
Vestibular disorders are quite common, and largely considered idiopathic. It was estimated that up to 35% of the U.S. population above 40 years of age has vestibular dysfunction. It affects women up to three times more frequently than men (Neuhauser et al., 2005; 2007). Some of the more known types of vestibular impairment, are BPPV (benign positional paroxysmal vertigo), Meniere’s disease, vestibular migraines, idiopathic dizziness, cervicogenic dizziness, vestibular neuritis, car sickness, boat sickness, etc. Unfortunately, because these illnesses do not have an officially known etiology, proper testing may not exist. Agrawal et al. (2009) estimated that only 30% of patients with vestibular dysfunction would be diagnosed with the common tests which are used today. Further, the likelihood of acquiring one of the above problems increase with age, and is also greatly associated with diabetes mellitus as well as peripheral neuropathic disorders.
From 2001 through 2004, 35.4% of US adults aged 40 years and older (69 million Americans) had vestibular dysfunction. – Agrawal et al., 2009
Although vestibular disorders are common and often disabling, they remain difficult to diagnose and treat. – Lewis, 2015
The point of this article is not to repeat the well-known, but rather to reveal the lesser known yet common relationship between craniocervical dysfunction and the vestibular system. Naturally, this approach should be used when infections, tumors etc. have been excluded, i.e. when the condition is considered “idiopathic”. However, let us first briefly discuss how the vestibular system works.
NB: I have been planning to write this article for a while, but unfortunately I am very busy. Therefore it must be somewhat shorter (abbreviated) than priorly planned. I may fill in some gaps later on. Similar but more detailed information and associations between ear-dysfunction and TMJ / neck associations can be found in my tinnitus article.
The vestibular system and its function
The vestibular portion of the inner ear, also known as the labyrinth, consists of two otolith organs: The utricle and sacculus, which register linear movements (anterior, posterior, lateral, medial, up, down), and three semicircular canals which register rotational movements (yaw, pitch, roll), which are called the superior, posterior and horizontal semicircular canals.
Fig. 1: Vestibular system
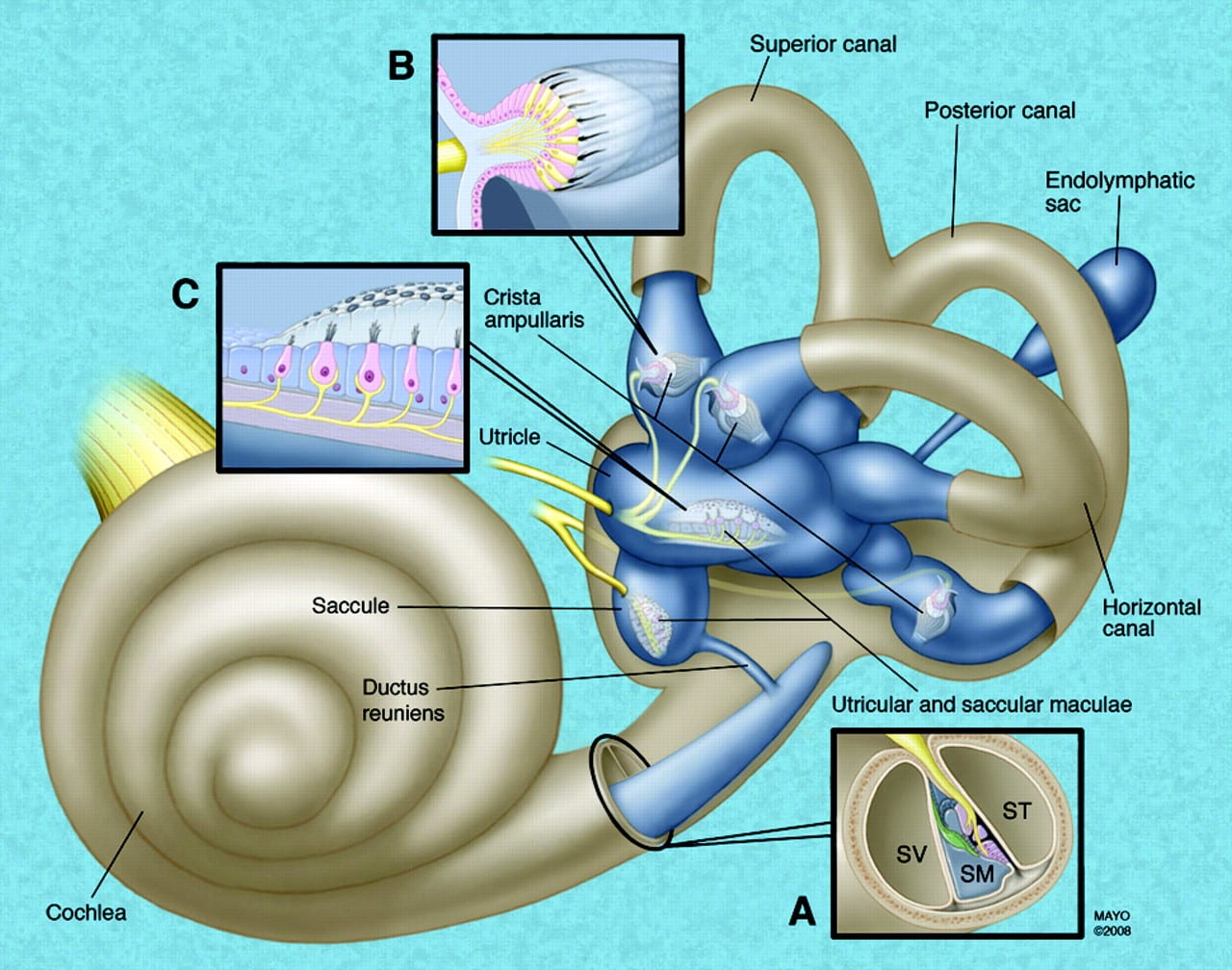
The otolith organs consist of a otolith crystals, the otolithic membrane and the stereocilia hair sensors. The otolith crystals are attached to the otolithic membrane, as showed below, and they move in accordance with gravitational forces as well as momentum. If someone pushes you forward, for example, the otolith & hair sensors would be pulled backwards, creating electrical signals translated from the body’s position and movement to your brain and thus allowing precise counter movement being organized in the cerebellum.
The sacculus register vertical (longitudinal) and lateral (coronal) movements, and the utricle register forward, backwards (sagittal) and lateral movements. Thus they both have a common ground in coronal movements, but are unique in perceiving longitudinal and sagittal movements. This is because the sacculus is aligned perpendicular to the utricle.
Fig. 2: Saccular and utricular motion organs
There are three semicircular canals, as mentioned already. The posterior canal registers pitch, which is a coronal axis rotation. The anterior canal registers rolls, which is a sagittal axis rotation. And, finally, the lateral canal registers yaw, which is a longitudinal axis rotational movement.
The hair sensors in the semicircular canals are stimulated a little differently than the otolith organs. All of the vestibular chambers are filled with endolymphatic fluids, just like in the cochlea, however the semicircular canals register movement of this fluid. During motion, the endolymphatic flow will move the crista hair cells and thus create signals according to which movements are occurring. These signals are then sent to the cerebrum for interpretation. The endolymphatic fluid is produced by the stria vascularis, which is the outer wall of the cochlear canal, as well as by dark cells within the labyrinth, located in the sacculus and utricle. It is also regulated by the endolymphatic sac, as well by the tympanic plexus. Improper endolymphatic regulation will influence balance, which we will discuss shortly.
The stria vascularis and vestibular dark cells are the two main structures responsible for endolymph secretion, and possess many similarities. The characteristics of these structures are the basis for regulation of inner-ear homeostasis – Ciuman, 2009
Fig. 3: Semicircular motion organs
Craniocervical factors that affect the vestibular system
Several factors, in addition to the obviously noted vestibulocochlear nerves (CN 8), may affect the vestibular system. Several studies show that intracranial hypertension (ICH), sudden intracranial hypotension (SIH), intermittent ischemia, venous congestion and nerve compression syndromes may dramatically affect function and interpretation of the vestibular chambers. Posture, muscle function and stress levels are all imperative factors to consider when treating vestibular dysfunction.
Thus, this article will expand upon these topics and explain the mechanism of dysfunction as well as how one may approach treatment.
Intracranial pressures / Venous congestion
Intracranial pressures are intrinsically related to vestibular function. The reason for this is that endolymphatic fluid levels are regulated through intracranial pressure (ICP) and proper drainage. The cerebral venous system does not have valves, as in the rest of the body, and is thus more sensitive to flow aberrancy. Thus, low pressure may cause vertigo, as may high pressures (Larsen 2018b, Soler 1998, Friedman 2014, Schievink 1996, 2000). Longstanding ICH may lead to dural perforation (especially in susceptible patients, such as those with Ehler-danlos syndrome (EDS)) with concomitant CSF leakage and sudden intracranial hypotension (Higgins 2015). Mokri (2002) showed that patient swho had their proven CSF leak fixed, developed hypertension, paradoxically suggesting that the two are associated. Further, longstanding ICH may also cause [secondary] endolymphatic hydrops (Ranieri 2017), a known pathology associated with Meniere’s disease, hearing loss and vertigo.
Fig. 4: Proximity of the IJV and CN9-12 to the transverse and styloid processes
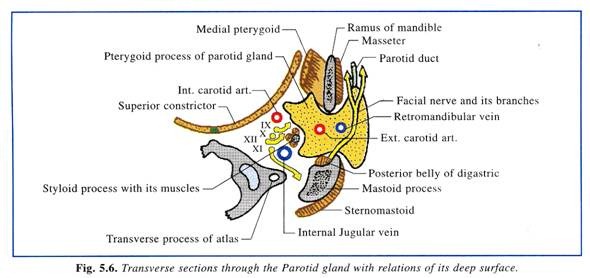
Fig. 5: Interscalene triangle & costoclavicular space
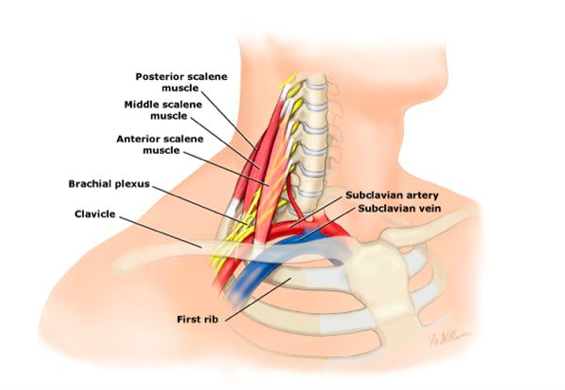
The most common cause of idiopathic intracranial hypertension is poor posture. I have named it biomechanical intracranial hypertension (Larsen 2018b). The reason for this, is that droopy shoulders may often lead to compression of the distal subclavian artery (SA) (weak and tight scalenes may as well). Distal SA obstruction will force blood redirection toward the carotid and vertebral arteries, thus saturating the cerebrovascular system. As a second but perhaps more important problem, is that hinge-neck postures as I have described in many of my articles (atlas, migraine), may cause blockage of the internal jugular vein, which is the main venous drainage from the cerebrum. This may occur as the vein is blocked between the styloid process of the cranium and the transverse process of the C1 (Larsen 2018b, Gweon 2011, Dashti 2012, Higgins 2015), and/or wrapped around the transverse process (TP) (Flanagan 2014) as the patient hyperextends their head in posture. Jayaraman et al. showed that extracranial IJV obstruction was coincidentally present in 33% of came into their department for angiography (the latter being negative, and the patients were deemed healthy), indicating that its prevalence is much higher than anticipated. Either way, drainage will be impaired, and the pressure will build up. More so, if the subclavian artery is obstructed as well. Increased inlet yet obstructed outlet is a recipe for intracranial hypertension, and may result in many maladies, some of which being endolymphatic hydrops, vertigo, chronic fatigue, migraine, tinnitus, hearing loss, vision impairment or even blindness (Corbett 1982, Jayaraman 2012).
In many circumstances, the IJV obstruction may be unilateral. Some practitioners may argue that unilateral obstruction is not a big problem, as compensatory drainage occurs through the contralateral sinus and IJV. However, studies show that also unilateral obstruction may still be clearly symptomatic (Cumurciuc 2005; Hyun-Ah Kim 2008; Thandra 2015; Zhou 2017).
Fig. 6: Compression of the internal jugular vein between the SP and C1 TP. Source: Gweon et al. 2011
Fig. 7: Axial MRI: Large forward atlanto-occipital subluxation of the C1 in a patient with longstanding vestibular dysfunction and ear “fullness”
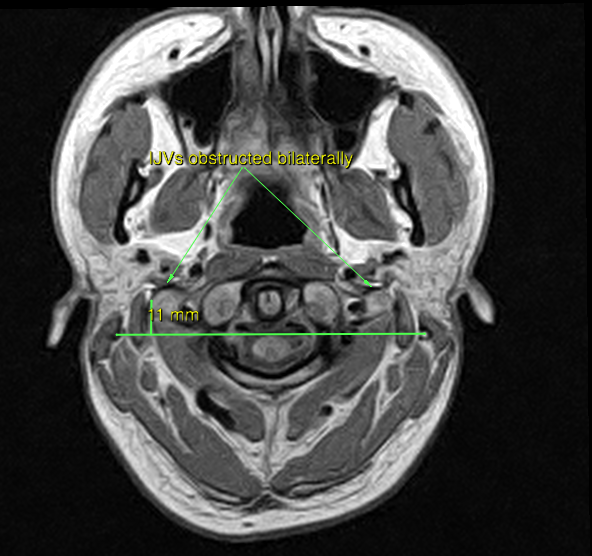
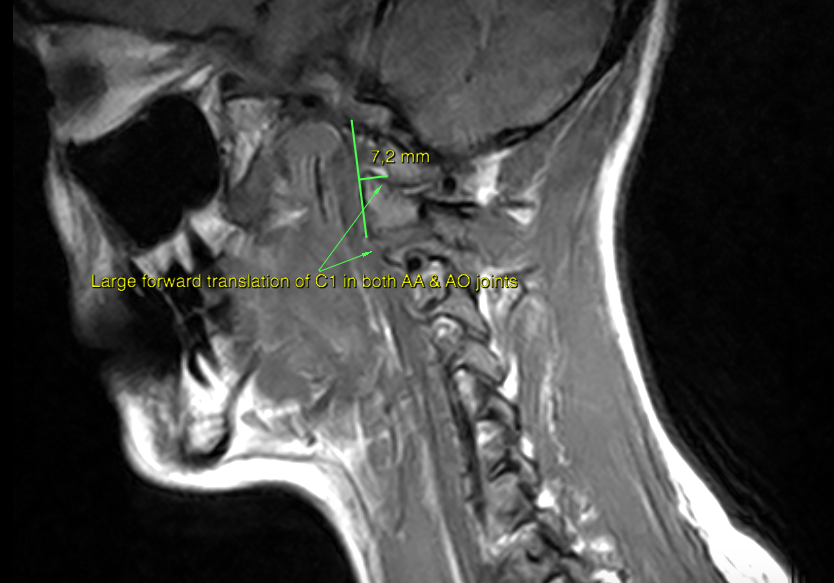
Fig. 8: Sagittal MRI: Conspicuous forward subluxation
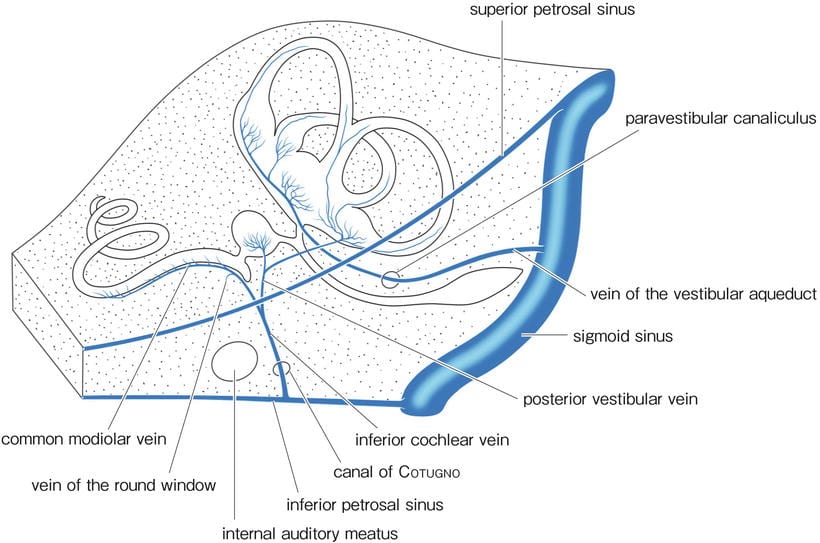
Endolymphatic fluid is drained out from the ear via the vein of the vestibular aqueduct, and into the sigmoid sinus. As stated, there are no venous valves in this system and thus adequate pressures are needed to maintain fluid balances. If the venous outlet is blocked of the system is saturated, especially the first-mentioned or both in tandem, endolymphatic drainage will be greatly impaired and may even retrogade. This leads to longstanding pressure buildups within the vestibular as well as cochlear chambers, with mentioned sequelae of hydrops etc. A common surgical intervention is to remove the endolymphatic sac, a regulative organ for endolymphatic fluid. However it is my impression that endolymphatic “overproduction” from the endolymphatic sac is extremely unlikely to cause such massive amounts of fluid that hydrops occurs. An utterly blocked outlet, potentially with retrogade flow is a much more likely culprit.
Fig. 9: Inner ear’s venous drainage
It has been documented that ICH and SIH may often be an occult disorder, where lumbar puncture opening pressures (LPOP) are normal despite clear symptoms of ICH. Thus one may not solely rely on LPOP for diagnosis of ICH and SIH. MRI criteria for SIH and ICH must be evaluated thoroughly for each case. MR or CT venography for evaluation of venous integrity should be performed (Higgins 2015, 2017; Larsen 2018b; Mokri 1997; Schievink 1998).
Generally, the problem may be ameliorated by improving cervical and scapular postures, as to decompress the IJV and SA. If the atlas has subluxed significantly forward, strengthening exercises that prevents anterior translation of the C1 will be done. The most important exercises are those for the longus capitis and levator scapulae.
Migraine-associated vertigo has become a well-recognized disease entity diagnosed based on a clinical history of recurrent vertigo attacks unexplained by other central or peripheral otologic abnormalities, which occurs in the patient with a history of migraine headaches. – Cha, 2010
The inner ear fluids play a major role in the cochlear and vestibular physiology by the transmission of the mechanical stimulus to the hair cells, on the one hand, and by the transduction of this signal to a nerve potential, on the other hand. – Ferrary & Sterkers, 1998
It has also been shown that, the distal portion of the endolymphatic sac, although it may be large in size may not have any discernable confluent area within it and that it may also overlap the sigmoid sinus (Friberg et al, 1988). There is a thickening of the dura mater around the endolymphatic sac which extends to the sigmoid sinus, beyond the end of the sac itself – Locke, 2008
The endolymphatic sac responds to endolymph volume disturbance, showing opposite responses to volume increases and decreases. Although evidence is still limited, the endolymphatic sac appears to act as a “bidirectional overflow” system. While volume disturbances originating from out-of-balance transport processes anywhere in the labyrinth may be corrected by the sac, dysfunction of the sac itself is likely to have a substantial effect on endolymph status – Salt, 2001
Vertebrobasilar insufficiency
Another relatively common cause of vestibular dysfunction, yet often one that is occult (hidden), is positional vertebrobasilar insufficiency. It is well known that vertebral artery injuries may result in immediate vertigo. It is less known, however, that intermittent obstruction of the VAs may cause chronic yet periodic vertigo in absence of concrete VA injury. It may also cause migraines, vision impairment, etc.
Fig. 10: Vertebral artery course and segments
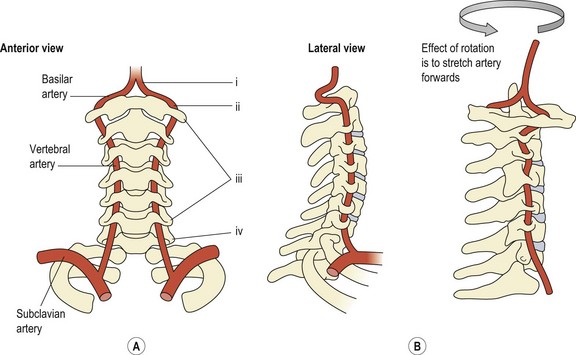
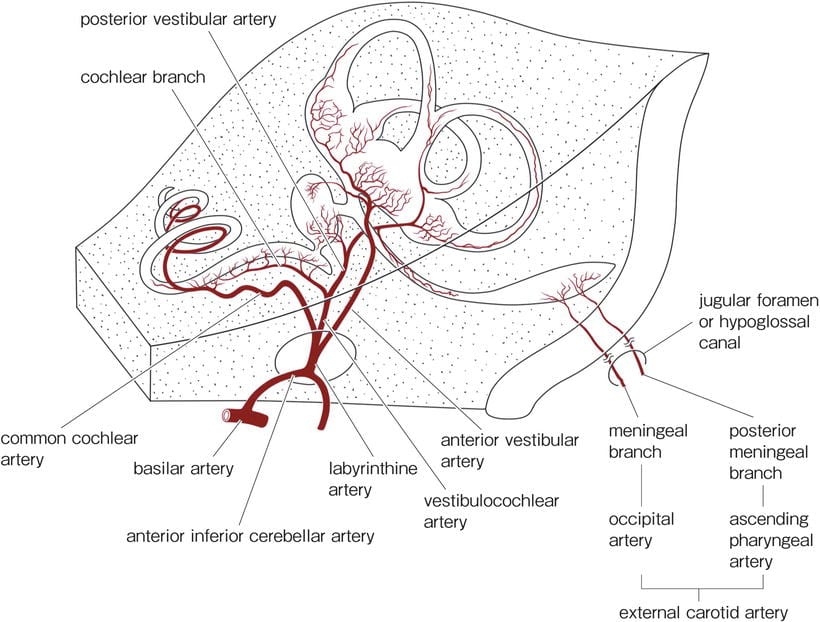
The vertebral arteries arise from the subclavian artery, runs through the transverse foramen between C6-C1, then enters the cranium to form the basilar artery. The basilar artery supplies the cerebellum, then connects to the posterior circle of Willis (COW). However, it also supplies the ear via the labyrinthine arteries. It is very common that one of the arteries are underdeveloped (hypoplasia), where the right artery is usually smaller than the left one (left dominant VA) (Pellerito & Polak 2012). The labyrinthine arteries carry a small yet crucial blood supply to the inner ear, and it has been documented that the inner ear is very sensitive to ischemia (Nuttall 1999b; Wangemann 2002b). Further, intermittent cerebral ischemia may also lead to vertigo on its own, as dizziness is a known pseudostroke symptom (Tehrani 2014).
Fig. 11: Inner ear’s arterial supply
It has been shown many times that biomechanical obstruction of the vertebral arteries may occur. It is commonly seen in patients with thoracic outlet syndrome, as the scalenus anticus may compress the VA if it branches off the posterior side of the subclavian artery (Powers 1961). It may also become compressed between the scalenus anticus and the longus colli, at the scalenovertebral angle (Kojima 1985). Osteophytic development within the vertebral foramen, or even laterally protruding disc herniations may also compress the arteries. There have been reports of migraine and transient blindness occurring with rotation, where a tight scalenus anticus have ben found as culprit with dynamic angiographic examinations (Sell 1994, Saxton 1998). Positional blockage of the VA has also been found with ultrasound doppler examinations in the DeKleyn’s position, despite angiography being normal (Arnetoli 1989). However, dynamic examinations of the VA is rarely performed, and the patient will be told that their hemodynamics (blood flow) are normal as the pathology is intermittent, positional and occult.
Typical symptoms of TOS are pain between the shoulderblades, arm pain, carpal tunnel syndrome, radial neuralgia, migraines, neck pain, chest pain, breathing pain, and more (Larsen 2018b; Selmonosky 1982, 2002, 2008)
Thoracic outlet syndrome may be ameliorated by strengthening the scalenus anticus and medius carefully, along with postural changes. Bow hunter’s syndrome may somewhat be ameliorated by strengthening the suboccipitals, as they prevent excessive C1-2 movement. However, fixation may be necessary in extreme circumstances. Disc herniations and/or osteophytic development within the transverse foramen may be surgically removed. In such case, a significant decline in systolic speeds will be noted upon doppler ultrasound of the vertebral artery (V2) between one foramen to the next (if a lesion is present).
BPPV can occur secondary to various other conditions including viral neurolabyrinthitis, Meniere’s disease, and vertebrobasilar ischemia [137]. In Meniere’s disease, it has been suggested that hydropic distension or rupture damages the otolithic apparatus, leading to the release of otoconia debris which migrate to the semicircular canals where they may result in BPPV [138]. Although BPPV is one of the most common causes of vertigo, it is not the only disorder associated with recurrent vertigo. Meniere’s disease, migraines, vertebrobasilar insufficiency, and panic disorder are also characterized by recurrent episodes. Caution in diagnosis BPPV is warranted as other conditions can present with BPPV-like symptoms. For example, central vestibular disorders can give rise to positional nystagmus, which can be mistaken for BPPV. Such lesions can arise from posterior fossa such as from small cerebellar strokes [131]. In inner ear pathologies which may cause vestibulopathies, such as perilymph fistulas, nystagmus may be enhanced by Dix-Hallpike testing. Furthermore, as spontaneous nystagmus associated with a perilymph fistula improves, nystagmus toward the affected ear in the downward position may misdirect the examiner from the initial pathological trigger of the symptoms. – Parham, 2014
This theory is supported by the strong correlation of hydrops with Meniere attacks, the finding that autoregulation of cochlear blood flow is impaired in the hydropic ear, and studies demonstrating that symptoms and signs in people and in animal models vary with conditions that alter perfusion pressure in the inner ear. Induction of Meniere attacks in animal models requires both hydrops and a mechanism that reduces perfusion pressure, such as epinephrine injection or head dependency. There is a strong clinical association between Meniere attacks and disorders that increase the risk for cerebrovascular ischemia, such as migraine. – Foster & Breeze, 2013
Thoracic Outlet Syndrome (TOS) causes dizziness because of positional compression of the vertebral artery with resultant symptoms of vertebrobasilary insufficiency. Compression of 7,C8,and T1 nerves fibers is responsible for the neck pain. – Selmonosky, 2007
The cases of 17 patients with vertigo, tinnitus, deafness, supraclavicular bruit, and a diminished radial pulse are reported. All the patients had an anomalous vertebral artery. All had subclavian-vertebral arteriograms preoperatively. Each patient showed an anomaly of the vertebral artery system which allowed intermittent compression of either the origin or cervical course of the artery. The compression was usually aggravated by rotation or hyperextension of the neck. In most cases, the vertebral artery arose at the level of the thyrocervical trunk and the compression was relieved by section of the scalenus anticus muscle and by division of the inferior thyroid artery. – Powers et al., 1961
We report a patient who developed occasional vertigo when turning his head to the right side. Occlusion of the right vertebral artery occurred at the narrowed “scalenovertebral angle” with this rotational head movement. This triangular tunnel consisted of the hypertrophied ligament of the longus colli muscle and the anterior scalene muscle. – Kojima et al., 1985
Rotation-induced vertebrobasilar artery hypoperfusion causes transient ischemic attacks (TIAs), affecting the cerebellum, brainstem and spinal cord. When these symptoms occur transiently due to head movement, compression of the vertebral artery by an extraluminal lesion should be suspected. Cervical spondylotic spurs and anterior scalene muscle or deep cervical fascia are among the factors which can compress the vertebral artery. – Dadsetan & Skerhut, 1989
Rotational positioning of the head showed vertebral obstruction in one direction, and unobstructed filling of the vessel when the head was turned to the opposite side. Fifteen patients showed rotational vertebral artery occlusion. The site of obstruction occurred at the origin of the vertebralartery or cephalad to the level of C5. Two patients had bilateral fascial band obstruction, one patient had left only, and the remaining 10 were obstructed on the right side. An anterior scalenotomy was done with preservation of the phrenic nerve. We were more impressed with the deep cervical fascia as the cause of intermittent rotational obstruction rather than the anterior scalene muscle. Only two patients showed unequivocal poststenotic dilatation as evidence of severe anterior scalene muscle compression. The obstructing extra-luminal fascia was quite dense, fibrotic and often completely encircling the artery. – Hardin & Poser, 1963
Subclavian steal symptoms presents secondary to arterial insufficiency, created by a retrograde flow that “steals” blood from the brain circulation, more specifically from the basilar artery via the vertebral artery. Classically it presents with neurological symptoms from the posterior brain and cerebellum [4,6]. Decreased flow over the basilar artery gives rise to symptoms like lightheadedness, ataxia, vertigo, dizziness, confusion, headache, nystagmus, hearing loss, presyncope and syncope, visual disturbances, focal seizures, and in extremely rare cases, death [6–10]. However the vast majority of patients are asymptomatic and rarely require any intervention [3,5,11]. – Alcocer et al., 2013
This article describes migraine without aura since childhood in a patient with bilateral cervical ribs. In addition to usual migraine triggers, symptoms were triggered by neck extension and by arm abduction and external rotation; paresthesias and pain preceded migraine triggered by arm and neck movement. Suspected thoracic outlet syndrome was confirmed by high-resolution bilateral magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) of the brachial plexus. An unsuspected aberrant right subclavian artery was compressed within the scalene triangle. Left scalenectomy and rib resection confirmed the MRI and MRA findings; the scalene triangle contents were decompressed, and migraine symptoms subsequently resolved. – Saxton et al., 1999
Thoracic outlet syndrome (TOS) refers to the compression of the neurovascular bundle within the thoracic outlet. Cases are classified by primary etiology-arterial, neurogenic, or venous. In addition to the typical symptoms of arm swelling and paresthesias, headaches have been reported as a potential symptom of TOS. In this report, we describe a patient with debilitating migraines, which were consistently preceded by unilateral arm swelling. Resolution of symptoms occurred only after thoracic outlet decompression. Patients with migraines and concomitant swelling and/or paresthesias, especially related to provocative arm maneuvers, should be considered a possible atypical presentation of TOS and evaluated in more detail. – Chahwala et al., 2017
It is also noteworthy that the hypertrophied and contracted anterior scalenus muscle exerts a strong although intermittent compression of the vertebral artery, causing in severe TOS diverse symptoms that are very characteristic of vertebrobasilary insufficiency. – Silva & Selmonosky, 2011
Reports of transient blindness resulting from this condition are even more rare. The authors describe the case of a middle-aged woman who presented with transient blindness when she turned her head excessively to the left. She also exhibited other less severe brainstem symptoms. Arteriography demonstrated occlusion of the left vertebral artery only when her head was rotated to the left. Surgical exploration revealed entrapment of the left vertebral artery by a tight anterior scalene muscle, release of which resulted in complete resolution of her symptoms. – Sell et al., 1994
Nerve entrapment syndromes
It is commonly thought that vestibular dysfunction is attributed to vestibular nerve impairment. “Vestibular nerve neuritis” is a common yet generic and often false diagnosis. It may as well be called “idiopathic dizziness”. It must be understood and considered the tympanic plexus is also greatly involved in regulating vestibulocochlear function. Many nerves contribute to the tympanic plexus, which may also be irritated in the neck and temporomandibular joint. This is why patients with neck and jaw disorders have a high prevalence of vestibular co-dysfunction, in my experience.
The tympanic plexus is formed by several nerves, namely the glossopharyngeal nerve, the facial nerve, and sympathetic fibers coming from the internal carotid plexus. However, it also communicates with the trigeminal nerve via the otic and pterygopalatine ganglia as well as the vagus nerve via the glossophargyneal nerve. It supplies the mucosa of the middle ear, the mastoid cells, the auditory tube, and parotid glands. – Barral & Croibier, Manual Therapy for the Cranial Nerves, 2009
Fig. 12: Tympanic plexus contribution
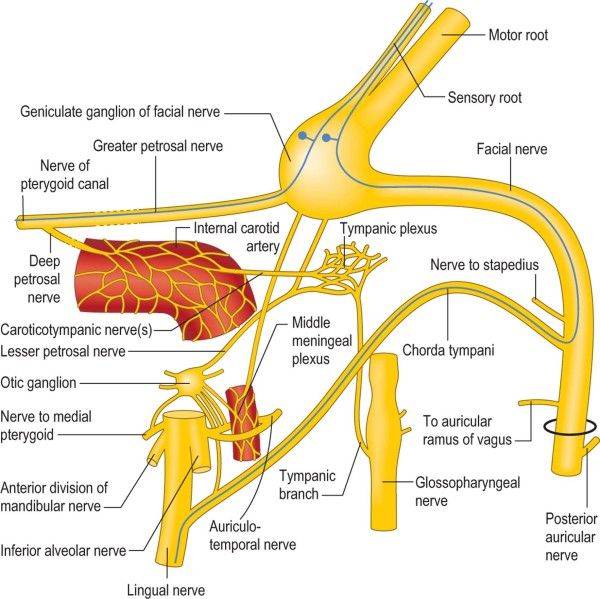
The tympanic plexus is involved in regulation of endolymphatic fluid levels, opening of the eustachian tube and thus also tympanic chamber pressures, the mucous membranes as well as mastoid air cells. When the nerves which contribute to the tympanic plexus are compromised, e.g. entrapped, this may cause faulty signalling to occur within the ear’s nervous network. The most common nerves to become compromised are the vagus nerve, sympathetic plexus and trigeminal nerves.
The glossopharyngeal nerve may become entrapped between the styloglossus and stylohyoid muscles. Further, it anastomosis with the vagus nerve. The vagus nerve transmits between the scalenus anticus and clavicular head of the sternocleidomastoid muscles, and may become entrapped here. It may also become compressed between the cranial styloid process and the C1 transverse process, as it passes between these structures in up to 66% of the population (Kim & Ledwitz-Rigby, 2014). One is especially predisposed to this problem with poor craniocervical postures and/or forward subluxation of the atlas (see my atlas article for more information). Vagus nerve entrapment will also often cause eustachian tube dysfunction, explaining why many patients with vestibular disorders also feel “fullness” of the ears or clogged” ears (Park et al. 2012). This resolves when the entrapment has been dealt with. Other symptoms include burning tongue syndrome, throat pain, “lumpy” throat, chronic or periodic idiopathic dry cough, excess hiccups (phrenic nerve), tinnitus, dysphagia (swallowing difficulty), itchy throat, ear pain, etc.
If the compression of the neurovascular bundle occurs at the atlantostyloid interval, this indicates that the atlas has come forward. It can also be a positional problem (Larsen 2018c). The patient must stop hinging at the neck and tucking their chin and follow the guidelines which I outlined above as well as. in my atlas article. If there is myofascial entrapment of the glossopharyngeal nerve within styloglossus and stylohyoid, the patient must stop clenching their hyoid muscles in posture. If it is vagus nerve entrapment between the SCM and scalenus anticus, strengthening of these muscles will be appropriate intervention. Once again, proper posture must also be maintained throughout the day.
Fig. 13: Oromandibular course of the glossopharyngeal nerve
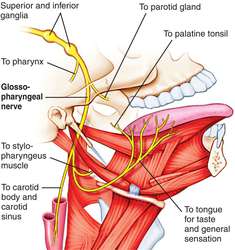
Fig. 14: Cervical course of the vagus nerve

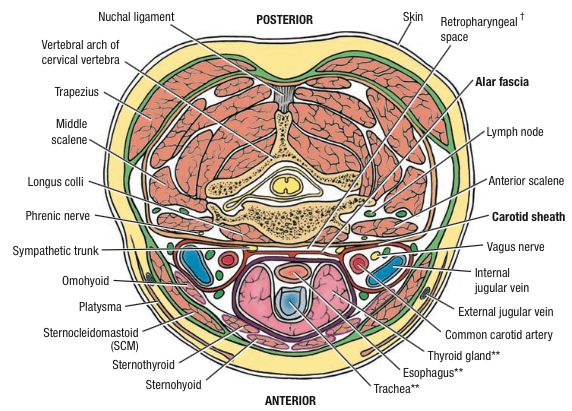
The sympathetic plexus contribute directly to the tympanic plexus. It may become entrapped between the cervical alar fascia and the longus colli & longus capitis muscles, causing diffuse symptoms of dysautonomia such as vestibular and vision impairment, tinnitus, itchy ears, ear clicking, eustachian tube dysfunction, etc. The superior cervical and stellate ganglia of the sympathetic chain has been implicated in Meniere’s disease (Franz 1998, 2007, Kang et al. 2005, Raj 2007), and I have personally (anecdotally) confirmed this association. Strengthening of the longus colli and longus capitis along with postural correctives are the main intervention for this problem.
Fig. 15: The sympathetic plexus transmits between the alar fascia and longii muscles
The trigeminal nerve (auriculotemporal branch) may become compressed between the mandibular condyle and TMJ fossa, hence its implication in TMD. It has been well documented that patients with TMD may struggle with symptoms of trigeminal neuralgia as well as vestibular impairment (Levandowski 2008). Further, several researchers have shown that the trigeminal nerve directly innervates the vestibular and cochlear chambers (Liu & Xu 2016; Vass 1998, 2001, 2004; Shore 2000) and that its stimulation may elicit vestibular dysfunction such as nystagmus (Marano 2005). The trigeminal nerve also innervates the tensor tympani muscle, whose dysfunction has been implicated in Meniere’s disease. Likewise, the facial nerve innervates the stapedius muscle. Tenotomy of the stapedius and tensor tympani muscles has been shown to greatly reduce vertigo and tinnitus (Franz 2003). However, are the muscles really to blame, or are they symptoms of compromised nerves? My impression is that the latter is true. In addition to vertigo and dizziness, trigeminal nerve compression may cause tinnitus, tremendous temple headaches, eye pain, palatine pain, tooth aches, cheek sensitivity, ear pain, etc.
Auriculotemporal nerve compression is a mechanical phenomenon and must be treated as such. Forward movement of the mandible in posture (see video below) as well as strengthening of the pterygoid muscles will ameliorate the situation as it causes mandibular protraction and thus TMJ decompression. The patient must also be assessed for whether or not they clench their suprahyoid muscles for neck stability (video below).
Fig. 16: Auriculotemporal nerve course posterior to the mandibular condyle

In support of the neural theory, the Barré-Liéou syndrome or posterior sympathetic syndrome has often been mentioned. Its mechanism is, however, uncertain and has been discredited, allowing misuse of this eponym [16]. This socalled posterior sympathetic syndrome has recently been challenged, as vestibulocochlear symptoms can be explained by the “anterior sympathetic” system comprising the superior cervical ganglion and its postganglionic neurons, with branches to the eustachian tube and inner ear [17]. Overall, evidence suggests that disturbances of the cervical spine can be associated with Ménière’s disease symptoms and that their adequate management can lessen inner-ear symptoms. – Franz & Anderson, 2007
The effect of novocain block on vertigo of Meniere’s disease. I have had the satisfaction of abruptly terminating two cases of Meniere’s disease during acute severe attacks by means of a procaine block. One case occurred at the Wembley Hospital. The patient was wheeled into the theatre lying curled up vomiting, with nystagmus, pallor and sweating. 5 ml. of procaine were injected in the stellate ganglion and within three minutes the patient had recovered sufficiently as to walk back unaided to the ward. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus
Superior cervical ganglion neurons project to the dilator pupillae muscle of the iris to control pupil dilation. Ocular blood flow is controlled both via direct autonomic influences on the vasculature of the optic nerve, choroid, ciliary body, and iris, as well as via indirect influences on retinal blood flow. – McDougal & Gamlin, 2015
It is generally believed that the cause of Meniere’s disease is related to autonomic dysfunction (Hilger’, 1950; Beickert’, 1953; Watanabe10, 1955; Hisaki’, 1960; Williams», 1965). The positive rate showing a response of either the sympathetic hyperreactor or sympathetic hyporeactor type in the cases with Meniere’s disease and aural vertigo was 79% and 87% respectively in the acute stage when nystagmus was present. – Uemura et al., 1972
MANDIBULAR joint neuralgia (Costen’s syndrome), first reported by Costen in 1934,1 is accepted by otorhinolaryngologists and members of the dental profession as a definite clinical entity. It should be considered in every differential diagnosis of recurring facial pain. – Beyes & Teich, 1952
According to the author’s hypothesis, the lack of posterior support of the alveolar ridge led to mandibular vertical height loss which caused a slipping backward of the condyles over the articular disc thus resulting in TMJ discal damage, erosion of the glenoid fossa bone, compression of the Eustachian tubes and tympanic plates and consequent impingement of the auriculotemporal nerve (ATN), which runs on the postero-medial aspect of the TMJ capsule, and chorda tympani nerve4 . – Paparo et al., 2008
Normal spacing between the roof of the glenoid fossa of the temporal bone and the condyle of the mandible should be approximately three mm to support the disk between them. The retrodiskal tissues originate from the distal portion of the glenoid fossa and are inserted into the posterior portion of the disk. This tissue contains a matrix of blood vessels and nerves, particularly fibers of the auriculotemporal nerve, cranial nerve V, an afferent branch of the trigeminal nerve. If this space is insufficient or reduced or restricted and the condylar head grows posterosuperiorly or is iatrogenically repositioned posteriorly or posterosuperiorly, the condyle will pinch this tissue and usually the result will be pain. – Sims & Stack, 2007
Our clinical work suggests that the auriculotemporal (AT) nerve, a branch of the mandibular nerve, the largest of the three divisions of the trigeminal nerve, plays a critical role in TMD sequelae. The AT nerve provides the somatosensory fibers that supply the joint, the middle ear, and the temporal region. By projecting fibers toward the otic ganglion, the AT nerve establishes an important bridge to the sympathetic system. As it courses posteriorly to the condylar head of the TMJ, compression, injury or irritation of the AT nerve can lead to significant neurologic and neuro-muscular disorders, including Tourette’s syndrome,Torticolli, gait or balance disorders and Parkinson’s disease. Subsequent irritation and compression of the AT nerve can occur, with associated parasthesia, pain and discomfort. Symptoms can be local and specific (e.g., TMD), as well as varied and systemic (e.g., neurologic, dystonic and neuro-muscular disorders, including tremors, muscle spasms leading to impaired and awkward positional control of the head, hands, other extremities, speech impairment, incontinence, impaired sleep, associated depressive symptomatology). – Demerjian et al., 2011
Anatomical relationships between the auriculotemporal nerve and the muscles of mastication, temporomandibular joint, and surrounding vessels in the area of the infratemporal fossa create favourable conditions for entrapment syndromes. Entrapment of the auriculotemporal nerve plays a role in the pathogenesis of temporomandibular joint pain syndromes, headaches, as well as pain symptoms or paraesthesias within the external acoustic meatus and auricle. Komarnitki et al., 2012
The syndrome of symptoms (Table 1) as first described by Costen, an American otolaryngologist, was discussed. Costen attributed the symptoms to temporomandibular joint dysfunction consequent upon mandibular overclosure with distal condylar displacement. He assumed that the displaced condyle might lead to any of the following: Compression of the eustachian tube, erosion of the glenoid fossa or tympanic plate, pressure on the chorda tympani, or pressure on the main trunk of the auriculotemporal nerve. – Clarke, 1962
Sectioning of the tensor tympani and stapedius muscle tendons significantly reduced the frequency and intensity of vertigo and improved both the functional profile and tinnitus. – Franz et al. 2003
Suboccipital dysfunction
The suboccipital muscles are a unique muscle group with a very high density of receptor cells. They are the most local stabilizers of the craniocervical junction, and have a muscle fiber configuration that allows them to move the head in all various directions. The reason for this, is that the suboccipitals synchronize the head with the eyes’ movements. If you palpate them while moving your eyes around, you’ll feel them pop up under your fingers, according to your ocular movement. Very interesting, indeed!
When they are adequately dysfunctional, meaning extremely weak, the patient may first experience dizziness during motion such as in the car or boat sickness. As the dysfunction progresses, the dizziness may become more pronounced. Weakness of the suboccipitals may also cause tremendous headaches and may mimic migraines. It may also cause excessive movement of the atlanto-occipital and atlantoaxial joints when overly lax / weak. I never recommend massaging these muscles; only strengthening. It is imperative to understand that weak muscles feel tight and are painful, and that this will exacerbate with continuous stretching, yet permanently resolve with proper strengthening. You can find exercises for these muscles in my atlas article and/or on my youtube channel.
Fig. 16: Suboccipital muscles

The distribution and arrangement of spindles within the muscle and their arrangement was studied. The spindle density of superior oblique muscle was found to be 190, that of inferior oblique was 242 and the rectus capitis posterior contained 98 spindles per gram of muscle. – Kulkarni et al., 2001
Muscle spindle density is extremely high in the deep muscles of the human neck. – Liu et al., 2003
Stress levels
Everyone knows that stress is an amplifying factor. However, a common tendency of people who are very stressed, scared, anxious etc., is that they hold their breaths and brace their bodies. I call this phenomenon “global involuntary clenching strategy” (GICS), where the patient is more or less constantly creating valsalva maneuver due to inability to handle stress. Constant valsalva will cause intracranial hypertension as well as muscle imbalances, and may therefore be directly linked to vestibular dysfunctions and not merely an amplifying factor. I will not elaborate upon this topic here, but rather you can read about it in my GICS article.
Within the poorly understood mechanisms implicated in the aetiology of benign paroxysmal positional vertigo (BPPV), the results of this trial provide clinical evidence of a potential role of emotional stress connected to adverse life events as a trigger of otoconial dysfunction. High levels of anxiety, depression and somatization were recorded and considered psychogenic precursors of BPPV, thus emphasizing the role of psychological distress in precipitating peripheral vestibular disorders. Therefore, appraisal of life stress and psychological attitudes may have potential implications in the clinical assessment of this labyrinthine vertigo and its frequent relapses. – Monzani et al. 2006
The postural common denominator
The importance of posture is a very controversial topic these days. However, I think it is counterintuitive to reject posture. Clearly, the way we hold ourselves greatly affect how we use our muscles. It’s not coincidental that patients with poor postures often have very painful muscles. However, we need to know the specifics of what good posture really is. I think the main reason that posture remains controversial, is the lack of very important nuances. Cues to “straighten the back” or “lower the shoulders” are detrimental as they discourage natural postural habits (Larsen 2018a, 2018b).
Loss of lumbar lordosis is causing patients to clench their abs in posture, inhibiting them from breathing properly. Stress exacerbates the poor breathing pattern, and sets them on course in an evil circle. Moreover, depression of the clavicles, which is very common, will promote hinge-neck postures as well as compression of the costoclavicular space (thoracic outlet syndrome) (Swift 1984, Telford 1948, Larsen 2018b). As I touched upon earlier, costoclavicular space compression (CCS) may compress the subclavian artery, redirecting more blood into the head. Hinge-neck postures may block the internal jugular vein, thus potentially creating a huge imbalance between arterial inlet and venous outlet, resulting in craniovascular saturation and intracranial hypertension.
Although many “sub-diagnoses” can be made, I sincerely believe that poor posture and stress are the main and fundamental causes of vestibular disorders. That said, once the malady has progressed and matured, both posture and proper corrective rehabilitation is required to reverse the problem.
Case example
Below is the case of a 45 year old woman who had sudden onset of vertigo. She has a history of several whiplash accidents and has suffered from both jaw and neck pain for many years, yet has been active and working throughout this time. She was initially diagnosed with vestibular neuritis, but as time went by she started to develop other cognitive dysfunctions such as dysarthria (speech difficulty), confusion, disorientation, facial numbness and left-sided transient facial hemiparesis (facial paralysis, also known as Bell’s palsy or seventh nerve palsy). She was nor able to say “R” nor hold a normal conversation, or even sign papers. She was admitted to the hospital and several examinations were performed, however no concrete pathology was found. Her MRIs were deemed “normal”, and she was sent home.
When she visited my office, she presented with a significantly poor posture, with very distended external jugular veins, indicative of intracranial hypertension. I set her in proper posture, and within two minutes she was able to pronounce “R” and look me in the eyes. Her colleague, which assisted her, confirmed that her ability to interact had improved on those minutes. This indicates that there is biomechanical compression of the IJVs (Larsen 2018c), or else she would not improve by postural alteration alone.
Later, going through the MRIs (I received these at her second visit), to my surprise, I saw clear signs of intracranial hypotension (low pressure), not hypertension. Either way, not so “normal” findings after all, as priorly stated by the hospital. I was also able to detect stenosis of the left IJV, which was caused by forward subluxation of the atlas. Ultrasound also showed hypoperfusion in the left IJV and hyperperfusion in the right IJV, as well as rounded systolic peaks of the left ICA and vertebral artery, which is compatible with her stroke-like symptoms as well as the MRI images. As stated earlier, long-term hypertension can cause SIH (sudden intracranial hypotension) (Higgins 2015). This is. what happened here. Her lumbar puncture opening pressure was. 11,5 cm H2O (ref: > 10). Clearly, with a blocked vein, one would expect higher levels than 11,5, unless there is indeed a leak. Such a sudden leak in the following of chronic venous congestion would explain the sudden onset of vestibular and cognitive impairment.
6 weeks after the postural correction and initiation of neck and jaw rehabilitation, she is once again able to hold a normal conversation, pronounce “R”, solve math puzzles, sign papers, her memory has returned, and last but not least, has a 95% reduction in dizziness. The CSF leak heals on its own once the IJV blockage resolved. This has also been documented by Higgins (2015). I presume that’s also what happened here.
Fig. 17: Signs of SIH

Fig. 18: Forward subluxation of the left atlanto-occipital joint, explaining fig. 19

Fig. 19: Left IJV stenosed at the atlantostyloid interval
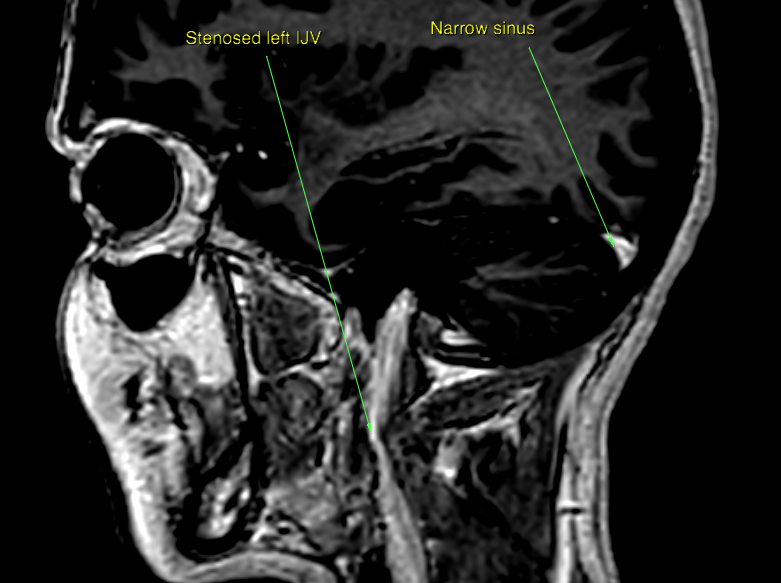
Fig. 20: Hypoperfusion (poor drainage) in the left IJV

Fig. 21: Relatively normal right IJV. There is a slight but insignificant stenosis here as well.

Fig. 22: High-pressure “splash-flow” in right IJV in attempt to compensate for left stenosis

Case #2 – Positionally conditioned
Below is a 38 year old woman with proven intracranial hypertension without known cause (“idiopathic”). She suffered whiplash in the early 2000. Her lumbar puncture opening pressure was 50cm H2O in 2003, and she was diagnosed with idiopathic intracranial hypertension. A shunt to drain out the excess CSF was installed, normalizing the ICP to around 15cm H2O. Her headache was somewhat ameliorated yet many symptoms persisted, and she was ultimately not able to continue working. She still had tremendous neck pain, perceived intracranial pressure with eye pain, and chronic headaches. Around 2015 it was postulated that it may be related to venous congestion, so she underwent CT venography, however this exam was negative. Then, in 2018 she sought a seated MRI examination abroad, which did not explain her symptoms either, except for indications of atlantoaxial instability.
Fig. 23: Falsely normal atlantostyloid interval and unobstructed IJVs because the patient didn’t lie in a way which simulated her natural posture.
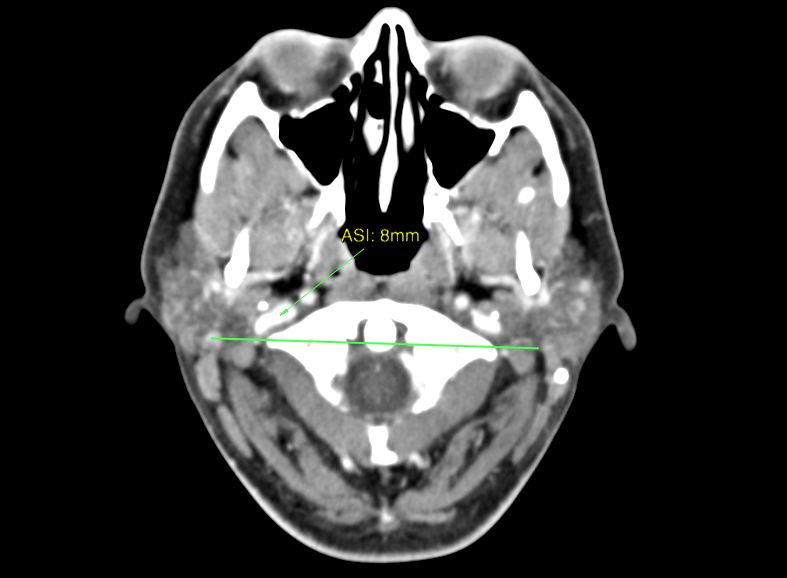
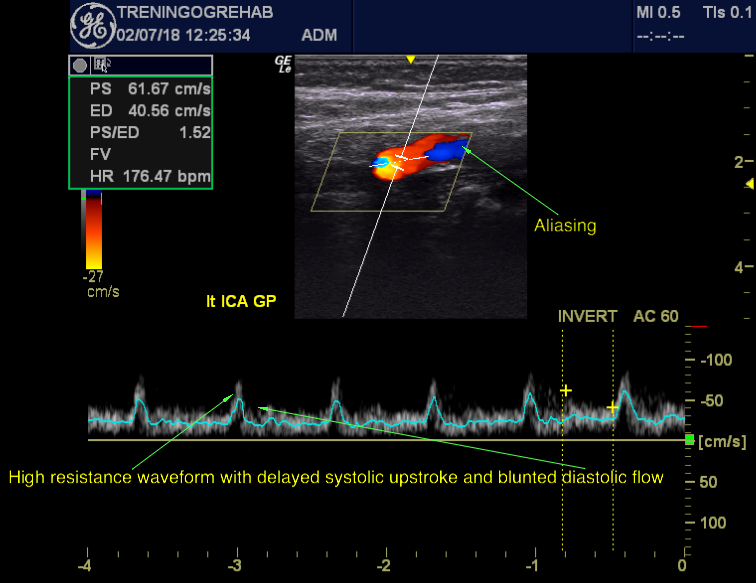
In person, the patient once again presents with very poor neck and shoulder posture, suggesting biomechanical IJV stenosis as a possible etiology of her problems. Due to the atlantoaxial instability, I examined her vertberal arteries with rotation (with ultrasound), but this test was unremarkable. Thus excluding arterial insufficiency as the cause of her remaining symptoms. Examination of the MRIs however show that there was still flattening of the posterior eye (global flattening), and concave partially empty sella (pituitary compression), which indicate the presence of ICH. Further, in opposition with the lying CTV, the upright MRI showed obliteration of the left internal jugular vein, and partial obstruction of the right one. Doppler confirmed these findings, and also showed slowed systolic upstrokes. Now, why would there still be evidence of ICH if the CSF is drained via the shunt? Because excess CSF is just a secondary symptom! The main problem here has been occult venous congestion since the problem’s genesis. Thus the CSF excess is a mere sequela of internal jugular vein stenosis. I set this patient in proper posture, which has reduced her symptoms considerably. We are also rehabilitating her neck and shoulder problems. As most patients with a history of whiplash and associated disorders (WAD), this patient also had TOS (thoracic outlet syndrome).
Fig. 24: Indicator of ICH (Osborn’s brain, 2017)

Fig. 25: Indicator of ICH (Osborn’s brain, 2017)
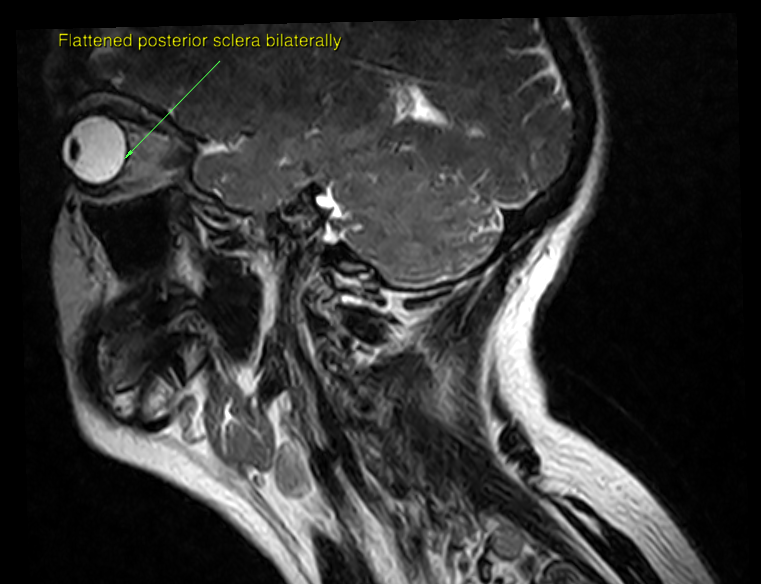
Fig. 26: Obstruction of IJVs in upright position with poor posture

Fig. 27: Atlantoaxial hypermobility
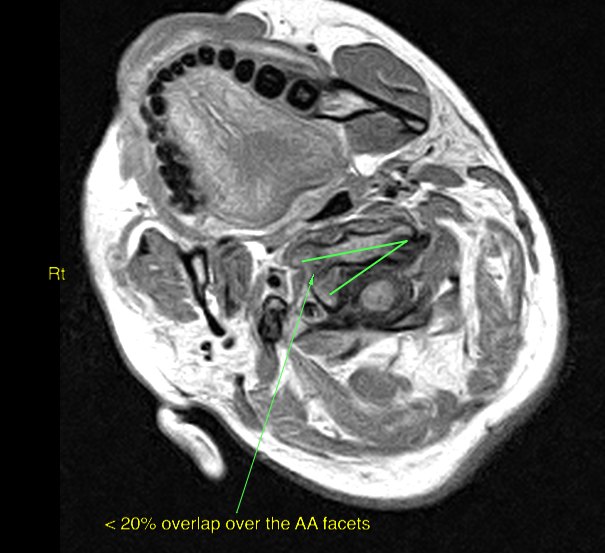
Fig. 28: Hyperperfusion (compensatory flow) right IJV

Fig. 29: Very slight perfusion in the left IJV with “good posture”

Fig. 30: However, zero left IJV perfusion when lying in her natural posture (“bad posture” or “BP”)

Fig. 31: Quite abnormal left ICA waveforms, yet the right ICA was more or less normal, compatible with the left IJV obliteration
This case is a good example of how patients with poor posture may have falsely negative CTV or MRV results when searching fore extracranial stenosis, if they are not lying down in their natural posture. As mentioned, extracranial stenosis is a little known yet common problem (Jayaraman 2012).
Treatment & detection
It takes time to get to the point of chronic vestibular dysfunction. The patient must be aware that the treatment is rough and that it is not a quick fix. First and foremost he or she must resolve their poor posture. The patient needs to learn to properly arch their lower backs in posture and to stop bracing, i.e. to stop holding their breath, clenching their abs and creating valsalva habitually. Moreover, they need to maintain a “long neck” position and raise their shoulders in posture, until the superior angle of the scapulae are leveled with the T2 vertebra (Osar 2012, Larsen 2018b, Larsen 2018c).
Poor posture for 16 hours and then 2 minutes of corrective exercise is a futile strategy and needs not be attempted. It is fundamentally necessary to practice proper posture AND supplement this with proper corrective rehabilitation of impaired soft tissues. The most important and commonly impaired muscles in vestibular disorders, are the longus capitis and colli, scalenus medius and anticus, suboccipitals, levator scapulae and trapezius muscles. Rehabilitation should be started with very, very light stimulus two-three times per week. Aggressive or even moderate strengthening may cause tremendous flareup of their symptoms. This is harmless, but unnecessary. Start easy, and gradually build the muscles up.
Intracranial pressures: Lumbar puncture opening pressures are known to be unreliable. The practitioner should not reject SIH or ICH based on a negative LPOP. Schievink (1998, 2000) which is one of the foremost researchers on SIH, states that LPOP is not needed to diagnose SIH, but rather, the physician should be guided by the appearance of the cerebral MRIs as well as the patient’s clinical symptoms. Imaging signs for ICH are such as, but not limited to: Flattened posterior globes with or without optic nerve bulging, optic nerve sheath distension, undulated optic nerve, [partially] empty sella, pons flattening, obliteration of the basal cisterns and cerebral sinuses, chiari, or “tight brain” appearance. Signs for SIH are such as, but not limited to: CSF-depleted tractus opticus, distended transverse and sagittal sinuses, < 50˚ pontomesencephalic angle, enlarged pituitary, brain sagging, chiari, basal cistern effacing, elongated midbrain, lateral ventricle narrowing, mamillopontine distance < 5,5 mm (Osborn’s brain, 2017).
Detection of venous blockage can be done through MRV or CTV (V=venography), but it is important that the patient lies with their natural cervical and scapular position during the examination. A seated examination is not necessary. Any arterial insufficiency, generally implying rotational insufficiency of the vertebral arteries, can be detected with a doppler scan with and without rotation of the neck. The patient will be scanned in the DeKleyn’s provocative position. However, it is important that the physician scans the V3 segment (the supraatlantal segment) and not the V2, in case of Bow hunter’s syndrome. In either case, a significant systolic decline with signal loss, tardus parvus waveform, or potential absence of flow will be noted. Confirmation should be done with dynamic MRA or CTA (A=angiography). Detection of stenosis via MRV or CTV (venography) is underutilized and under-appreciated, according to Higgins 2004. Most likely because IJV stenosis at the craniocervical junction is not a well-known problem. Similarly, there are few practitioners measuring the vertebral arteries with rotation of the neck.
As for rehabilitation of atlanto-occipital instability and/or nerve entrapment syndromes, these topics are too large to repeat once more, when I’ve written in lengths about them in other articles, such as my neck pain, thoracic outlet syndrome, temporomandibular joint disorder and atlas joint instability articles. Confer with these for rehabilitative protocols. The main scope of this article is to show WHY the neck and TMJ may greatly affect the vestibular system.
In conclusion
If no concrete findings or causes for vestibular impairment are found, such as tumors or similar, then craniocervical and TMJ involvement should be considered as a potential cause. Poor postures may cause chronic intracranial venous congestion with subsequent intracranial hypertension. It may also promote thoracic outlet syndrome, which as been implicated in intermittent vertebrobasilar insufficiency. Both of these problems are known etiologies of chronic vestibular dysfunction. Further, the nerves from the neck and jaw contribute to the tympanic plexus, and may thus be implicated in dysregulation of the middle and inner ear structures, as well as eustachian tube. Neck and jaw disorders are treatable and even curable with the right approaches.
References:
- Neuhauser HK, von Brevern M, et al. Epidemiology of vestibular vertigo: A neurotologic survey of the general population. Neurology. 2005;65(6):898–904.
- Neuhauser HK. Epidemiology of vertigo. Curr Opin Neurol. 2007;20(1):40–46.
- Agrawal Y, Carey JP, Della CC, et al. Disorders of Balance and Vestibular Function in US Adults. Arch Intern Med. 2009;169(10):938-944. doi:10.1001/archinternmed.2009.66.
- Lewis RF. Advances in the diagnosis and treatment of vestibular disorders: psychophysics and prosthetics. J Neurosci. 2015;35(13):5089-5096. doi:10.1523/JNEUROSCI.3922-14.2015
- Ciuman RR. Stria vascularis and vestibular dark cells: characterisation of main structures responsible for inner-ear homeostasis, and their pathophysiological relations. J Laryngol Otol. 2009 Feb;123(2):151-62. doi: 10.1017/S0022215108002624. Epub 2008 Jun 23. PMID: 18570690.
- Soler D, Cox T, Bullock P, et al. Diagnosis and management of benign intracranial hypertension. Archives of Disease in Childhood 1998;78:89-94.
- Friedman D. (2014) The pseudotumor cerebri syndrome. Neurol Clin 32: 363–396.
- Schievink WI, Meyer FB, Atkinson JLD. et al. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J Neurosurg. 1996;84:598-6058613851
- Schievink WI, Ebersold MJ, Atkinson JLD. Roller-coaster headache due to spinal cerebrospinal fluid leak. Lancet. 1996;347:14098637363Google ScholarCrossref
- Schievink WI. Spontaneous spinal cerebrospinal fluid leaks. Neurosurg Focus. 2000;9:1-9
- Mokri B. Intracranial Hypertension After Treatment of Spontaneous Cerebrospinal Fluid Leaks. Mayo Clin Proc. 2002;77:1241-1246
- Higgins N, Trivedi R, Greenwood R, Pickard J. Brain slump caused by jugular venous stenoses treated by stenting: a hypothesis to link spontaneous intracranial hypotension with idiopathic intracranial hypertension. J Neurol Surg Rep. 2015 Jul;76(1):e188–e193. doi: 10.1055/s-0035-1555015
- Ranieri A, Cavaliere M, Sicignano S, Falco P, Cautiero F, De Simone R. Endolymphatic hydrops in idiopathic intracranial hypertension: prevalence and clinical outcome after lumbar puncture. Preliminary data. Neurol Sci. 2017 May;38(Suppl 1):193-196. doi: 10.1007/s10072-017-2895-8. PMID: 28527079.
- Gweon HM, Chung TS, Suh SH. Evaluation of the Cause of Internal Jugular Vein Obstruction on Head and Neck Contrast Enhanced 3D MR Angiography Using Contrast Enhanced Computed Tomography. JKSMRM 15:41-47(2011)
- Dashti SR, Nakaji P, Hu YC, Frei DF, Abla AA, Yao T, et al. Styloidogenic jugular venous compression syndrome: diagnosis and treatment: case report. Neurosurgery. 2012 Mar;70(3):E795-9. doi: 10.1227/NEU.0b013e3182333859
- Larsen K. Occult intracranial hypertension as a sequela of biomechanical internal jugular vein stenosis: A case report. Anaesth Pain & Intensive Care 2018;22(2)
- Flanagan MF. The Role of the Craniocervical Junction in Craniospinal Hydrodynamics and Neurodegenerative Conditions. Neurol Res Int. 2015;2015:794829. doi:10.1155/2015/794829
- Corbett JJ, Savino PJ, Thompson HS, Kansu T, Schatz NJ, Orr LS, Hopson D. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982 Aug;39(8):461-74. doi: 10.1001/archneur.1982.00510200003001. PMID: 7103794.
- Jayaraman MV, Boxerman JL, Davis LM, Haas RA, Rogg JM. Incidence of extrinsic compression of the internal jugular vein in unselected patients undergoing CT angiography. AJNR Am J Neuroradiol. 2012 Aug;33(7):1247-50. doi: 10.3174/ajnr.A2953. Epub 2012 Feb 9. PMID: 22322614.
- Cumurciuc R, Crassard I, Sarov M, Valade D, Bousser MG. Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatry. 2005 Aug;76(8):1084-7. doi: 10.1136/jnnp.2004.056275. PMID: 16024884; PMCID: PMC1739763.
- Kim HA, Sohn SI, Lee H. Cerebral venous thrombosis mimicking acute unilateral vestibulopathy. Neurol Sci. 2008 Feb;29(1):41-3. doi: 10.1007/s10072-008-0858-9. Epub 2008 Apr 1. PMID: 18379740.
- Karaman E, Saritzali G, Cansiz H. A case of increased intracranial pressure after unilateral modified radical neck dissection. Am J Otolaryngol. 2009 Jul-Aug;30(4):261-3. doi: 10.1016/j.amjoto.2008.04.007. Epub 2008 Sep 21. PMID: 19563938.
- Thandra A, Jun B, Chuquilin M. Papilloedema and Increased Intracranial Pressure as a Result of Unilateral Jugular Vein Thrombosis. Neuroophthalmology. 2015 Jul 15;39(4):179-182. doi: 10.3109/01658107.2015.1044541. PMID: 27928352; PMCID: PMC5123161.
- Zhou D, Meng R, Zhang X, Guo L, Li S, Wu W, Duan J, Song H, Ding Y, Ji X. Intracranial hypertension induced by internal jugular vein stenosis can be resolved by stenting. Eur J Neurol. 2018 Feb;25(2):365-e13. doi: 10.1111/ene.13512. Epub 2017 Dec 7. PMID: 29114973.
- Higgins JNP, Pickard JD, Lever AML. Chronic fatigue syndrome and idiopathic intracranial hypertension: Different manifestations of the same disorder of intracranial pressure? Med Hypotheses. 2017 Aug;105:6-9. doi: 10.1016/j.mehy.2017.06.014. Epub 2017 Jun 24. PMID: 28735654.
- Mokri B, Piepgras DG, Miller GM: Syndrome of orthostatic headaches and diffuse pachymeningeal gadolinium enhancement. Mayo Clin Proc 1997, 72:400–413.
- Schievink WI, Morreale VM, Atkinson JL, et al.: Surgical treatment of spontaneous spinal cerebrospinal fluid leaks. J Neurosurg 1998, 88:243–246.
- Cha YH. Migraine-associated vertigo: diagnosis and treatment. Semin Neurol. 2010 Apr;30(2):167-74. doi: 10.1055/s-0030-1249225. Epub 2010 Mar 29. PMID: 20352586; PMCID: PMC5682200.
- Ferrary E, Sterkers O. Mechanisms of endolymph secretion. Kidney Int Suppl. 1998 Apr;65:S98-103. PMID: 9551441.
- Locke RR. Anatomy of the Transmastoid Endolymphatic Sac Decompression in the Management of Ménière’s Disease. The University of Glasgow Faculty of Biomedical and Life Sciences April 2008
- Salt AN. Regulation of Endolymphatic Fluid Volume. THE VESTIBULAR LABYRINTH IN HEALTH AND DISEASE October 2001. Volume942, Issue1. p306-312
- Pellerito J, Polak J. Introduction to Vascular Ultrasonography 6th Edition, 2012; Elsevier publishing.
- Nuttall AL. Sound-Induced Cochlear Ischemia/Hypoxia as a Mechanism of Hearing Loss. Noise & health. 1999b;2:17–32. [PubMed] [Google Scholar]
- Wangemann P. Cochlear blood flow regulation. Adv Otorhinolaryngol. 2002b;59:51–57.
- Saber Tehrani AS, Kattah JC, Mantokoudis G, Pula JH, Nair D, Blitz A, et al. Small strokes causing severe vertigo: Frequency of false-negative mris and nonlacunar mechanisms. Neurology. 2014;83:169–173.
- Powers SR Jr, Drislane TM, Nevins S. Intermittent vertebral artery compression; a new syndrome. Surgery. 1961 Feb;49:257-64.
- Kojima N, Tamaki N, Fujita K, et al: Vertebral artery occlusion at the narrowed “scalenovertebral angle”: mechanical vertebral occlusion in the distal first portion. Neurosurgery 16:672–674, 1985
- Sell JJ, Rael JR, Orrison WW. Rotational vertebrobasilar insufficiency as a component of thoracic outlet syndrome resulting in transient blindness. Case report. J Neurosurg 1994; 81: 617–9
- Saxton EH, Miller TQ, Collins JD. Migraine complicated by brachial plexopathy as displayed by MRI and MRA: aberrant subclavian artery and cervical ribs. J Natl Med Assoc. 1999 Jun; 91(6): 333–341.
- Selmonosky, C.A. Byrd, R. Blood, C. Blanc, J.S. Useful triad for diagnosing the cause of chest pain. South. Med. J. 1981, 74, 947-949.
- Selmonosky C.A, Silva R.P. The diagnosis of thoracic outlet syndrome. Myths and facts. Revista Chilena de Cirugia 2008, 60, 255-261.
- Selmonosky, C.A. Thoracic outlet syndrome. The missing link in the diagnosis of non-coronary chest pain. Italian Journal of Cardiology 2008, 9, 217S.
- Parham K. Benign Paroxysmal Positional Vertigo: An Integrated Perspective. Advances in Otolaryngology. Volume 2014 |Article ID 792635 | https://doi.org/10.1155/2014/792635
- Foster CA, Breeze RE. The Meniere attack: an ischemia/reperfusion disorder of inner ear sensory tissues. Med Hypotheses. 2013 Dec;81(6):1108-15. doi: 10.1016/j.mehy.2013.10.015. Epub 2013 Oct 22. PMID: 24199949.
- Dadsetan, M.R., Skerhut, H.E. Rotational vertebrobasilar insufficiency secondary to vertebral artery occlusion from fibrous band of the longus coli muscle. Neuroradiology 1990, 32, 514-515.
- Hardin CA, Poser CM. Rotational Obstruction of the Vertebral Artery Due to Redundancy and Extraluminal Cervical Fascial Bands. Annals of Surgery: July 1963 – Volume 158 – Issue 1 – ppg 133-137
- Alcocer F, David M, Goodman R, Jain SK, David S. A forgotten vascular disease with important clinical implications. Subclavian steal syndrome. Am J Case Rep. 2013;14:58-62. doi:10.12659/AJCR.883808
- Chahwala V, Tashiro J, Li X, Baqai A, Rey J, Robinson HR. Ann Vasc Surg. 2017 Feb;39:285.e5-285.e8. doi: 10.1016/j.avsg.2016.05.109. Epub 2016 Aug 13. Venous Thoracic Outlet Syndrome as a Cause of Intractable Migraines.
- Kim PW, Ledwitz-Rigby F. Variations in the anatomical structures surrounding the transverse process of the atlas (C1) in 15 cadavers. Experimental Biology 2014 Meeting Abstracts V28, issue S1. April 2014. (915.14).
- Park MS, Lee HY, Kang HM, Ryu EW, Lee SK, Yeo SG. Clinical manifestations of aural fullness. Yonsei Med J. 2012;53(5):985-991. doi:10.3349/ymj.2012.53.5.985
- Franz B, Anderson C. The Potential Role of Joint Injury and Eustachian Tube Dysfunction in the Genesis of Secondary Ménière’s Disease. International Tinnitus Journal, Vol. 13, No. 2, 132–137 (2007)
- Franz B, Collis-Brown G, Altidis P, et al. Cervical trauma and tinnitus. Int Tinnitus J 4:31–33, 1998.
- Raj PP. Stellate Ganglion Block. Raj’s Practical Management of Pain (Fourth Edition), 2007
Hi, I have suffered with various symptoms for nearly a year including constant dizziness/feeling as though everything is slightly moving, headaches and eye pain, anxiety, jaw pain and dislocating. I had an MRI with contrast at the beginning of the year which showed slight scoliolis in my neck and arteries being slightly pressed on. My gp has told me this would not be the cause of the constant dizziness I am getting but after reading your article I am not convinced. My posture is also very bad. Where should I start with correcting this? Should I see a chiropractor?
I recommend that you come by my clinic.
Hi, I have suffered with various symptoms for nearly a year including constant dizziness/feeling as though everything is slightly moving, headaches and eye pain, anxiety, jaw pain and dislocating. I had an MRI with contrast at the beginning of the year which showed slight scoliolis in my neck and arteries being slightly pressed on. My gp has told me this would not be the cause of the constant dizziness I am getting but after reading your article I am not convinced. My posture is also very bad. Where should I start with correcting this? Should I see a chiropractor?
Hi. I am not sure if you can help with my problem, but a lady put a link to your website on a vestibular migraine post on Facebook. I have had long standing dizziness, balance issues,fullness in my ears, pressure in my sinuses, and neck and shoulder pain for the last 4 to 5 years. I have went to so many doctors, specialists, physiotherapy, chiropractor, osteopathy, and nothing has helped. I am unable to work or do many things because of my condition. My doctor has said it’s possibly vesitbular migraines, as I suffer from migraines, but I am very unsure that this is the real problem . Is this something that you could help me figure out. Many thanks, I look forward to hearing from you
Hello, yes, I can help you with this. I suggest that you book a Skype consultation.
Hi. I am not sure if you can help with my problem, but a lady put a link to your website on a vestibular migraine post on Facebook. I have had long standing dizziness, balance issues,fullness in my ears, pressure in my sinuses, and neck and shoulder pain for the last 4 to 5 years. I have went to so many doctors, specialists, physiotherapy, chiropractor, osteopathy, and nothing has helped. I am unable to work or do many things because of my condition. My doctor has said it’s possibly vesitbular migraines, as I suffer from migraines, but I am very unsure that this is the real problem . Is this something that you could help me figure out. Many thanks, I look forward to hearing from you
Hello. i am from the united states and for the last year and 3 months i have had constant lightheadedness/dizziness. it is never vertigo but i just feel faint at all times. i used to workout in the gym and lift weights. On march 23rd 2019 i went tot the gym and lifted weights, i did bench press, pull ups, bicep curls and work my back out with some cables. ever since i have been stuck with this 24/7 constant dizziness. i have been to every doctor you can go to and they all say nothing is wrong. i have seen chiros who told me i have a “military neck” or “straight” neck. i saw a upper cervical chiropractor who made my symptoms worse. about a few weeks after that i started experiencing tinnitus that hasnt gone away either (its not super loud thank god) i have had cat scans done on my brain and i have no tumors. i even got a special ct scan to rule out semicircular canal dehiscence and they said that was normal…. but i have extreme thinning near my facial nerve but they dont think thats the problem. At this point i am being told that it is only caused by stress. i am 29 years old and had to stop working, skateboarding, hiking and pretty much anything that requires activity. my life is hell and i know you guys are in norway but i was wondering if you had any recommendations for me? my email is [email protected]
Book a skype consultation and send me your imaging
Hello,
I am a 38 year old guy from Canada and since the morning of July 3rd, 2020 I have had a sort of 24/7 oscillopsia twinned with dizziness where when I move my head in certain movements, objects don’t stay stable and blur, and brain fog, inability to think well. The weird thing is that the features of the oscillopsia have changed a bit in that time, sometimes better and worse. I also get a weird effect sometimes where when I move my head up and down, objects in my visual field seem to move slightly to the right as well as up and down. I thought I had BPPV at first, because I get little vertigo spells from certain heas movements, but I’ve done Epleys and it doesn’t seem conclusive.
In the week before this happened I started running for an hour at night for the first time in years. I was not sick with a virus or anything.
The morning it happened I woke up, felt fine and moved my head to the side and got a vertigo spin feeling. From there it progressed to nausea, photophobia, loud sound sensitivity, pressure in head, pain behind eyes, eyes catching up to head movement
foggy brain, like a flu, but only in the head. In the last month and a half, I started to get a ringing in my ears. Another weird symptom is that periodically my head, at rest, seems to want to fall laterally to the side, or sometime backwards, or sometimes torqued to the left. As if that is the center of gravity, not straight and on my shoulders.
I went to ER on 2nd day and they said likely labrynthitis or neuritis. But I had no virus. I had another similar episode mid Sept 2020, and that doesn’t fit with labrynthitis. It also doesn’t feel like its really improving. I still feel dizzy and brain foggy. I had VHITs done privately and it seems like it might be a central vs. proxysimal cause based on audiologists assessment as both semi circular canals were deficient in the same head movement, upwards. But not downwards.
I have been reading your articles, and I think I might have a hinge neck (I work at a standup desk on a computer) and also the TOS, because my scalene muscles are really tight and it feels super ‘nervey’ and then painful if I press into the triangle. My jaw muscle is also tight. It hurts to press into the joint. I think I might be a ‘clencher.’
At the base of my skull, maybe 1-2 vertebra down, it hurts to press on the both sides, more on my left.
I’m still waiting to see a neurologist and I’m starting to lose my mind thinking I’m going to be like this forever. My son is only 2.5 years and I can’t bear thought that I am going to be a dizzy, spaced out mess as a father for life..
I had a minor concussion when someone opened a door on the top of my head as I was looking down in Nov 2019. I was foggy for several days afterward.
I had a CT scan in emerg last week and they said it was ‘normal.’ Bloodwork, normal. Echocardiogram, normal. EKG, normal. MRI in march 2019 normal. I’m going to get another MRI soon.
Do you have any idea what this could be from? Next steps I should take?You obviously are very knowledgeable, and thoughtful. Any insights you could provide would be much appreciated.
Book a skype session and send me your head and neck MRIs. I’ll have a look at the head CT also.
If you have any angio-/venograms I’ll see those also.
Hi Kjetil,
I have just sent you a message on Facebook but I am delighted to find you here!
I have been suffering from tinnitus since June 8th sudden onset.
I had two incisors removed on May 29th which was under local anaesthetic and very traumatic due to abscess and difficult numbing of anaesthetic a lot of pulling and pain.
Subsequently my bite is more off and scheduled finally for denture plate and occluder and equillabration due to missing teeth with TMJ dentist. Naturally anxious as anything in mouth aggravates tinnitus eating chewing swallowing. Dentist is hoping it will ease mouth muscles?
Wound healed normal but I have not due to tinnitus. Only relief when standing.
History of whiplash many years ago and chronic scapula pain. Usually managed at home stretch excercises.
Received chiropractor assessment and discovered mechanical! Somatic sensory tinnitus evokes with movement eyes mouth tongue head . Tension felt on temples with touch and head/neck flexion.
Can it be coming from levator scapula or neck history of cervical changes MRI 2008
Up until February working full time since 1978, and had planned togobacktowork but developed covid 19 symptoms March 8th no test done as none available until much later eventually tested in august and it was negative. Hard to know as test done five months after symptoms .
Can you let me know the best treatment for somatic tinnitus?My posture has not been good since March 8 possible hyaloid muscles diagram 3 resembles my neck?
.,
Due
Hi, this is too much for a blog comment. Please book a skype session and send me your images
Hello I had braces when I was 15-17. But to me my jaw was never corrected. Lately, for about 3 weeks I’ve tried to fix my jaw by moving it to the position I thought it should be in. And November 13th I started to drive and I got very dizzy, like I just got off a roller coaster ride and ever since I have just been waking up with dizziness and when I move around it starts. Heart races, palms sweat, and very nauseous like I’m just getting off of a roller coaster. My ears ring a lot. If you can help me, I would be truly thankful
Book a session and provide me with at least a head MRI
Hello,
I have suffered from barotrauma. I believe my inner ear has been damaged. Would we be able to get in touch?
Stewart
This is outside of my expertise. See an ENT.
I just followed your video on opening the mouth properly and I felt lot of pressure in my ear and heard a clicking noise (which i never do) but only after following your instructions on the youtube video. I’m protruding lower jaw forward when opening my mouth. My question is, is it normal to feel pressure in the ear and discomfort in the jaw joint?