Edgmont). 2005 Jul;2(7):26-36. PMID: 21152158; PMCID: PMC3000195.
- Song WJ, Chang YS, Faruqi S, et al. European Respiratory Journal 2015 45: 1479-1481; DOI: 10.1183/09031936.00218714
- Sims A, Stack B. Tourette’s syndrome: a pilot study for the discontinuance of a movement disorder. Cranio. 2009 Jan;27(1):11-8. doi: 10.1179/crn.2009.003. PMID: 19241794.
- BEYERS, TEICH S. MANDIBULAR JOINT NEURALGIA (COSTEN’S SYNDROME). AMA Arch Intern Med. 1952;90(3):389–391. doi:10.1001/archinte.1952.00240090110009
- FREESE AS. Costen’s Syndrome: A Reinterpretation. AMA Arch Otolaryngol. 1959;70(3):309–314. doi:10.1001/archotol.1959.00730040317004
- Costen JB. I. A syndrome of ear and sinus symptoms dependent upon disturbed function of the temporomandibular joint. Annals of Otology, Rhinology & Laryngology. 1934 Mar;43(1):1-5.
- Larsen K. The true cause and solution for temporomandibular dysfunction (TMD). Web article, 2017. Available from: https://mskneurology.com/true-cause-solution-temporomandibular-dysfunction-tmd/
- Larsen K. Atlas joint instability: Causes, consequences and solutions. Web article, 2017. Available from: https://mskneurology.com/atlas-joint-instability-causes-consequences-solutions/
- Larsen K. Occult intracranial hypertension as a sequela of biomechanical internal jugular vein stenosis: A case report. Anaesth Pain & Intensive Care 2018;22(2):238-242
- Gweon HM, Chung TS, Suh SH. Evaluation of the Cause of Internal Jugular Vein Obstruction on Head and Neck Contrast Enhanced 3D MR Angiography Using Contrast Enhanced Computed Tomography. January 2011. Journal of the Korean Society of Magnetic Resonance in Medicine 15(1):41
My tongue can produce tinnitus a well as pressing my face or moving my jaw on the left side only.
Sometimes a getup with tinnitus and movement in inner ear.
Other days I getup with no sounds or pain or clogging in the ear
I was diagnosed with TMD 4 years ago and all the therapies are not fixing these symptoms.
What you do to diagnose what I have? and what treatments do you offer. I am in the USA