
Many patients suffer from chronic spine or radicular pain (radiative pain into their limbs), and undergo magnetic resonance imaging (MRI) with an aim to detect the cause of their symptoms. There are many things that can go wrong in this process, resulting in improper treatment and patient guidance. This article will address common mistakes as well as appropriate approaches in spine imaging interpretation, clinical workups, and treatment.
Clinical signs of spinogenic pain
Spinogenic pain, meaning pain that originates from spinal pathology, is common. Up to 45% of adults suffer from low back pain each year, with its peak in age groups 35 to 55 (WHO). With regards to the neck, up to 20% of adults suffer from neck pain (Genebra et al. 2017). While an integrated approach and explanation of spine diagnosis are outside the scope of this article, I will explain the basic mechanisms, diagnostic workups and treatment strategies for this patient group.
Degenerative spinal pathology tends to manifest as either segmental back low back or neck pain, with or without radiculopathy (radiative “nerve” pain). In the acute phase of a disc herniation, severe spinal pain which spreads into most of the lower back or neck, along with strong radicular pain in the entire limb or even both limbs will often occur. In cases of chronic radiculopathy or bone disease (usually Modic changes), the pain is generally focal at the affected spinal level, and the degree of radiculopathy may not affect the entire limb, but be more diffuse. It will also often come and go, and especially vary in intensity.
Approach for spinogenic neck and upper limb pain
Patients with non-acute spinogenic neck pain and brachialgia or periscapular pain are often misdiagnosed. Their brachialgias may be misdiagnosed as biceps or triceps tendinitis by a clinician poorly trained in neurological examinations. Periscapular pain may be misdiagnosed as thoracic facet joint subluxations or similar, usually by a therapist practicing manipulation therapy. Pain between the shoulder blades are usually induced by C5 or C6 root compressive disorders. Brachialgias can be C5 to T1, technically, although C8 and T1 are uncommon in spinopathy. C4, C5 and C6 root compression are the most common findings, but C7 is not rare either.
It is important to understand that spinal positioning and loading are the most important variables in the aggravation of spinogenic pains. If a patient says that every time they look to the right, it radiates into their right arm, shoulder blade or shoulder, this should warrant a spine workup by the clinician. First, a Spurling’s test should be done. A Spurling’s test is a compressive test for foraminal compression. The patient will lean their head all the way back, and the clinician will apply axial compression (push down on the head). If the test is negative, it can be done with rotation to the left and right. Ipsilateral rotation and extension will worsen the foraminal stenosis on the side that is rotated towards. You may have to hold the test for up to a minute in some patients, but be careful not to apply excessive pressure. Either immediately or within some time, frank pain, murmur or paresthesia should appear in the trapezius, shoulder, shoulder blade, arm or fingers. You can try to detect a dermatome pattern, although it is sometimes deceiving. Thumb pain often suggests C6 root stenosis, while 2nd and 3rd digits suggest 7th cervical nerve stenosis. Pinky are either C8 or T1 roots, but this is rare in spinogenicity. Shoulder pain is often C5. And, as I said, pain between the shoulder blades tend to suggest C5 or C6 root stenosis. Just be sure to understand that the symptoms elicited from the test does not usually follow the typical dermatomal pattern, and is often not elicited immediate during the test. There will, in almost all circumstances, also be elicited frank neck pain during the test, and you will feel patient reluctance when pulling them into the position. Beware that some patients, usually chronic sufferers, may have normal Spurling’s tests and virtually normal strength exams despite aggressive MRI findings. Reproduction of symptoms with valsalva maneuver or coughing is also a relatively specific indication of herniation with root compression.

It is possible to apply traction tests for the musculocutaneous, median and radial nerves during the Spurling’s test, similar to a modified Lasegue’s test for the low back, for increased sensitivity and specificity. The ulnar traction test can also be done, but as I have said [repeatedly], it’s not commonly affected in spinopathy. After this test, a myotome workup should be done. Apply solid pressure when performing these tests; do not treat your spine patients like stroke patients. This is a common mistake done by many neurologists. Look for asymmetries. They can be subtle, even in significant root stenosis, when chronic rather than acute. Paresis is rare in chronic radiculopathy. For the C4 myotome (C3-4), have the patient perform a shrug (scapular elevation). This test is usually negative unless there is very aggressive stenosis. Moreover, not all patients’ main myotome for the spinal accessory nerve is the C4 level. For the C5 root (C4-5 level), resist shoulder abduction at 45 degrees. C5-6 median nerve, have the patient pull their index finger and thumb together and try pulling them apart. C5-6 musculocutaneous nerve, resist elbow flexion (biceps) at 90 degrees). C6 radial nerve, wrist extension, C6-7 combined median and ulnar nerves, wrist flexion (keep finger extended and resist at the palm). C7 radial nerve, elbow extension (triceps) at 90 degrees. C8 ulnar nerve (C7T1), have the patient pull their pinky and thumb together and try ripping them apart (use less force here). T1 root (T1-2 level), finger abduction. Don’t use a lot of force. Examine both sides.
If a Lhermitte’s sign is elicited (lightning down the whole spine) during the Spurling’s maneuver, this warrants a rapid MRI as it may suggest central stenosis. Radiating pain into the legs does as well. Paresis (severe weakness) discovered during the clinical workup also warrants a rapid MRI.
Let us say that our patient has right-sided brachialgia and pain in the shoulder blades when reading books and using his cell phone. It is a nagging 5 out of 10 NRS on the scale. Coughing (valsalva) reproduces the pain. You perform the Spurling’s test and feel patient reluctance and stiffness when performing it. Within 30 seconds some radiation is elicited into the right thumb and his shoulder blade. You perform the musculocutaneous, median and radial nerve traction tests while having him in the Spurling’s position (obviously you will not be applying head pressure at the same time), and they are positive. You lie him down on the bench and examine the good arm (left) first. All myotomes are normal, except mild weakness of the pinky (this is common in asymptomatic patients). You examine the right side, and find normal shrugging and shoulder abduction power (C3-4 and C4-5 levels), but find weakness in the grip strength (C5-6 median) and wrist extension (C6 radial). Wrist flexion (C6-7), triceps (C7) are strong. C8 and T1 myotome also mildly weak. This clinical workup strongly, very strongly suggests right-sided C5-6 foraminal stenosis either due to a herniation or osteophytes. You can also be at a lookout for mild C8 or T1 stenosis, but this is more likely to be caused by a mild costocalvicular syndrome without clinical significance, presuming the patient has no actual ulnar nerve symptoms.
If Spurling’s is normal and MRI is normal, consider a workup for thoracic outlet syndrome, which is an extremely common and misunderstood disorder with, perhaps, as high prevalence as spinogenicity itself. Most patients with TOS experience worsening of symptoms when carrying objects or working overhead, and have positive Eden’s, Morley’s and Roos’ tests. See my TOS article for more information. These patients are often misdiagnosed with fibromyalgia. 5th finger weakness is extremely common in TOS, as the C8 and T1 nerves lie very susceptible for compression in the costoclavicular interval (Selmonosky 2008). The Selmonosky triad for TOS include a positive Morley’s test, weakness of the 5th finger, and a positive “white hand sign” (carcass-like palm paleness when elevating the arms, within 1 minute) (Selmonosky 2008).
Cervical lateral recess stenosis
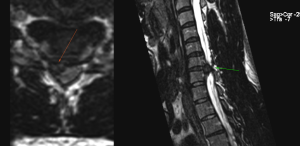
One devious cervical herniation variant to be aware of, is lateral recess herniations. This herniation will lie in the canal rather than the foramina and compress the emerging root fascicles directly adjacent to the medulla. In this case, the spurling’s test will be absolutely negative even in the presence of surgical grade herniations, as it does not compress the medulla, nor does it worsen foraminal stenosis with extension and rotation. The patient below had aggressive radicular pains and paresis of the triceps (C7). The Spurling’s test and neck maneuvers did absolutely nothing to affect his symptoms. MRI showed a huge C6-7 lesion compressing the exiting C7 root in its lateral recess. He was operated on with C6-7 ACDF and recovered completely.
Approach for spinogenic low back and lower limb pain
Patients with low back pain and radiculopathy usually see worsening with spinal flexion and extension. In an acute disc herniation, severe low back pain with obvious radiculopathy may enable easy rendering of the diagnosis. In chronic cases, however, the cause of the patient’s pains may not be as conspicuous. Ask about triggers. Does it hurt to put on your shoes? Is the back stiff in the morning and gets better with movement? Does it elicit pain or radiculopathy when you bend back (extend) your back? Did these symptoms onset with a “bang” related to a heavy lift or bending down? These are all common complaints that should increase suspicion for spinogenic low back pain.
There are three main problems that affect spinogenic low back sufferers:
- Lateral recess stenosis (also known as paramedian)
- Foraminal stenosis
- Vertebral inflammation (Modic changes)
- (Rarely(!), we may also see an extraforaminal herniation with actual root compression)

The lateral recess is the lateral compartment within the spinal canal where the root descends before exiting (a level below). The foraminae are the actual root outlets. Disc herniations generally cause lateral recess stenosis, whereas arthritis causes foraminal stenosis. Herniations tend to worsen with flexion (ie. radicular pains worsen with flexion), whereas foraminal stenosis worsens with extension. Moreover, foraminal stenosis is wildly (wildly!) underreported in radiology reports and is often also missed by surgeons. The reason for this is that it is underwhelmingly demonstrated in the axial planes on MRI, which we will discuss later.
Let us say that a patient suffers from very local spine pain and sporadic pain down the outside of his right leg (this is the L5 dermatome). Stand him up and have him slouch forward in “horrible” lumbar flexion. Does it worsen the back pain? Does it induce/reproduce the right-sided thigh symptoms? If so, this may suggest either modic changes, or lateral recess stenosis due to disc herniation. Now, perform lumbosacral extension, Have him pull his pelvis “back and up”, while leaning back with the torso. He may not tuck the pelvis under. Stay there. Does it induce spinal pain? Does it induce [often diffuse] pain in the butt, front of the thigh, or outside of the thigh? If so, this may suggest foraminal stenosis due to arthritis.
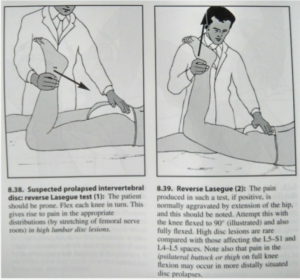
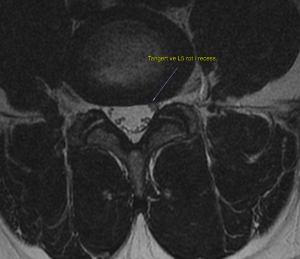
In continuation, move on to perform nerve stretch tests; Lasegue’s tests. These tests are different depending on where the root stenosis is (!). There is one test for the L5 and S1 roots (sciatic nerve) and one for the L4 root (femoral nerve – Reverse Lasegue’s test). You can also do a variant for the L3 root (obturator nerve), but this is a less common finding in radiculopathy. However, the test also varies depending on whether the compression is in the lateral recess, or in the root outlet. The Lasegue’s tests are basically stretch tests for the nerves, and to be positive, it needs to be done in a provocative position. Most clinicians do not know this. For lateral recess stenosis, the test should be done during spinal flexion. For foraminal stenosis, it should be done during extension (this is where most clinicians go wrong).
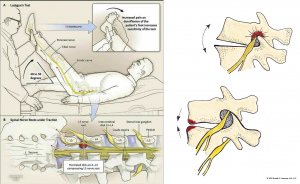
- For L3 radiculopathy, have the patient on the table and passively pull the leg into abduction. Pain in the deep groin is a positive test. This test should be done in flexion if there is L2-3 lateral recess stenosis (L3 descending – rare) and in spinal extension if there is L3-4 (L3 exiting) foraminal stenosis due to arthritis. Ie., just have the patient arch their low back and redo the test.
- For L4 radiculopathy, in the L3-4 lateral recess (L4 descending – not common but not rare), perform the reverse lasegue’s test when standing. Ie., stand, tuck the pelvis, and passively bend their knee and pull the femur into extension. For L4 stenosis in the exiting L4-5 foramina (common), have the patient prone on the bench, back arched, bend their knee and pull the femur back.
- For L5 radiculopathy in the L4-5 lateral recess (L5 descending root – common ), perform the standard Lasegue’s test with a tucked pelvis. For L5S1 foraminal stenosis (L5 exiting root – common), perform a standard Lasegue’s test with the low back arched. If it’s negative, the back may not be sufficiently arched. But sometimes it is negative despite clinical symptoms and compatible MRI. Mysteries of the universe. This regards all of these tests, of course.
- The S1 root does not have an intervertebral foramen, and can thus only become compressed in the lateral recess (L5S1 level – common) (or higher up due to central stenosis – not rare, not common). A supine standard Lasegue’s test will work fine, with a flexed spine.
The next thing that should be done, is a myotome examination. This is a little tricky in the legs and is often misinterpreted. Also, because the legs are strong, the clinician may simply not be strong enough to identify weakness in the quadriceps or patient’s dorsiflexor. Functional tests may be viable for clinicians with poor upper body strength. For example, detecting quadriceps strength deficits can require extreme loads depending on the patient’s body type and strength level. Most patients will present with relative weakness and not absolute weakness, where the latter, clearly, is much easier to detect than relative weakness. The L3 root innervates the adductors. The L4 root innervates the quadriceps. The L5 root innervates the foot dorsiflexors (tibialis anterior, peroneal group), and the L5S1 roots innervate the foot evertors (peroneals). The S1 root innervates the calf and the toe flexors. It is very important to understand that foraminal stenosis will be completely OCCULT in the examination if the patient is not placed in extension, even in severe incidences. It is preferable to have an MRI at hand before performing the exam, or else it will take too long and include a lot of double checking. For example, if you know that the MRI shows L5 lateral recess stenosis and L5 foraminal stenosis, then you know that the L5 and S1 roots are affected. Perform the L5 tests for traction and strength in both flexion and extension. Simple, right? Ok, it is a little complicated, but once you’ve done this a few times, it becomes a logical algorithm.
Always do both a manual exam and a functional exam for the legs. Even strong clinicians can miss weakness in the quadriceps, for example. I will have the patient supine and I’ll lower the bench to a height where I have the advantage. Resist hip adduction at 20-30 degrees of abduction (L3). For the quadriceps (L4), bend the knee and hip to 90 degrees. I will place my left hand in the posterior crease of the knee, and my right hand at the lower shin and attempt to break them down (I weigh 110 kg / 240 lbs). It is very difficult to break the patient’s strength at this position. For the L5, have them dorsiflex, and try to pull them down. Use both hands if you are not strong. For the S1, grip the patient’s toes (2-5th, not the hallux) and have them flex their toes hard. Try to rip them open. You will have to modify the tests (spine flexion or extension) based on clinical suspicion and MRI appearance. If there is weakness also in the S2 (hamstrings), this could suggest piriformis syndrome or central stenosis. The latter, especially, if there is concomitant sphincter dysfunction (S2-4). S2 weakness is not seen in spinogenicity except for incidences of central stenosis (this is because it does not transmit in the lateral recesses nor intervertebral foraminae).
For most clinicians, functional myotome tests for the lower limbs may be more applicable. For adduction, you have a good manual lever if you grab the lower shin, so this is not necessary to modify. However, the L4-S1 myotomes, modified tests are helpful. The squat is bipedal and thus easy to cheat by moving more weight over to one side. It is therefore preferable to one a one-legged squat. Have the patient hold on to something to maintain balance. Squat down (no need to go deep) and evaluate side to side difference and compare it to the MRI. For the L5, this is generally not so hard to detect manually, but you can also have the patient heel-walk. A common cheat is to make the steps more narrow due to weakness; have them make broader steps. For the S1, manual pulling on the toes has a decent sensitivity. However, walking on the toes is more specific for severe S1 stenosis. If the patient can walk on the toes, have them do unilateral calf-raises and evaluate strength side to side. Also here, don’t let the patient cheat by making their steps too narrow.
As with the upper extremities, always consider entrapment neuropathy as a potential cause if there is a truly normal MRI and no spinogenic triggers. See my article on lumbosacral plexus entrapment syndrome.
Scenario 1
A 35 year-old patient submits to your care with low back pain and radiculopathy down the backside of both legs. It came suddenly during deadlifting. You ask if it hurts to bend forward and he says that he can barely move and struggles to put his clothes on. You stand him up and have him bend forward; it causes tremendous low back pain and lightning is passed down both S1 dermatomes. You ask if he has any problems either emptying his bladder or peeing himself, but he says no. The Lasegue’s test is positive bilaterally, and there is weakness of the toe flexors bilaterally. He is able to walk on his toes, but with considerable effort. These findings are all in complete harmony with an L5S1 broad-based disc herniation, compressing both descending S1 roots in their lateral recesses. Physical therapy focusing on proper spine posture, bending technique (hip hinging) and decreasing stress and abdominal tension tend to be the best options for conservative management. If refractory, microdiscectomy can be pursued, and will have good results.
Scenario 2
A 55 year-old patient has been suffering from low back pain and right buttock pain for years. He has had several MRIs, but they were reported as normal but with age related findings without root compression. You ask him about triggers, and he says that he can sit and work in his office, but struggles to walk for longer periods, and also wakes up with pain during the night, especially when he’s on his back or stomach. “I’ve been told that I need to learn to live with it”, he says. You stand him up and have him flex and extend the spine. Flexion is ok except for mild stiffness, but extension hurts. You tell him to really push into extension and lift his butt up while he’s doing it. Gradually, right-sided buttock pain is induced, and it also radiates slightly down the lateral side of the calf. He says that the calf tends to start aching after walking for 45 minutes or so. You put him on the table and perform a Lasegue’s test with flexion and extension. It seems to be moderately positive only in the extended position. You test the right dorsiflexor but it is normal. Toe flexors are also normal. You stand him up and have him hyperextend his low back for 1-2 minutes, and rapidly retest the right L5 dorsiflexor. It is now weak. You review the MRI in the sagittal plane (Sagittal T2w images) and realize that there is considerable arthritic stenosis bilaterally, more pronounced on the right side, that has not been reported. This problem cannot be treated conservatively; no amount of physical therapy can remove the osteophytes from the foraminae. Endoscopic foraminotomy or lateral arcotomy are the best treatment options for this problem.
Scenario 3
A 45 year-old patient visits your office with severe, longstanding low back pain that is almost solely flexion-induced. He suffers when working and when sitting, but feels a little better when walking and exercising, especially when he tries to “stay upright” in his posture. He says that he had numerous episodes of acute lumbago with radiation when he was younger, with onset in his early twenties, but hasn’t had radiative pain in a long time. “But the low back pain killing me”, he says. You have him bend forward, and it is painful. Extension is not very painful. Lasegue’s and myotomal exams are all normal. You review the MRI and see disc obliteration at the L4-5 level with considerable Modic changes of T2 and STIR hyperintensity (suggesting active bone inflammation — Modic changes). His bloodwork (ESR, CRP) is normal and he does not have fever or subfebrile clinical indications when his back hurts (this could suggest infected Modic, which happens once in a while). Installing a disc prosthesis is the best option in cases like this one.
Case 4 – real case
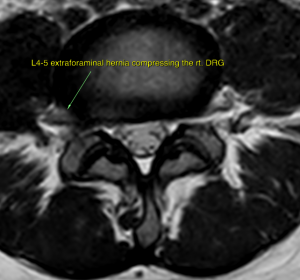
A 39 year-old woman consulted with me for acute low back pain and anterior thigh pain after undergoing lumbar spinal manipulation therapy. Although I am not a huge fan of these procedures, they are generally safe in the lumbar spine. I reviewed her MRI and did not identify any serious pathology. There was mild foraminal stenosis, but she had no issues arching her back. She felt no weakness in the leg. After some looking, I identified a right-directed lateral bulge at the L4-5 level that was compressing the L4 dorsal root ganglion (DRG). Such a hernia would bulge further if bending forward to the left, so I had her do that. Sure enough, it reproduced her symptoms along the L4 dermatome. The Lasegue’s test for disc-induced L4 radiculopathy is a little tricky, because the patient must be standing and tucking their pelvis while you perform the reverse Lasegue’s test. The test was positive, however, and only on the right side. This is a case of a symptomatic extraforaminal disc herniation. It is a rare finding, at least rarely symptomatic, in my experience.
Spine imaging and pitfalls
When should the patient obtain an MRI? In my opinion, either if there is weakness and compatible clinical examination suggesting spinogenicity, or if the pain has been ongoing for more than six months (no weakness). There is a lot of confusion and frank nonsense out there that MRI is not helpful in rendering diagnoses nor predicting clinical outcomes, but this is far from the truth. The reality is that most if not all of the clinicians making these absurd claims, do not understand the pathomechanisms of spine pain, nor know how to properly interpret MRIs and perform clinical correlation.
In reality, MRI is invaluable in determining the interventive strategy for spine pain, but it needs to be done, and read, properly. It is also helpful in excluding the spine as a probable cause of pain generation. Let us discuss some principles and common pitfalls.
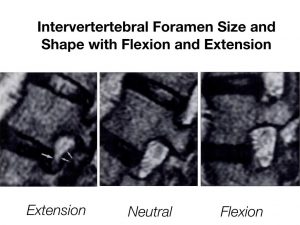
This is not to be viewed as a complete tutorial on spine imaging, obviously. However: For the spine, this is generally going to be the axial and sagittal planes, so that we see an axial cross section and sections from the side. This enables views of the roots and foraminae in both “short and long axis views”. Lateral recess stenosis and central canal stenosis is best appreciated in the axial planes. In the cervical spine, the axial slices are decent also in determining degree of foraminal stenosis, except when the resolution is poor or slices thickness is too wide. The cervical foraminae are angled at 45 degrees, and are therefore almost impossible to evaluate in plain sagittal sequenes. Therefore, in the cervical spine, we should always include sagittal-oblique images at a 45 degree angle. In the thoracic and lumbar spine, axial MRI is helpful in recess and central stenosis, but almost useless in determining foraminal stenosis (!). Many are not aware of this, and therefore end up underestimating the degree of foraminal stenosis. Thoracic and lumbar spine foraminal stenosis is best evaluated in the sagittal plane. The third point is that the degree of foraminal stenosis depends on degree of spinal extension, as extension further narrows the foraminae whereas flexion widens them. Therefore, clinical correlation is absolutely necessary when determining actual degree of stenosis and whether or not it is symptomatic.
NB: This part of the article is truly not intended to guilt or ridicule anyone, but because the quality of spine reporting is so extremely variable, it needs to be called out, and patients need to be able to educate themselves.
Cervical spine:
Good cervical MRI sequences include T2-weighted images (fluid bright), T1-weighted images (fluid dark), and STIR (highly fluid sensitive sequences) in the sagittal plane. In the axial plane, T2 and GRE sequences are often used, preferably with a 2-ish millimeter slice thickness. Sagittal-oblique sequences at 45 degrees and 1,5-2mm slice thickness should be used. The axial sequences should be angled in line with the discs. Once the axial box is off-axis, the determination of foraminal stenosis becomes less reliable. The most common pitfalls in cervical spine imaging for degenerative pathology are:
- Believing that foraminae may be roughly evaluated in plain sagittal images. Some doctors, when short on time, may only skim through the sagittal sequences and not review the axials. This often leads to severe misreporting. The reality is that the central canal may appear impeccable even in the presence of severe foraminal stenosis, in neutrally sagittal sequences.
A woman had gradual onset of what eventually evolved into severe neck pain with radiculopathy and periscapular pains. Her Spurling’s test was positive. She had an MRI two years prior which was negative but with “normal age-related degenerative changes”. She had asked her GP for a new MRI, but was denied one because her prior was normal. I asked for a new MRI, including sagittal-oblique images. Sure enough, the central canal looked impeccable, and there was no pathology seen in the sagittal plane. However, three levels of severe root stenosis due to disc-osteophyte complexes were easily seen in both the axial and sagittal oblique images. It is clear that these sequences had not been evaluated at all by the first interpreter, two years prior. This is a surgical; chanceless to treat with physical therapy. The patient had spent 10s of thousands of dollars on PT without improvement.
- Using wide slice thickness without sagittal-oblique correlation. In some patients, one part of the foramina can be open while another part (either its upper or lower parts) completely obstructed due to disc/osteophyte lesions. This is very hard to evaluate in plain axial imaging, especially without fine slices (1,5-2mm)
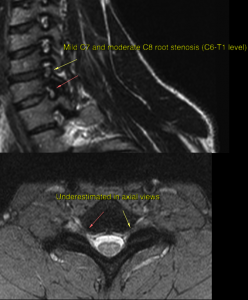
A 28 year-old male patient suffered from chronic neck pain with mild radiculopathy in the C8 dermatome (ulnar nerve) after an injury that occurred during a headstand exercise. He had an MRI, which was reported as normal, and underwent numerous sessions of physical therapy without improvement. As I have said, ulnar neuralgia is very uncommon in spinogenic pain. I reviewed his axial scans, and they appeared normal (there were foraminal openings wider in the given segment than what is seen below). Thankfully, there were sagittal-oblique sequences included. Here we could easily identify the problem; Arthritis moderately/severely filling the C7T1 (C8 root) and mildly filling the above C6-7 (C7 root) outlets. Note the very narrow foraminae in all levels above; this is congenital foraminal stenosis. This cannot be treated conservatively, so I referred him for foraminotomy. Needing surgery due to arthritis is certainly not common for an otherwise healthy 28-year-old, but with poor neck posture and concurrent congenital spinal and foraminal stenosis, this can happen. In this case, I do not think the interpreting physician had reviewed the sagittal-oblique images at all.
- A vital part of stenosis-grading is the clinical correlation. If the doctor interpreting the images does not have a lot of experience performing spinal and neurological examinations, it can be hard to reliably and correctly grade sites of stenosis. This can confuse the patient’s GP, who does not know how to read images and has to trust the reported findings. In cases like these, it is better to seek a second-opinion from a spine surgeon rather than just ordering a new MRI.
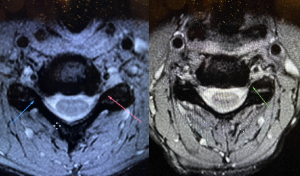
I sent a set of images out for second-opinion due to significant lymph swelling, which is outside of my expertise. I received a decent report with regards to the lymphatic problem, but additional notes of “mild foraminal stenosis”. I sent an email saying that I was happy with the report, other than the misgrading of the stenosis, and respectfully requested either removal of the grading (ie. just stating “stenosis), or appropriate grading. I also explained the clinical data, suggesting aggressive stenosis, especially of the right C6 root (left image). The company refused repeatedly. I ended up firing them, as the arrogance and unwillingness to cooperate was overwhelming.
- Not distinguishing between discogenic and arthritogenic stenosis. Disc lesions can heal, whereas osteophytes do not. Symptomatic foraminal stenosis due to osteophytic (arthritic) lesions can not be treated with physical therapy. It can be hard to distinguish between osteophytic and discogenic stenosis in the axial plane. A T2-weighted sagittal (for lumbar or thoracic) or sagittal-oblique sequence will enable you to differentiate between bony and disc tissues that are encroaching the foramina. This is very important for determining prognosis.
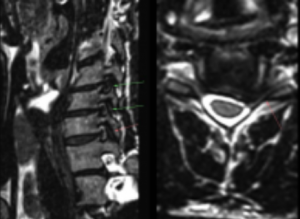
The images below beautifully demonstrate this problem. In the right image, there seems to be a large disc herniation filling up both foraminae, more pronounced on the left side. Correlation with sagittal-oblique sequences (left image) shows large disc-osteophyte beaks that can impossibly be treated conservatively. Multilevel spine surgery is warranted. For GPs and physical therapists, it is important to call the radiologist to ask whether or not the stenosis is discogenic or osteophytic, as this is rarely mentioned clearly in reports.
- The misconception that mild spinal cord compression is harmless.
A 50 year-old woman develops urinary incontinence and spastic paraparesis. MRI reveals mild cord compression that has caused signal changes in the spinal cord; myelopathy. It is rare for such light compression to cause myelopathy, but it can happen. And because it often does not reverse after surgery, lifelong debilitation may occur. Therefore, in circumstances of mild medullary compression, proactive treatment is superior to waiting for clinical deterioration; it should be revered. Do not attempt to treat spinal stenosis with physical therapy. On the contrary, very compression of the nerve roots must be present to cause irreversible paresis (permanent root damage). The spinal cord is much more sensitive to compression than the roots. Also, note that the herniation, in this case, is small. The compressive myelopathy would never have occurred with such a small herniation unless there was pre-existing congenital canal narrowing.
Lumbar spine
Lateral recess stenosis is easy to detect in the lumbar spine and is usually not missed. Sometimes, in cases where there is congenital stenosis (congenital narrowing of the spinal canal due to pedicular hypoplasia), even marginal amounts of bulging disc tissue or arthritis can result in lateral recess or foraminal stenosis. In my opinion and experience, the most commonly missed lumbar pathology is foraminal stenosis, without any doubt.
T2-weighted images are generally the ones most applicable when looking for root stenosis, both with regards to canal, lateral recess, and foraminae. A STIR sequence is helpful in grading the extent of vertebral inflammation (Modic changes). The sagittal T1w images are usually more sensitive in determining actual disc height reduction than the T2w images.
As I said, foraminal stenosis is frequently missed both by radiologists as well as surgeons, because of the misconception that axial sequences reliably demonstrate foraminal capacity. It is not without reason that Ross & Moore’s bible on spine imaging (great book, highly recommended) exclusively demonstrates foraminal stenosis in the sagittal plane, not in the axial plane. Unfortunately, the axial sequences grossly overestimate the foraminal size, whereas the sagittal plane is much more reliable in determining the degree of stenosis. Detecting arthritogenic foraminal stenosis is important because it cannot be treated conservatively.

Below is the case of a navy seal with severe back and right lower limb pain after a fall. The pain was so strong, he said, and this was a tough guy, that it crippled him, and he laid on the floor trembling in pain. He could not walk for more than 100 meters (ish yards) without devastating symptoms. He could, however, sit and work at a desk for 8 hours without a problem. Lumbar MRI was reported as normal. I had him perform flexion, and it was no problem. Extension, no problem. Lasegue’s test negative but Reverse Lasegue’s was borderline. Normal quadriceps (L4) strength bilaterally. I reviewed the MRI one more time and realized that there was a 9,5mm anterolisthesis that was affecting the foramina but was invisible in the central canal. The right L4 root was crushed in its foramen. I had him stand up again and hold the extended position for 5 minutes. The first two minutes, nothing happened. After 3 minutes he was shaking in pain, however, and I quickly retested his right L4 myotome, which was now paretic (nearly paralyzed). He was limping for the next 15 minutes, before the pain reduced (in spinal flexion). I recommended foraminotomy, but we might need to do both foraminotomy and fusion in this case.
Thoracic spine
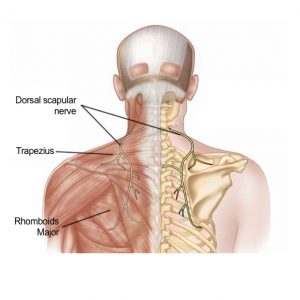
Imaging of spinal degenerative pathology in the thoracic spine is basically a combination of the cervical and lumbar spinal segments. Review the foramina as you would in the lumbar spine, and the central canal as you would in the cervical spine. Aggressive degenerative pathology in the thoracic spine is rare. In most incidences, I see patients acquiring a thoracic MRI because they have upper back / periscapular pain. In reality, this is usually coming from the neck through the dorsal scapular nerve, either due to C4-5 or C5-6 root stenosis, or due to thoracic outlet syndrome.
Post-surgical imaging
There is a lot of internal politics in medicine. And again, I am not writing this to bash anyone. However: Many radiologists are shy of conflict and thus reluctant to describe poorly liberated foraminae after surgical intervention to avoid getting angry calls from spine surgeons. Below we see a 45 year-old woman who was diagnosed with bilateral C5-6 and C6-7 root outlet obstruction due to disco-arthritic lesions. She underwent ACDF C5-7 and the surgical notes state that the surgeon carefully liberated all four foraminal passages. Upon awakening, the patient did not feel good, and requested a new MRI. She was harshly denied one by her surgeon. She visited her GP, who called the hospital’s radiology department who also denied her a new spine MRI. She went privately, and received a report that the foraminae were within normal post-surgical limits. Ie., claiming successful intervention. Looking at the images, we see large beaks of uncovertebral arthritis that fill the right C6 and left C7 root outlets. Needless to say, this was a poorly done job. I recommended re-operation at a different hospital.

Another case. A 26 year-old male patient undergoes L5S1 microdiscectomy (right lateral recess decompression) due to refractory radiculopathy ongoing for several years. As can be seen in the images below, there is a complex disc herniation mainly compressing the right, but also the left descending S1 root. After surgery, he feels better on the right side for a short period, but the left gets worse and worse. Moreover, the right-sided pain returns. He has another MRI, and the radiologists notices the post-surgical changes but is perplexed by the perpetuated bilateral recess stenosis. The patient has a followup with the surgeon, who looks at the images, looks him right in the eye, and tells him that the images look normal. Clearly, this is not normal. I recommended revision surgery at another hospital.

Failed back surgery syndrome. Or is it?
A 55 year-old female patient develops strong low back pain with diffuse radicular pains over a period of many years, and was struggling to walk. MRI was done, showing central canal stenosis at the L3-4 and L5S1 levels. She undergoes bi-level microdiscectomy and flavectomy for canal decompression. After the surgery, her symptoms remained similar and she still couldn’t walk well. She was diagnosed with failed back surgery syndrome. When she visited my clinic, she struggled to perform low back extension, and had positive Lasegue’s tests in extension. She could not walk while maintaining lumbosacral extension. The images show aggressive foraminal (arthritic) stenosis in the L3-4, 4-5 and L5S1 levels which had not been diagnosed nor treated. I recommended multilevel foraminotomy.

Treatment pitfalls
The most common treatment pitfalls involve poor understanding of the pathomechanism of the patient’s pain generators. First and foremost, it is important to understand that symptomatic stenosis due to arthritis cannot be treated conservatively in the lower back, but can possibly be ameliorated (if it is mild to moderate) in the cervical spine. Explaining this in detail is outside of the scope of this article, but briefly, it is because spinogenic low back pain develops due to extension deficit and poor erector function, whereas cervical spine dysfunction generally develops in “hinge”-patterns, ie. hyperextended patterns. Reducing the extension by making the neck “long” in cervical spine dysfunction will increase foraminal diameter, whereas extension therapy for the low back will reduce foraminal diameter. I will attach some videos explaining this. As a general rule, consider symptomatic arthritogenic root stenosis to be a surgical matter.
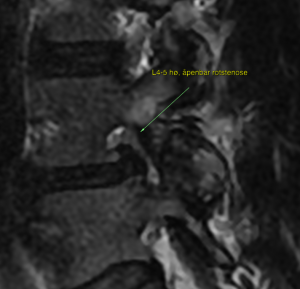
Another pitfall is radiculopathy due to chronic root stenosis in the presence of small disc herniations. Small disc herniations may sound like less of a problem, but reality is that these should not cause root compression. When they do, it tends to be because the canal was narrow to begin with, and this can have quite a poor prognosis with conservative therapy. Below is the case of a 38 year-old male patient with chronic left-sided L5 dermatomal pain after deadlifting. It had been refractory for 8 years. Activities involving spinal flexion worsens his symptoms consistently. I review his MRI the first time and was not able to see a clear reason for his symptoms. We ordered a new MRI with very fine slice thickness (0.8 mm slices). Now we were able to identify thickening of the left descending L5 root in its L4-5 lateral recess, compressed between a very very small disc bulge and mild facetal hypertrophy on the opposite side. The MRI also shows the left L5 root thickened due to inflammation (arrow). EMG showed signs of chronic left L5 root pathology. This cannot be treated conservatively, as there was almost no pathology to treat. The disc lesion was minimal, and the likelihood of reducing it to a state of childhood is zero. Likewise, the very mild facetal hypertrophy is not reversible. I recommended either learning to live with it, or lateral recess decompression.
Beginning Modic changes tend to improve with appropriate low back therapy if the majority of its intervertebral disc height is intact. However, if there is poor disc height, the likelihood that the bony pathology will spread is high. In cases of aggressive active bone inflammation and low disc height, with compatible clinical indicators, this has poor conservative prognosis. I recommend installing a disc prosthesis. Ventral root ganglion neurolysis can also be done, but this is symptom relief only.
Legitimate central stenosis (ie. compression of the medulla or the cauda equina) should not be attempted treated with physical therapy, in my opinion. Mild postural corrections are acceptable, but a patient with legitimate central stenosis (this is often reported equivocally) should be careful with their spines, especially if it is in the cervical or thoracic spine. The lumbar spine (cauda equina) is less sensitive to compression than the medulla, but central stenosis must still be respected. Rest and mild activities, with follow-up imaging after 3-6 months is the best option in my opinion. Surgery should be considered. Patients with ligamentum flavum hypertrophy, small disc herniations and congenital stenosis have poor likelihoods of spontaneous recovery. Surgery is warranted.
When to consider surgery
Generally, surgery is considered “the last resort”. Personally, I have a more balanced view on this. There are two main factors to consider:
- Risk of permanent damage unless operating (eg. central stenosis or severe root compression with paresis)
- Excruciating pain with an obvious etiology identified on imaging
- Poor prognosis with conservative treatment (eg. foramen filled with arthritis, or disc height reduction with aggressive refractory inflammatory Modic changes, refractory stenosis due to congenital pre-stenosis)
- Central stenosis
- Central stenosis with myelopathy requires surgery without exceptions
- Fusion: Lumbar fusion is generally not a good idea. It tends to work well in the neck, but in the low back, it tends to have a poor resolution rate and high complication rate, especially when done without the right indications. Lumbar fusions equipment also cause a lot of imaging artefacts, making it difficult to evaluate MRIs if something goes wrong. It should only be done if there is aggressive listhesis or other causes of instability that absolutely require surgical fixation. The bar for when to consider fusion should be higher in younger patients and lower in older patients (55+).
References
- World Health Organization. Priority diseases and reasons for inclusion: Low back pain. Web article. Available from: https://www.who.int/medicines/areas/priority_medicines/Ch6_24LBP.pdf
- Genebra CVDS, Maciel NM, Bento TPF, Simeão SFAP, Vitta A. Prevalence and factors associated with neck pain: a population-based study. Braz J Phys Ther. 2017;21(4):274-280. doi:10.1016/j.bjpt.2017.05.005
- Selmonosky CA, The diagnosis of thoracic outlet syndrome. Myths and Facts. Chilean J of Surg 2008 June; 60(3):255-261.
- Larsen K. How to truly identify and treat thoracic outlet syndrome (TOS). Web blog, 2018. Available from: https://mskneurology.com/how-truly-treat-thoracic-outlet-syndrome/
- Salardini A, Biller J. The hospital neurology book. McGraw Hill publishing, 2016
- Ross JS, Moore KR. Diagnostic imaging: Spine, 3rd edition. Elsevier publishing, 2015.
- Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome. Part one: A common yet little-known cause of chronic pelvic and lower extremity pain. Anaesth pain & intensiv care 2019;23(2):124-137
Hi Dr. Kjetil! Does the correction of lumbosacral extension apply (posture) if there has been a lumbar fixation done (L5-S1 levels)? I mean after the surgical procedure (fixation). Thank you!
Lumbar fusion is generally a really bad idea. It tends to work well in the neck, but in the low back, it tends to have a poor resolution rate and high complication rate. It should only be done if there is aggressive listhesis or other causes that absolutely require surgical fixation. The bar for when to consider fusion should be higher in younger patients and lower in older patients (55+).
Now, to your question. If they have used angled rods that maintain the lumbar lordosis, then light postural correctives can be done to encourage erector activation and function. However, I see lots of patients with fused lumbar spines and untreated foraminal stenoses. Therefore, there’s no guarantee that this will help.
Fusion cases really have to be evaluated individually.
Hi, I really appreciate the time, knowledge, and effort you give in this website. My MRI came back with mild-moderate spinal canal stenosis at C6-C7 (there is a central disc protrusion), mild stenosis at C5-C6 (a posterior disc osteophyte complex), and minimal C4-C5.
C3-C4 and C4-C5 mention a disc bulge. C3-C4 “contacting” the ventral thecae sac C4-C5 “indenting.” Reversal of the normal cervical lordosis without spondylolisthesis. I have only noticed problems in my cervical region since May 20. My primary reason for going to the doctor was the hand numbness (sometimes felt very cold and I would carry a HotHands pack), along with what seemed to me to be TOS-like symptoms.
Some symptoms are definitely worse in the evening (numbness in left hand, discomfort at the end of my middle finger, muscle pain in muscle between thumb/1st finger, twitching in the muscle below my 5th finger & muscles near the ulna.) During the EMG, the doctor said I do not have carpel tunnel syndrome. During the day, I feel mostly normal (I am better if I am up and active) but symptoms have gotten worse and I take ibuprofen 800mg, and tizanidine 2mg earlier in the day.
Driving is very aggravating to the symptoms: reaching for seatbelt to put it on, turning head to check blind spot, steering with left hand/arm, sitting in the seat (scapular pain/neck) to name a few.
I also now have issues with urgency incontinence, adipsia (and symptoms of dehydration), muscular tinnitus (right side only, when laying on my right side- the tizanidine seems to help with this).
I am often very tense and almost afraid to move, but I don’t realize I am tensing my shoulders, etc. Pushing below my clavical left side (dorsal or ventral side) aggravates symptoms.
I am just a confused, science teacher, pharmacy school drop-out. Can TOS cause these spinal issues because of my tense, angry muscles? Or do the spinal issues lead to the TOS-like symptoms that really isn’t TOS? Thank you in advance.
Hi, to review something like this you’ll need to book a consultation.