Groin and anterior femoral pain is relatively common, especially amongst women, and can sometimes be debilitating. These symptoms are often wrongfully diagnosed as generalized diagnoses such as pelvic girdle syndrome, or as fibromyalgia. It can also be misdiagnosed as meralgia paresthetica, femoral or saphenous neuralgias. This article will detail an unknown but common musculoskeletal pathology that I have called pectineo-femoral pinch syndrome (PFPS), which often causes these exact symptoms. To the best of my knowledge, this condition has not been mentioned in the literature until our study (Larsen & Chieng 2019) included it briefly as a subcomponent of lumbosacral plexus entrapment syndrome, in 2019.
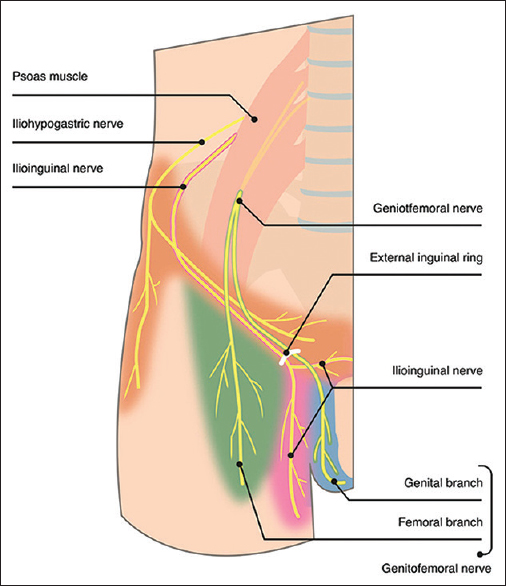
Pectineo-femoral pinch syndrome is a condition where the nerve bundle emerging from the femoral triangle (femoral, lateral femoral cutaneous, genitofemoral and ilioinguinal nerves), as well as the obturator nerves become positionally compressed by a combination of very tight upper adductor complexes (pectineus, add. brevis, add. longus), resulting in what often seems to be lumbar plexopathic pain due to its large potential area of affection, but is really caused by compression of the bundle of nerves in its periphery rather than at the site of the plexus. This holds especially true for patients where the symptoms are exclusively positional, ie., occurring during or after provocative hip flexion.
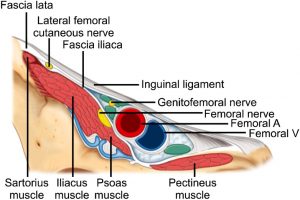
My first encounter with this problem was a patient with extreme femoral pain during squatting back in 2016. Most of the time, the symptoms occur after rather than during the provocative activity, making it much harder to detect its cause. In this case, however, it happened immediately during hip flexion. I treated her for lumbosacral plexus entrapment syndrome, which had helped her femoral pains that were induced by walking and running, but the squatting problem remained the same. After much back and forth and many trial and errors over the course of at least a year, I noticed how her squat-induced symptoms would ameliorate if we used a narrow stance, and conspicuously worsen with a wide stance. Similarly, she would also get worse with a deep- and better with a shallow squat. She would develop weakness in the quadriceps (L4 myotome) and adductor muscles (L3 myotome) after provocative activity. I had repeatedly been exploring the hip anatomy to try to figure out the cause of her symptoms, but as far as I could see, there was no obvious compressor of the femoral and related nerves emerging from the femoral triangle. When the patient noted improvement with a narrow stance, I figured it would have to be something with the adductors. A lot of back and forth resulted in a theory that the pectineus and upper adductor complex might lift and crush the femoral nerve and its companions into the inguinal ligament, only during hip flexion, and only in patients with very tight groins.
Because this is a positional compression of the nerves, it is not a mere irritation or myofascial entrapment neuropathy — It can exert a very strong compression on the nerve bundle, sometimes resulting in transient paresis of the quadriceps. I have seen grade 2 weakness in some of these patients, which is a weakness so strong that the patient cannot extend their knee against gravity (ie. cannot lift the weight of their own thigh), although this is less common. Both symptoms and weakness improve when the patient avoids excessive hip flexion. The definition of “excessive” varies from patient to patient, depending on the degree of groin tightness but also the degree of lumbosacral flexion. Lumbosacral flexion detauts the adductor complex during hip flexion.
The most common cause of the extreme groin tightness tends to be either hip impingement, hip osteoarthritis, or anxiety / PTSD / OCD. What all of these have in common is that the patient tends to clench their groins to stabilize either the hips or as a bracing maneuver to protect themselves. Sometimes this strategy is also seen in bedwetters or prolonged childhood bedwetters. It is also commonly seen in rape and sexual abuse victims.
Whether this problem also has the potential to compress the common femoral artery and vein is by me unknown, but plausible, and may be a cause of seemingly idiopathic thromboembolic development in these two vessels due to repeated mechanical insults, similar to that seen in costoclavicular syndrome (thoracic outlet syndrome) (Bushnell et al. 2009; Hussain et al. 2016).
Diagnosis
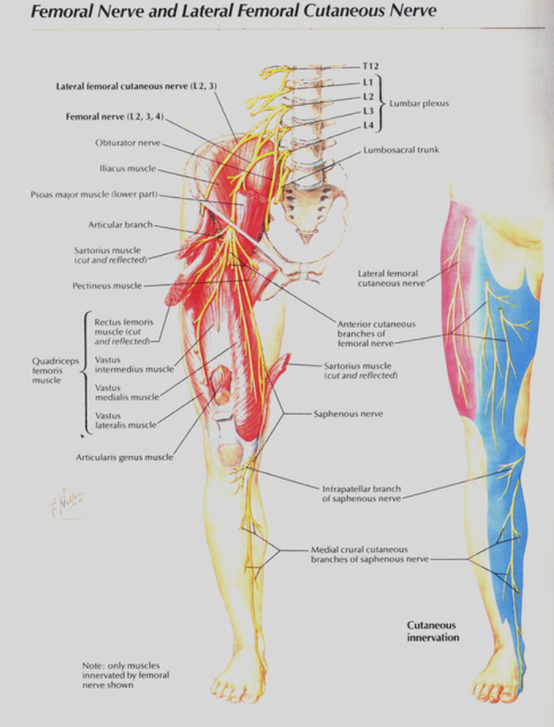
The typical patient with pectineo-femoral syndrome will complain of severe pain in their groin or thigh, often in the zone of innervation either of the lateral femoral cutaneous, femoral, saphenous, genitofemoral, or obturator nerves. In simple words, anterolateral, anterior, groin or anteromedial thigh and leg. Testicular or anterior labial pain may also sometimes occur. They will generally report that their symptoms are much worse when sitting, but not all of them are able to detect that the degree of hip flexion is the most crucial variable for pain generation and intensity. The patient may enter your office limping due to the sometimes severe neurogenic weakness that PFPS induces. Sometimes, the patient (athlete) will be asymptomatic with regards to pain, but note weakness or lack of progress in their training (leg-/quadriceps dominant exercises). They may also note severe muscle soreness up to a week after training in the adductors of quadriceps that is misperceived as DOMS. In reality, these are neuropathic symptoms that will improve with a decrease in hip flexion. These patients may also be screened for PFPS.
Place the patient on the table and perform a spine, neurological exam of both lower extremities as well as a hip impingement examination of both hips. Hip impingement is a common finding in this patient group, often with very stiff FABER and abduction tests (suggesting posterior and lateral femoroacetabular arthritic lesions). Anterior femoroacetabular impingement (AFAI) may also be present. Have the patient bend their spines forward and backward to ensure that spinal flexion and extension do not induce L3 or L4 radiculopathy, nor great spinal pains. Perform strength tests for the lower extremities (L1-2 hip flexion, L3 adduction, L4 quadriceps, L5 foot dorsiflexion, S1 toe flexion, S2 hamstrings) — We are predominantly looking for weakness in the L3 and L4 myotomes. Weakness in other myotomes suggests other causes than PFPS. Sometimes, the patient will only demonstrate weakness after provocation, and a lot of strength may be necessary to break the patient’s quadriceps strength even when it is compromised, as it is a very large muscle group. A lumbar MRI should be done, to exclude L3 or L4 root stenosis, usually at the L2-3 or L3-4 lateral recess sites. This would rarely only affect the patient when they sit, but should be done nonetheless. Technically, other causes of neuropathies could also be excluded (MS, B12 deficiency, etc), but if the patient’s symptoms are solely triggered positionally, this strongly suggests a musculoskeletal origin of their symptoms.
Next, after having excluded a spinal cause of their symptoms, the most important provocation test is the Larsen squat test. If the patient had normal, or just slightly decreased L3 or L4 strength levels prior to provocation, make note of this. Have the patient squat down while slightly arching their low backs, while leaning into a wall. They should just be sitting down in a full squat (“relaxed”), not constantly clenching (fatiguing) their quadriceps. Stay there for two minutes. After this, immediately place them on the table and retest the adductors (L3) and quadriceps (L4) muscles on both sides. A positive test will demonstrate weakness greater than what was previously noted without provocation. It is best for a strong individual to perform this test, especially if the patient is a man. Grade four weakness (mild to moderate neural compromise) can be almost impossible to detect in the quadriceps if the patient is strong. Grade three weakness (paresis) will be easy to detect as it suggests severe neural compromise. Grade two weakness would be evident if the patient is not even able to extend their knee against gravity. As already insinuated, the more sinister the patient’s affliction is, the easier it is to detect it with the provocation test.
After confirming the weakness with positional compression of the femoral and obturator nerves, place the patient in a chair and have them lean well backward. Wait five minutes and redo the L3 and L4 tests. Decent strength should now be demonstrated, unless they were limping into your office in the first place, in which it may take a few weeks for full recovery of neural strength. Normalization of strength is usually seen, in compliant patients, within 4 weeks.
Treatment
As should already be evident, the main treatment for pectineo-femoral pinch syndrome is to avoid excessive hip flexion. Generally, this will involve avoiding squatting and forward bending more than absolutely needed, and especially to avoid spending long durations in these positions. It will generally involve a sitting position that is leaning back to about 135 degrees. Rounding the back will help to detaut the groin, but will often result in low back pain. I, therefore, prefer to lean back (decrease degree of hip flexion) rather than rounding the back to stay more vertical.
Simultaneously, the patient may rehabilitate the underlying culprit of their problem. This will, initially, involve stretches for the upper groin muscles, or massage therapy. However, the massage therapist must pay special care not to massage and compress the femoral nerve in the femoral triangle. This can cause a dramatic worsening of symptoms. The stretches must not be done in 90 degrees of hip flexion, as this will worsen the compression. Approximately 135 degrees of hip flexion is suitable during the stretch, to target the upper adductor muscles. The knee should be bent during the stretching. Patients with underlying stress should become aware of their groin bracing habits and work on stopping this. Psychotherapy or anxiolytic drugs may be helpful in some circumstances. Patients with hip impingement may require a combination of cam or pincer surgeries or just conservative treatment (strengthening of the piriformis, gluteus medius, minimus and iliopsoas muscles). Patients with significant OA should undergo hip replacement, and strengthen the same muscles required in hip impingement cases.
It is possible to quickly recover from the symptoms associated with pectineo-femoral pinch syndrome. However, restoring normal hip flexion capacity without pinching the nerves is often a lengthy process, and patience will be required. With regards to pain, the prognosis is very good. Full range of motion, however, not always possible to reobtain. Improvements in hip flexion, however, is generally possible with a combination of the above-mentioned strategies.
Athletes with pectineo-femoral pinch syndrome should avoid full range-of-motion squats, and may benefit from rounding their backs slightly in the bottom (as long as it reverses on the way back up). A more narrow stance is favorable, presuming there is no significant anterior femoroacetabular impingement, in which we would have the dilemma between pest and cholera. Both of these corrections will generally enable greater squatting depth with less femoral nerve pinching.
- Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome. Part one: A common yet little-known cause of chronic pelvic and lower extremity pain. Anaesth pain & intensive care 2019;23(2):124-137.
- Bushnell BD, Anz AW, Dugger K, Sakryd GA, Noonan TJ. Effort thrombosis presenting as pulmonary embolism in a professional baseball pitcher. Sports Health. 2009;1(6):493-499. doi:10.1177/1941738109347980
- Hussain MA, Aljabri B, Al-Omran M. Vascular Thoracic Outlet Syndrome. Seminars in Thoracic and Cardiovascular Surgery Volume 28, Issue 1, Spring 2016, Pages 151-157
Hi Dr Kjetil,
I find that when I do the larsen squat to my patients they get super tired and they cannot avoid to clench constantly their quads. Do you have another option to diagnose this syndrome or another feedback I can say to them to avoid the constant clenching? I’m not sure if they are weaker because they are tired or because they present this syndrome. Thank you
hey Juan
You sure we’re talking about the same thing?
Sounds like they just need to squat with lower weights.
I mean, they present the symptoms (burning pain, weakness after sitting..) and when I put them into the squat to redo the mytome exam, it is very hard for them to mantain the larsen’s squat.
That’s not how it should be done. You’re doing it wrong. The myotome exam is done on the table.
Can this be a more low grade, chronic problem if the nerves have been irritated for a long time ? I fit the description ie anxious, clencher, fai, and have occasional sharp groin pain but more persistent burning tingling nerve pain in the areas mentioned but no weakness. Aggravated by sitting with excessive hip flexion.
Read my lumbar plexus entrapmnet syndrome article
Hi I stumbled across you in trying to google my symptoms of having anxiety with C1 and C2 damage I am currently working with a nucca practitioner from Kelowna British Columbia. Do you have anyone who does what you do in my town I found your article extremely fascinating and educational not sure where to go in collecting my spine
I often have this intense pain in my right leg from my hip to my knee.The pain is generally in middle thigh but the pain goes from my hip to my knee.It usually lasts for a week to ten days me in bed I can’t put pressure on my leg or walk on it the pain is so bad
I have spent hours and hours searching, and this is the first article that I have found describing to a T what I am experiencing. MRI, CT scans and EMG testing found nothing. Unfortunately I am a landscaper and cannot avoid deep hip flexion, may have to quit my job. Do you know of any doctors in the Seattle, Washington area who could help me with this? TIA for any help
Would like to be added to your distribution list
Hi. Apologies, there isn’t one. Consider following me on social media platofrms. There should be links available on the “about me” page I believe, or in the bottom of the page
Hi Kjetil.
You fixed my TOS 3 years ago. Well I guess I fixed it with posture change and trap training after our appointment. It was agonizing left shoulder/neck pain and numbness that could not be explained by MRI, XR, multiple MDs for years. For that I am grateful. Completely back to normal now.
Ironically I began having left hip pain over the last year. It started as dull left side lower back ache. Since then it has migrated to the left hip. I cannot sit for more than 30 minutes at a time. I will have pain for days afterwards. I have difficulty with flexi on/abduction. Interestingly I can run everyday, workout with weights daily no problem. So I knew it had to again be an elusive process. I read your lumbar plexus compression article but it didn’t fit all the boxes. However now I realize that I have PFPS as first described by you in this article.
My question is, why do you advocate stretching the pectineus when otherwise you are so against stretching a weak muscle? How is this different than the anterior scalene in TOS?
Thanks in advance.
If you read my 2019 paper on LPES you’ll see that I advocated strengthening of the pectineus. Unfortunately, if 90% of your protocol is right then a 10% error will still cause improvement. This was the problem here, it took a long time until I realized how wrong I was; the pectineus tends to tense up due to clenching in hip instability and anxiety patients. The treatment, therefore, is to stretch or massage the pectineus and strengthen the hips / stop clenching.
This is the first article I have read that describes in part my symptoms. R groin surgery..no pain..fine til I stepped in a very small indented hole. Pain diagnosed as acute spasm psoas. Treated and I do regular exercise..but pain anteriormedial thigh and I can not squat.
So..I read with interest..if I do narrow squat..no pain. If I hyperextend ( avoid the slight bend at lumbasacral I can weightbear without pain..how do I long term rehabilitate …It improves with rest, but the moment I get up…have you observed any psoas involvement with this syndrome?
Read my LPES article
Hi Mr. Larsen,
Thank you for presenting such a thorough and detailed explanation of PFPS. I am wondering if a long term symptom of PFPS would be swollen inguinal lymph notes due to the compression and lack of circulation in this region?
Thank you for your consideration.
Lymph, doubtful
Oh yea, have you heard of testicular pain symptoms with this condition mistakenly being attributed to chronic epididymitis?
I had a right distal femur prosthesis due to bone cancer, originally 25 years ago. Now on my third one (due to previous fractures), and this time pain is horrendous. 16 months on from revision, I am reliant on two crutches unable to weight bare due to excruciating pain. Severe pain in my groin area, definitely worse when bending or leaning forward and a feeling of something pinching or catching. Pain so intense muscles spasm in my leg and I have to take morphine. Leg is so weak I have to physically lift it as seem to have no strength in it, but when knee is bent, not extended, I can lift and raise it. However, I can have brief periods where this is not the case, and sometimes I can go from being crippled one minute, to good for an hour and back to crippled. I am acutely aware that bending, squatting and sitting down, brings the pain on. Numerous X-rays, MRIs and CTs show nothing of significance. From an orthopaedic point of view, all looks good, but I am in severe pain in the hip and groin area and don’t know what to do. I am a normally healthy active female, who for the past 12 months has completely been unable to function and from reading your article I am positive this is what I am suffering from. I do know I tense my leg in an effort to stabilise the hip area and to avoid the pain, but am unable to prevent myself from doing this as I am waiting for the pain. I am in UK but wonder if you could give me any advice or guidance as to how I can overcome this as I am in a desperate situation. I have a great consultant but his expertise is oncology arthroplasty, and he has done his job in rebuilding the leg, but is unable to tell me why I am suffering so badly.
Hello,
Is there a link for a peer reviewed version of this article? Thank you for helping us injured people out!
I mention it in the LPES paper I wrote in 2019