Postural orthostatic tachycardia syndrome (POTS) is regarded as a chronic but generally idiopathic dysfunction of the autonomic nervous system, ie., the system that regulates automatic processes such as blood vessel dilation and narrowing. In addition to the postural tachycardia that develops, these patients tend to suffer from profound fatigue, syncopal or presyncopal events, migraines, vestibular dysfunction, tinnitus, occipital headaches, cognitive impairment, and more (Garland et al., 2015). In severe cases, transient but aggressive stroke-like symptoms may occur when standing up and render the patient wheelchair bound. Severe sufferers often see gradual worsening, whilst others may be able to maintain their symptoms at a stable level.
This article will explain postural orthostatic tachycardia syndrome from another perspective, somewhat in opposition to the common consensus on the topic, which I believe to be wrong in some areas, and sometimes harmful to the patients receiving treatment. This, especially regarding improper treatment using vasopressors like Midodrine, or hypovolemic treatment with sodium. There is room for these agents in POTS, but it must be timed properly to avoid worsening the underlying condition, which I strongly believe is forced cranioarterial vasodilation due to underlying cranioarterial hyperperfusion. This is also the underlying reason for why many patients develop POTS after a traumatic or spontaneous CSF leak, with or without normal CSF pressure levels. I will explain this mechanism later in this article. Many patients also develop POTS after certain infections, and especially coronavirus. Coronavirus sets off an inflammatory response called cytokine activity. This activity is heavily vasodilatory, and this vasodilatory response seems to stay for long after the body has ridden itself of coronavirus. High stress and anxiety are also very common preexisting problems in patients with POTS. This is relevant, because high stress levels predisposes for raised craniovascular pressures both physically due to involuntary Valsalva activity (“bracing”), but also due to raised sympathetic tone. Neck or head injuries can also cause POTS, as they can alter craniovascular perfusion rates.
It is important to remember that although there forelies some literature consensus on POTS, it is still largely considered an idiopathic condition, meaning that its pathomechanism is not fully understood. Without a valid explanation of mechanism, treatment strategies can not be soberly developed. There must therefore be room for critical thinking and also room for challenges to the established consensus. No one is right all the time, and this article is, naturally, not intended as direct criticism or mockery of other POTS researchers.
POTS and its associations
As stated, POTS is considered to be a dysautonomic problem that causes excessive vasodilation. Causes such as autoimmune autonomic neuropathy, poor venous return- which is adhered to the formerly mentioned, and mast cell activation syndrome. Despite these postulations, however, most POTS patients do not demonstrate significant amount of neuroantibodies nor mast cell activity in workups, and thus the two clinical entities are considered controversial as a cause of POTS (Li 2014, Wang 2012, Shibao 2005). Paradoxically, they are also affected by hypersympathetic tone, which would seem contradictory considering the vasodilatory nature of the syndrome. Patients with POTS are also quite frequently hypermobile, and many are diagnosed with disorders such as Ehler Danlos syndrome. That said, general vessel wall integrity has not been proven to be the cause of POTS, as tonometry of the large vessels in this patient group tends to be normal (Cheng et al., 2017).
Empirically, I have found that POTS, in most cases (and I can only speak for the patients that I have examined) is a craniovascular problem with systemic sequelae — Not originally a systemic problem. It might certainly be worsened or set off by occurrences such as a CSF leak, cytokine reaction to infection (such as coronavirus), allergic reaction, etc. I believe that these factors are “last drop”-phenomenons and amplifiers, rather than the disorder’s real etiology.
A proposed mechanism for POTS
The symptoms seen in POTS are paradoxical. Most POTS patients suffer from pre-existing fatigue, neck and shoulder pain (or even “fibromyalgia” or small-fiber neuropathy, which are often umbrella diagnoses of little clinical value, unless there are legitimate underlying causes such as diabetes, autoimmune neuropathy, or similar), migraines, etc. Moreover, these patients tend to demonstrate signs of raised arterial blood pressures on doppler ultrasound examinations of the neck, which would seem contradictory as the patient suffers from low blood pressure. Even when upright, the patient demonstrates high pressure waveforms.

Fig. 1. Compression exerted by the scalenus and pectoralis minor muscles, ie., distal to the carotid and vertebral branches, will result in retrograded flow and hyperprefusion toward the head (Larsen et al., 2020).
Fundus images (retinal photos, ie., pictures showing the back of the eye) often demonstrate subtle retino-hypertensive findings such as arteriovenous “nicking” and “copper wiring”. Copper wiring means that the arteriolar light reflex is increased due to increased arteriolar wall fatty buildup (this happens when the pressure is raised over time). AV nicking means that the veins over whom the arteriole crosses, gets pinched (compressed) by the hardened hypertensive arteriole. They may also frequently demonstrate hypertensive vasospasm, which means that all of the arterioles are diffusely constricted. These findings are subtle and are rarely documented by the ophthalmologist before the patient starts to develop small infarctions of the retina, which does not tend to happen with this patient group. Moreover, the optic disc generally appears normal or only mildly swollen.

Fig. 2. Subtle AV nicking (green arrows), copper wiring (blue arrows) and gentle elevation of the papilla (yellow arrow)
What is causing these raised cranial blood pressures, and why can it result in POTS? A thoracic outlet syndrome-induced craniovascular hyperperfusion phenomenon (TOS CVH) seems to be the main cause of cerebrovascular dysregulation. TOS CVH is a problem where mild to moderate-, but continuous compression of the subclavian arteries result in retrograded flow towards the head, through the carotid and vertebral arteries (Larsen et al. 2020). This results in the head being fed more blood than it is able to consume, to which it is quite sensitive. This causes cerebrovacular congestion and hypertension. High cerebral blood pressures are well-known for causing derangement in cerebral autoregulation, which is the system that maintains normal bloodpressures in the head. Gradual hyperdilation of the intracranial arteries will occur with these patients, mainly when lying down, as cerebral blood flow (CBF) in general, especially combined with he CVH phenomenon, tremendously increases blood flow when lying down (Garrett 2017, Larsen 2020).

Fig. 3. Obvious extracranial vascular dilation when lying completely supine, improvement when flexing the neck (the very small and soft pillow in the upper left image should not be confused with the large and hard pillow that is used to flex the neck in the two lower images)
The body can relatiely easily compensate for reduced blood flow to the head when occurring over time. Take carotid atherosclerosis, for instance, where it is well-known that carotid stenosis due to plaque is often asymptomatic until 70% narrowing (Pellerito & Polak, 2013). The body compensates for the reduced flow by inducing vasoconstriction to maintain homeostasis. When the perfusion rates increase, however, and especially when increased over time, this is harder to compensate for. Intracranial arterial vasodiolation will certainly permit a greater volume of blood to enter the head, but it does not increase consumption and can thus, still, not protect well against the CVH phenomenon. What it does then, is reduce cardiac output and induce peripheral vasodilation. This will result in the paradoxical situation where body pressures are low because head pressures are high, and that’s exactly what happens in these patients.
Excessive vasodilation with simultaneous hypertension is a vulnerable state for the arteries. It greatly predisposes for POTS, migraines, vestibular dysfunction, tinnitus, brain fog, memory loss, etc. (Larsen et al., 2020). But in severe circumstances, the CVH phenomenon can cause seizures or hemorrhages (Marchi 2007; Friedman 2009; Jha 2003). It is also known that hyperperfusion can impair the blood brain barrier (Ivens et al., 2010).
The patient will usually be asymptomatic, at least with regards to tachycardia as long as they are lying down. The cognitive dysfunction, fatigue, dizziness, migraines, etc., are still usually present even if the patient lies down a lot, but worsens with exertion as well. This is because the cerebral blood pressure is high when lying down, and the intensity will depend on various factors, especially the severity of the CVH effect. When standing up, CBF naturally decreases, as the blood now also needs to support your muscles to maintain erect position, and the heart also has to pump the blood vertically against gravity rather than horizontally. This results in reduced cranial blood pressures, but is normally compensated for by induced vasoconstriction through neurogenic autoregulation. Because this function is impaired, and gradually so, a variable degree of acute postural hypotension and hypoperfusion will occur, meaning that the brain – that was getting oversaturated by blood when lying down – is now paradoxically undersaturated when standing up. This will immediately prompt a hypersympathetic reaction to induce peripheral vasoconstriction and significantly increase cardiac output and frequency.
There is a secondary protective mechanism for this. As well known in ICU settings, raised intracranial pressure (ICP: a term that really means CSF pressure, it does not mean vascular pressure) can cause ischemic strokes. This may seem irrelevant, but the point here is that raised ICP will force vasoconstriction due to external pressure, rather than the muscles of the arteries constricting (neurogenic/autonomic vasoconstriction). Studies have shown, albeit old studies (Pickering 1934, 1952; Shelburne 1932; Taylor 1954), that raised systemic blood pressures will cause raised ICP. I strongly believe that this is a protective response by the body to protect the cerebral arterial vessels from damage due to raised pressure. This would seem fitting with the many reports where malign hypertension is seen in concurrence with papilledema. Simultaneously, LOW CSF pressures would permit excessive cerebral vasodilation, and then especially if the primary regulatory systemic (autonomic vasoconstriction) is impaired by longstanding CVH. This would potentially explain why so many patients develop POTS “spontaneously” after, eg., a lumbar puncture or minor spontaneous CSF leak despite having normal CSF opening pressures. It also explains why taking acetazolamide (a drug that reduces CSF pressures by decreasing its production) makes these patients worse.
Patients with hypermobility are certainly more prone to developing CSF leaks than other patients (Schiewink 2004). They also seem to be more prone to general hypotension, which can be a predisposing factor. If such a patient develops TOS CVH (usually caused either by very high stress and poor posture, or head/neck trauma), they are much more susceptible to developing POTS than a patient with inherently normal blood pressure and tissue integrity. Further, as stated, many of these patients, and I am especially talking about patients who develop these problems without having suffered neck or head trauma, tend to suffer from preexisting anxiety and high stress.
To explain it simply, very high isolated head blood pressures (this will not show un a cuff exam for the arm, as it will show normal or even low pressures) will force cerebral arterial vasodilation, impair the cerebral autoregulatory system, and thus result in the paradoxical situation where head pressures are very high when lying down and very low when erected.
POTS and fatigue
Patients with POTS often suffer from symptoms similar to myalgic encephalomyelitis, and in my experience they have a similar cause. Why do these patients develop such severe fatigue, are more prone to infections, allergic reactions, and so on? I believe it has to do with the adrenal response that follows the CVH effect.
First and foremost, high cerebral blood pressures – with out without frank POTS – will result in autoregulative measures to decrease cardiac output and systemic blood pressures. This, in attempt to reduce the hypertensive burden on the brain. Even in solitude, this causes fatigue and various other symptoms. Now, as already stated clearly, when happening over the course of months and usually years, cerebral autoregulation becomes impaired to various extents. Every time the patient is upright, a paradoxical hypersympathetic response will occur to increase blood pressure, as the body needs a certain pressure to function. This means that, although the pressure is very high when lying down, the pressure gets so low when standing up that, without engaging the sympathetic system (through secretion of adrenaline and cortisol), the patient will pass out. When this happens every time the patient stands up or even remotely exerts themselves, adrenal burnout will often be the result. This causes further fatigue, brain fog, depression, cognitive decline, and immunosupression. It is thus a difficult problem to manage, because you’re damned if you do and damned if you don’t. Lying down may make you feel better, but worsens the hyperdilatory problem and autoregulation. Standing up and being active causes, often, severe adrenal burnout with its own associated constellation of symptoms.
Because of the pre-existing, aggressive load that these patients have on the adrenal system, I recommend being careful with stimulant use (eg. coffee), and physical strain (eg. exercise). If strain is inevitable, then being well prepared (drug timing, as detailed further down) will help.
Cofactors in the development of POTS
It should be evident by now that I consider cerebroarterial hyperdilation the main cause, or factor, in the development of POTS, and that this problem is usually caused by thoracic outlet syndrome. TOS is a very, very common problem amongst both whiplash and anxiety patients. However, I will touch upon other relevant comorbidities that are involved in the development of this problem.
Anxiety and high stress is probably the most important cofactor to consider, and to treat. This, especially, if the patient has developed POTS without history of neck or head trauma. In many circumstances, this manifests in the form of “bracing”. Bracing means that the patient, due to feeling poorly, “braces” themselves, or “clenches” their muscles, as an subconscious way to feel safe. I have written an article on this topic (link), which might just be the most improtant but also least appreciated piece of work on my website. “Clenching” causes high sympathetic tone, but also directly increases arterial, venous and CSF pressures via continuous but involuntary Valsalva maneuvers. To give an example: White coat syndrome, ie., fear of doctors of health anxiety is often something shrugged off as benign, for instance if the patient gets their blood pressure taken and it’s elevated or even skyrocketing. The patient will be told that it’s just anxiety, and nothing to worry about. But thinking about this a little more clearly, it would also mean that the higher the patient’s stress and anxiety levels, the higher their blood pressures. It also causes musculoskeletal dysfunction, as seen in the linked article.
This problem, when very prevalent, is highly toxic for the patient and they should work heavily on stopping their bracing habits. It is my experience that patients who brace and train themselves to brace less, even if the psychiatric state is the same. Consider it like changing a poor habit. Women are usually better at identifying and dealing with this than men are, perhaps because women are better at listening to their bodies. Do not underestimate this problem.
Jugular vein stenosis and CSF leaks. Jugular vein, or even dural sinus stenosis is a topic that has received much attention the recent years. Already in 1999, Seoane & Rhoton showed that severe jugular vein stenosis, if continuous, could result in cerebellar hemorrhage. This is rare, of course, and in this study happened during an awkward position during surgery. They concluded that this could be an important predisposing factor in the development of cerebellar hemorrhage during supratentorial craniotomy. Later on, in 2012, Jayaraman et al. showed that, coincidentally, 70% of patients that were admitted to the neurology ward and undergoing MRA, also turned out to have jugular vein stenosis. They postulated that its involvement in diffuse neurological disorders was likely, and noted that this problem was highly underreported. Ding et al (2019) found that 90% of patients with cervical spondylosis had jugular vein stenosis, showing that this is a very common disorder. It usually manifests with fatigue, brain fog, diffuse headaches or migraines,
Internal jugular vein stenosis usually happens at the C1 level, being positionally compressed by the C1 transverse process, or impinged between it and the styloid process in front. This phenomenon has been given various names, but I have called it jugular outlet syndrome. In many circumstances, this will result in venous hypertension. Many, mistakenly, believe that venous hypertension is benign if it does not cause papilledema (very high CSF pressures). This is not true. Firstly, it is important to understand that venous outlet obstruction literally means that the head is unable to efficiently rid itself of used blood. Moreover, venous hypertension raises both arterial, venous and CSF pressures, due to drainage congestion. Chronic increases of CSF pressure due to venous drainage impairment will often result in a spontaneous CSF leak, a small defect in the dura as it “gives in” to the pressure. Trying to heal this with a blood patch is futile, as it will either result in a new leak, or recurrent CSF hypertension. Higgins et al (2014, 2019) found that resolution of venous drainage impairment also resulted in spontaneous healing of the CSF leak in many of their patients. This suggests that the dura is able to self-repair if the CSF pressure is, and stays normal. It would also offer explanation as to why some suffer severe side effects from lumbar punctures, whereas others are fine and recovery right away. As I have already explained, CSF pressures may also rise to protect arteries from hyperdilating in incidences of generalized arterial as well as craniovascular hyperperfusion (as seen in TOS), so the venous part is not the only thing to consider.

Fig. 4. Poor posture, upper cervical facetal misalignment and jugular vein obstruction often go hand in hand.
Paradoxical hypovolemia. Empirically, it seems that the body sheds fluids in this patient group, gradually causing and worsening legitimate hypovolemia. This, again, as an attempt to reduce head pressures. And although it may have some success in doing so, it will also worsen the orthostatic intolerance and worsen the adrenal response that is seen in these patients. Replenishing fluids and salt will make it worse unless it is timed properly, and the head pressure is dealt with simultaneously.
POTS and viral infections. Some viral infections, especially coronavirus, can cause aggressive cytokine activity. I have personally had it, and had elevated heart rate for a long time afterwards, for more than a year, long after the infection was over. It seems that these agents cause long-lasting changes in vessel diameter (vasodilation). If you have underlying conditions such as EDS and migraines, getting a strong cytokine-inducing infection may be the last drop to trigger full blown POTS. For “normal” patients with mild elevations in heart rate, or fatigue after undergoing one of these infections, taking salt and water, and increasing heart strength and endurance may be helpful, but must be done gradually. For patients with POTS, I recommend treating the underlying [main] conditions first, as will be discussed later in this article.
Instability of the upper spine (AAI and CCI). Although jugular vein stenosis by the C1 may technically qualify as misalignment of the atlanto-occipital joints, as seen in some of AAI CCI expert Atul Goel’s papers (Goel, 2014), it is not really instability. Most of these patients (I am saying most, not all) demonstrate normal or nearly normal craniocervical measurements. Personally, I find these diagnoses heavily over-diagnosed by the alternative chronic pain community, and I do not agree that this problem is relevant to POTS. See my atlantoaxial instability article (link) for more information on potential problems. I know that some claim craniocervical fusion to help these patients, but I cannot agree to that. I can certainly agree that some of these patients may benefit from strengthening their upper necks, but other than potentially improving jugular outlet drainage, which is also important, it will not resolve POTS.
Diagnostic workup
POTS is a multifactorial problem. Although the main cause, in my experience, seems to be TOS CVH. As mentioned repeatedly, TOS increases cranioarterial perfusion rates by exerting mild to moderate, but continuous pressure on the subclavian arteries in the interscalene triangle and beneath the pectoralis minor. The compression that occurs under the collarbone, ie., in the costoclavicular space, is usually intermittent and plays a lesser role in POTS. The brain is relatively adaptable to fluctuations in pressures as long as they are intermittent.
Unfortunately, thoracic outlet syndrome is a controversial clinical entitity, and is difficult to diagnose. I have lost track of the amount of TOS patients I have treated who have been “cleared” for TOS by their physicians. TOS is mainly a clinical diagnosis, meaning that it’s mainly diagnosed based on clinical signs and tests rather than, eg., imaging. Neurography is another popular examination used in TOS that has extremely low value, as up to 90% of patients with TOS demonstrate completely normal neurographies (Rousseff et al., 2005). Most patients with TOS one or more of the following symptoms: Pain in the back of the head / upper neck (this is a vascular headache that tends to worsen when lying down — it is not an “atlas problem”), pain in the neck, chest, arms, shoulder blade or between the shoulder blades that worsen when or after carrying something or working with the arms (eg., cleaning windows, carrying groceries). Shortness of breath is also somewhat common.
What about the angiographies, then? The first problem is that only 5-10% of patients with TOS have severe compression on angiographies, and this compression is generally seen at the costoclavicular space (under the collar bone). This is a positional compression and is thus less important in the pathogenesis of POTS. It is possible to see decreased contrast intensity in the coronal plane on CTA in some circumstances, ie., in the subpectoral and interscalene triangle, but the changes are subtle and it is underreported. TOS is mainly diagnosed by expert surgeons with long experience in this exact problem. Someone who sees TOS twice per year, is only likely to catch the most obivous cases. Moreover, many surgeons are very uncomfortable diagnosing TOS in a patient who has preexisting diagnoses like Myalgic encephalomyelitis, fibromyalgia, dysautonomia, etc. Firstly, because it is a controversial diagnosis to begin with, and second, because they fear that there is too many other things going on that may interfere with the patients symptoms and thus prevent improvement after surgery.
I suggest reading my TOS article (link) as well as reviewing my TOS diagnosis video on youtube (link). It is also important to review my TOS CVH paper (link). It is important that patients are aware of the conventional diagnostic process in TOS, because TOS CVH is a virtually unknown problem. Being diagnosed for TOS is astronomically more likely than being diagnosed with TOS CVH, unless it is done by myself. That said, as for the real problem, being TOS CVH, there are several things we look for.
Duplex ultrasound
Conventionally, the ultrasound exam (only if performed by someone who understands TOS well), can have higher sensitivity than the CT or MR angiographies. The reason why is that you can do more provocative positions that would be difficult (not impossible, per se) on MRA or CTA, either because you get movement artefacts or due to doubled radiation.
TOS: I recommend looking for signs of hypoperfusion in the axillary (or, slightly more sensitive in the radial or ulnar arteries) with the arm in neutral, arms up, and shoulder squeezed “back and down” (Eden’s test position). This is for conventional TOS, although, as stated, it will help you with getting a TOS diagnosis if the exam is positive, but is not really the main problem in POTS. You will often see low systolic velocities even in neutral position (normal tends to be about 100cm/s or a little higher), and then obvious reduction or even tardus parvus waveforms with the arms elevated or Eden’s position.

Fig. 5. Doppler exam of the axillary artery in a patient with TOS. In this patient, it was only positive with the arm elevated.
TOS CVH: In TOS CVH you look for signs of elevated pressure in the carotid and vertebral arteries. Ultrasound has a blatant advantage in this screening, as it will give an impression of pressure status. This is completely omitted in an MRA or CTA exam, which only gives visual input as to whether or not there is flow obstruction. In initial stages, CVH waveforms manifest with increased pulsatility. In later stages, flow velocities decrease (this must not be interpreted as low flow, it is caused by distal hypersaturation), blunted systolic peaks with a slow upstroke and usually rapid diastolic decline. In severe cases, it can be difficult to identify the diastolic transition because the congestion is massive. See my CVH paper for the images of what this looks like. Aberrancies here are almost always reported as normal, becuase althogh the examiner can see that the waveforms are abnormal, they don’t know why, and thus leave it out. I have seen numerous cases of blatantly abnormal doppler exams being reported as normal in CVH cases.

Fig. 6. Extremely abnormal doppler waveforms in a patient with severe left-sided TOS (the left arm was completely paretic), and severe ME.
Duplex Volume flow ultrasound can also be used to measure the jugular veins, and it has the advantage of being able to place the patient in various neck positions to evaluate positional obstruction of venous outflow. Normal combined flow through both internal jugular veins combined is about 800-1200mL/min (Müller 1985, Brunhölzl 1990, Özen 2014). Özen et al., in their novel 2014 study, found that flow volumes lower than 150 mL/min were associated with severe flow obstruction seen on MRV, where as volumes lower than 55mL/min were associated with occlusive states, either due to thrombosis, severe sinus stenosis or severe jugular vein compression. Doing the exam upright is usually not helpful, as the veins naturally collapse in upright position. However, doing it in neutral, with the neck extended, flexed, and rotation may prove fruitful in some circumstances. The same applies for CVH, where arms up may also be done.
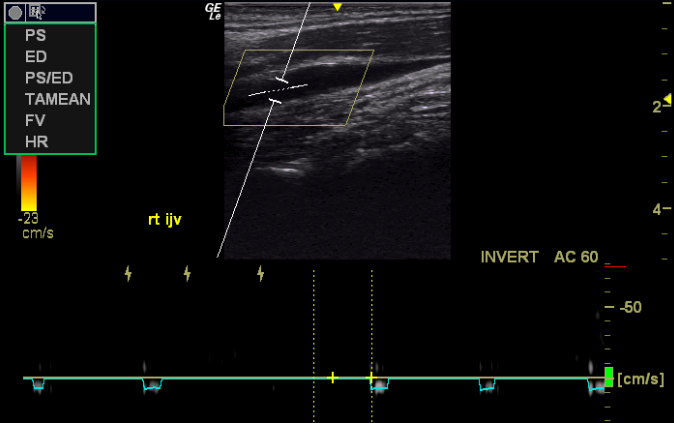
Fig. 7. Complete occlusion of the right jugular vein in a patient with severe fatigue
CT angiography. The contrasted CT scan is quite helpful, because you get so much information from it. Timing the contrast properly, you can get great views of both the arterial and venous flow in the same images. If you also raise the arms, you can get beautiful head, neck and subclavian images in one single study. We generally look for narrowing of the intradural or internal jugular veins, and narrowing of the subclavian arteries as seen in TOS. If the CT shows severe venous stenosis, a follow-up exam (catheter venography and manometry) may be done to evaluate the pressures inside of the veins. Technically, the manometry should also be able to prove the raised carotid arterial pressures, but this is so far untested.
Ocular USD: Doppler examination of the central retinal artery may show blunted systolic peaks, similar to what is seen in the internal carotid arteries. Transocular imaging may also, with greater sensitivity than MRI, reveal dilated optic nerve sheaths.

Fig. 8. Virtually normal optic nerve sheath diameter, but flattening of the posterior orbit and abnormal, blunted systolic waveforms in the central retinal artery in a patient with TOS and severe headache.
Brain MRI is usually normal, but can show gentle dilation of the lateral ventricles in some incidences, or dilated optic nerve sheaths (higher than 5.8mm Ø). Hypertensive encephalopathy (HE) is usually avoided due to the compensatory nature of CVH, but it cannot be excluded that TOS CVH is involved in some, seemingly idiopathic incidences of HE. I still recommend performing a typical MRI of the neck and head for a generalized exam.
Fundus images, meaning retinography, may frequently show subtle signs of hypertensive retinopathy in cases of TOS CVH. AV nicking and subtle copper wiring is common, but quite underreported or even often deemed normal, as it’s seen in patients with normal blood pressures (the examiner now being familiar with the CVH effect). Vasospasm is also common, but again, very underreported. Rose et al. (2010) found that migraine patients demonstrated a tendency toward hypertensive retinopathy despite being normo- or even hypotensive.

Fig. 9. Diffuse vasospasm. This can be difficult to spot unless you see retinas all day long. My friend who is an opthalmologist helped me to diagnose this patient, who also had POTS and severe TOS CVH.
Stress anxiety. The patient should screen themselves for bracing patterns, even if they think they don’t have it. Men are the worst in this respect, but women are usually quite aware if they tend to be tense. There are also ways for the clinician to investigate this, cf. my bracing article that was linked earlier. Many patients with this problem report some improvement with amitriptyline, which is generally a very safe and tolerated drug without addictive features nor a lot of side effects. The drug has some contraindications, so talk to your physician before making any decisions. Other drugs like SSRIs or SNRIs can also be attempted with the cooperation of your physician.
Upper cervical instability. As already explained, I highly disagree that this is a common problem in patients with POTS. CCI and AAI, in legitimate cases of surgical nature, will demonstrate brainstem compression, Cock-Robin syndrome, Bow hunter’s syndrome that severely and conspicuously trigger with cervical rotation (for AAI) or flexion or extension (for CCI). If you feel poorly regardless of what position you are in, or if your main trigger is orthostatic intolerance rather than intolerance to neck movement, you can probably cross these two problems off your list. Now, if you do suspect legitimate CCI or AAI, the imaging is potentially extensive and it depends on what your exact symptom are. If you pass out when you turn to the sides, you may have a warrant for dynamic angiography. If your neck locks, then a dynamic CT without contrast will do. If you develop a lhermitte’s sign when you extend your neck, a flexion/extension MRI of the neck is warranted. It doesn’t need to be upright; the movements themselves are enough.
Treatment strategies for POTS
As clearly stated, the literature consensus is that the exact cause of POTS is unknown. Therefore, all treatment protocols must be considered somewhat experimental. My experience is that it is important to treat the CVH phenomenon sooner rather than later, as the degree of impairment of cerebral autoregulation will make it harder to recover.
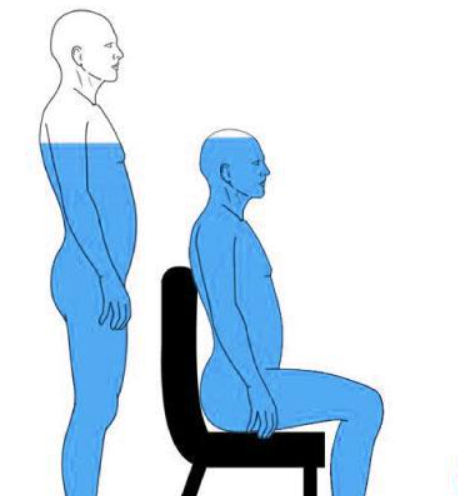
Conservatively, several steps can be done. Firstly, avoid lying completely flat (Larsen 2020). This reduces cerebral blood flow and thus also the craniovascular pressures. Use a bed wedge and a tall neck pillow, but don’t raise your back so much that you get tachycardia. Look for the sweet spot, if possible, that reduces head pressures but does not increase sympathetic tone. I have seen even severely affected (wheelchair bound) patients get better from doing this. This will directly prevent worsening of cerebral vasodilatory states, which is extremely important.
Stretching or botox injections to the pectoralis minor muscles can be done in many cases, if there is clinical indication. This can help a lot if there is an actual problem there. Stretching of the scalenes tend to make them worse, and botox of the scalenus muscles should ONLY be done if you have already decided that you want to go for surgery. The scalenes do not recovery well, if at all, from botox injections. It is also crucial to stop bracing and to stop holding your breath, that is, if you have this habit, to reduce the load on the accessory respiratory muscles (such as the scalenes). Upper cervical treatments for jugular vein compression can also be helpful, especially neck postural corrections, as postural dysfunction is hte main cause of jugulra vein compression (Larsen 2018). Pulling your shoulders a little bit back will stretch the pec minor and thus increase head pressures when you are standing and walking, and may thus decrease the sympathetic response somewhat, but this trick should certainly be avoided when lying down.
With regards to activity, then I recommend avoiding full exertion, as this will strain the adrenal glands unnecessarily, which makes for longer recovery times and greater vulnerability to infectious illness due to its adherent immunosupression. Moreover, I recommend timing salt and drug use to compliment your activities.
Drug and salt use: It is critical to understand the mechanism of POTS. If you don’t, some treatment strategies can make you worse. The whole point here, is that pressures are very high when lying down and very low when standing up. Thus, taking salt, midodrine or desmopressin before lying down for a longer period of time is a really bad idea, as it will worsen the head pressure. Especially so if done over time. Midodrine has a half life of approximately 5 hours, and should be taken prior to standing up, for instance in the morning before going to work. The same concept goes when planning desmopressin use, which stays in your body for about 10 hours total. If you are disabled and lie down all day, taking these drugs can be potentially dangerous, unless timed very carefully. Salt and water should be timed similarly to Midodrine. I would not recommend using it if you are only going to be upright for one or two hours, and if you do, you should certainly avoid lying flat after you get back home. Use a bed wedge. Now, when it comes to lying down, I recommend using vasodilator like candesartan or equivalent. Candesartan is an angiotensin II inhibitor, meaning that it decreases vasoconstriction. It has a half-life of approx 9 hours, so it is often helpful to take it a few hours before bed-time in order to get it out of your system within reasonable time after waking up the next day. This will, thus, aid somewhat in reducing head pressures when lying down and therefore also help in preventing progressive impairment of cerebral autoregulation and cerebroarterial hypervasodilation. Taking it before standing up (for a longer period of time) will worsen the orthostatic hypovolemia.
Finally, the importance of stress mastery or anxiolytic treatment cannot be stated enough for this patient group, especially if they developed this problem without a history of neck or head trauma.
Possible surgical routes: The most obvious intervention to resolve the CVH problem is TOS decompressive surgery. This is a good surgery when done right, but few surgeons have a lot of experience with it. It is important that, if you choose to get this done, it should be done by someone who does it often and knows it well. The standard surgery is partial removal of the first rib, and snipping the anterior scalene. This will resolve the compression of the subclavian artery in both the costoclavicular and interscalene triangles. Tenotomy of the pectoralis minor can also be done, but is generally not needed, as it responds well to appropriate physical therapy. If no such competent therapy is available (which it is often not, when it comes to TOS), then tenotomy or botox might be preferable.
Surgical liberation of the subclavian artery will immediately, and potentially severely reduce brain pressures when lying down. However, the vasodilatory state will remain the same for some time, until the autoregulatory mechanism starts to work properly again. It is very important to understand that, because CBF reduces after liberation, and cerebro-arterial diameter remains the same, then POTS will increase after surgery until the vasodilation starts to reduce. That said, because the hyperperfusion problem is resolved, the patient should now be able to start increasing their salt and water intakes (regardless of position), to treat the hypovolemia, but take care and monitor your symptoms and heart rate. They will also benefit from taking Midodrine before being upright for several hours, but care should be taken. Propranolol should be ceased a few days prior to surgery. As the POTS gradually improves, gentle cardiovascular strengthening can be attempted, but this can be months after the procedure was done. It is not yet clear if all patients recover proper autoregulatory capacity or not, but it will certainly prevent further damage of the brain and its regulatory system.
If the patient has craniovenous outlet obstruction, it the treatment depends on its degree. If the jugular veins appear crushed on a CT venogram, it is very hard to treat this conservatively. Styloidectomy (full resection off its base) and transversectomy may be indicated especially if the manometry shows raised pressures (Zhao 2019, Dashti 2012). Balloon venoplasty can be tried if the stenosis is intracranial. If the supine images look normal, but only upright MRI shows venous obstruction, then this is usualy just a postural problem that can be treated conservatiely with good results. It is also important to note, here, that styloidectomy without postural improvement will not resolve the drainage problem.
References:
- Garland EM, Celedonio JE, Raj SR. Postural tachycardia syndrome: beyond orthostatic intolerance. Curr Neurol Neurosci Rep. 2015;15(9):60.
- Li H, Yu X, Liles C, et al. Autoimmune basis for postural tachycardia syndrome. J Am Heart Assoc. 2014;3(1):e000755.
- Wang XL, Chai Q, Charlesworth MC, et al. Autoimmunoreactive IgGs from patients with postural orthostatic tachycardia syndrome. Proteomics Clin Appl. 2012;6(11–12):615–625.
- Shibao C, Arzubiaga C, Roberts LJ, 2nd, et al. Hyperadrenergic postural tachycardia syndrome in mast cell activation disorders. Hypertension. 2005;45(3):385–390.
- Cheng JL, Au JS, Guzman JC, Morillo CA, MacDonald MJ. Cardiovascular profile in postural orthostatic tachycardia syndrome and Ehlers-Danlos syndrome type III. Clin Auton Res. 2017;27(2):113–116.
- Larsen K, Galluccio FC, Chand SK.Does thoracic outlet syndrome cause cerebrovascular hyperperfusion? Diagnostic markers for occult craniovascular congestion. Anaesth pain intensive care 2020;24(1)69-86. DOI: https://doi.org/10.35975/apic.v24i1.1230
- Garrett ZK, Pearson J, Subudhi AW. Postural effects on cerebral blood flow and autoregulation. Physiol Rep. 2017;5(4):e13150. doi:10.14814/phy2.13150
- Pellerito & Polak. Introduction to Vascular Ultrasonography, 6th edition. Elsevier publishing.
- Marchi N, Angelov L, Masaryk T, Fazio V, Granata T, Hernandez N, Hallene K, Diglaw T, Franic L, Najm I, Janigro D. Seizure-promoting effect of blood–brain barrier disruption. Epilepsia. 2007;48:732–742.
- Friedman A, Kaufer D, Heinemann U. Blood–brain barrier breakdown-inducing astrocytic transformation: novel targets for the prevention of epilepsy. Epilepsy Res. 2009;85:142–149.
- Jha SK. Cerebral Edema and its Management. Med J Armed Forces India. 2003;59(4):326–331. doi:10.1016/S0377.
- Ivens S, Gabriel S, Greenberg G, Friedman A, Shelef I. Blood–brain barrier breakdown as a novel mechanism underlying cerebral hyperperfusion syndrome. Journal of neurology. 2010;257(4):615-620. doi:10.1007/s00415-009-5384-z.
- Pickering GW. The cerebrospinal fluid pressure in arterial hypertension. Clin. Sc. 1: 397, 1934.
- Pickering GW. The pathogenesis of malignant hypertension. Circulation. 1952 Oct;6(4):599-612. doi: 10.1161/01.cir.6.4.599. PMID: 12979074.
- Shelburne SA, Blain D, O’hare JP. THE SPINAL FLUID IN HYPERTENSION. J Clin Invest. 1932 May;11(3):489-96. doi: 10.1172/JCI100428. PMID: 16694055; PMCID: PMC435830.
- Taylor RD, Corcoran AC, Page RH. INCREASED CEREBROSPINAL FLUID PRESSURE AND PAPILLEDEMA IN MALIGNANT HYPERTENSION. AMA Arch Intern Med. 1954;93(6):818-824. doi:10.1001/archinte.1954.00240300012002
- Schievink WI, Gordon OK, Tourje J. Connective tissue disorders with spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension: a prospective study. Neurosurgery. 2004 Jan;54(1):65-70; discussion 70-1. doi: 10.1227/01.neu.0000097200.18478.7b. PMID: 14683542.
- Seoane E, Rhoton AL Jr. Compression of the internal jugular vein by the transverse process of the atlas as the cause of cerebellar hemorrhage after supratentorial craniotomy. Surg Neurol. 1999 May;51(5):500-5. doi: 10.1016/s0090-3019(97)00476-x. PMID: 10321879.
- Jayaraman MV, Boxerman JL, Davis LM, Haas RA, Rogg JM. Incidence of extrinsic compression of the internal jugular vein in unselected patients undergoing CT angiography. AJNR Am J Neuroradiol. 2012 Aug;33(7):1247-50. doi: 10.3174/ajnr.A2953. Epub 2012 Feb 9. PMID: 22322614; PMCID: PMC7965500.
- Ding JY, Zhou D, Pan LQ, Ya JY, Liu C, Yan F, Fan CQ, Ding YC, Ji XM, Meng R. Cervical spondylotic internal jugular venous compression syndrome. CNS Neurosci Ther. 2020 Jan;26(1):47-54. doi: 10.1111/cns.13148. Epub 2019 May 22. PMID: 31119898; PMCID: PMC6930831.
- Higgins N, Trivedi R, Greenwood R, Pickard J. Brain slump caused by jugular venous stenoses treated by stenting: a hypothesis to link spontaneous intracranial hypotension with idiopathic intracranial hypertension. J Neurol Surg Rep. 2015 Jul;76(1):e188–e193. doi: 10.1055/s-0035-15550
- Higgins JN et al. Headache, cerebrospinal fluid leaks, and pseudomeningoceles after resection of vestibular schwannomas: efficacy of venous sinus stenting suggests cranial venous outflow compromise as a unifying pathophysiological mechanism. J Neurol Surg B. DOI: 10.1055/s-0039-1677706
- Goel A. Goel’s classification of atlantoaxial “facetal” dislocation. J Craniovertebr Junction Spine. 2014;5(1):3–8. doi:10.4103/0974-8237.135206
- Rousseff R, Tzvetanov P, Valkov I. Utility (or futility?) of electrodiagnosis in thoracic outlet syndrome. Electromyogr Clin Neurophysiol. 2005 Apr-May;45(3):131-3. PMID: 15981682.
- Müller HR (1985) Quantitative Bestimmung des Blutflusses in der Vena jugularis interna mittels Ultraschall. Ultraschall 6:51–54
- Brunhölzl C, Müller HR. [Doppler sonography measurement of jugular vein blood flow]. 1990;19(1):26-9.
- Özen Ö, Ünal Ö, Avcu S. Flow volumes of internal jugular veins are significantly reduced in patients with cerebral venous sinus thrombosis. Curr Neurovasc Res. 2014 Feb;11(1):75-82. ncbi.nlm.nih.gov/pubmed/24321024
- Rose KM, Wong TY, Carson AP, Couper DJ, Klein R, Sharrett AR. Migraine and retinal microvascular abnormalities: the Atherosclerosis Risk in Communities Study. Neurology. 2007 May 15;68(20):1694-700. doi: 10.1212/01.wnl.0000261916.42871.05. PMID: 17502551.
- Larsen K. Occult intracranial hypertension as a sequela of biomechanical internal jugular vein stenosis: A case report. Anaesth Pain & Intensive Care 2018;22(2):238-242
- Zhao X, Cavallo C, Hlubek RJ, Mooney MA, Belykh E, Gandhi S, Moreira LB, Lei T, Albuquerque FC, Preul MC, Nakaji P. Styloidogenic Jugular Venous Compression Syndrome: Clinical Features and Case Series. Oper Neurosurg (Hagerstown). 2019 Dec 1;17(6):554-561. doi: 10.1093/ons/opz012. PMID: 31329946.
- Dashti SR, Nakaji P, Hu YC, Frei DF, Abla AA, Yao T, Fiorella D. Styloidogenic jugular venous compression syndrome: diagnosis and treatment: case report. Neurosurgery. 2012 Mar;70(3):E795-9. doi: 10.1227/NEU.0b013e3182333859. PMID: 21866063.
I found your article and your hypotheses very helpful. My vascular surgeon diagnosed me with bilateral TOS, but some of my doctors disagree because my symptoms change (I think physical therapy has helped a lot).
I have a neurologist, a cardiologist, an endocrinologist, a physiatrist, a neuromuscular psychologist all on my POTS/dysautonomia team, but no one knows what is causing my symptoms.
My chronic “coat hanger pain” gets much worse sitting up and, of course, standing. I have muscular (typewriter) tinnitus especially laying down, mostly on my right side (not my painful side). Stress was definitely a factor… , pain-bracing-pain is a vicious cycle, so I lay down.
What type of doctor would/should be able to help with the ideas you have proposed? I seem to hit a wall in every direction.
Your articles are extremely helpful.
Thank you.
For my ideas you see me, obviously. Now with regards to symptoms changing, this is very common in TOS.
As for referrals in your country, I can’t help you.
Thanks a lot, I am suffering from 4 years and I now hope to get a better life💙
This is fascinating.
In your opinion, could this apply to other types of dysautonomia that exhibit many of the same symptoms as POTS except the tachycardia, or is it just POTS-specific? Or perhaps for NMH (neurally mediated hypotension) that includes a dramatic drop in blood pressure where POTS does not?
Yes, I think it plays a role in various of similar nature
I have had pots for 14 years and I always wondered why I got worse lying down after around 30 mins later at night when going to bed. I always found if I sat upright for too long (until I was close to passing out and then laid down I would go into a seizure for 20 mins.around 30 mins after lying down, but I’d guzzle a litre of salty water before lying down to try & avoid the seizure but maybe this was actually making me worse? I’d get bradycardic episodes and difficulty breathing lying down which I wonder if was due to the high ICP (I had so much pressure in my face and head it was extremely uncomfortable). I was originally put on Atenolol but felt worse on this during the day (which now makes sense why). I’m just wondering about how the Propanolol helps as I thought the reduced cardiac output lying down (due to compensatory mechanism to lower ICP) contributes to why we feel so unwell lying down too (I get so weak I can barely roll over in bed, weak pulse, used to get bradycardic pauses too and difficulty swallowing/slurred speech, hard to get a breath etc.). Wouldn’t the Propanolol lower output further & make this worse again? The one medication that helps me come out of these episodes is Polaramine which is an antihistamine and anti-cholinergic. Would you know why this would help? If I don’t take it I can lie there for hours feeling unwell but I improve within 30 mins of taking it and I usually feel the need to pass urine which is a sign I am coming out of the episode and perfusing my kidneys I guess. I have wondered too with the adrenal complications whether the drop in cortisol around 11pm/12pm is another cause why I tend to feel really unwell?? I have definitely had stroke like symptoms while lying down, severe one-sided arm weakness, slurred speech, hemi-plegic migraines. Thankfully the severer symptoms are getting better over the years with mast cell stabilisers and low dose Naltrexone (I think I may have Sgogrens as a possible immune trigger or mast cell activation). I guess this may be more a trigger than the root cause?? I have elongated styloid processes and wondering if this could be a contributing factor? Most of my issues are on the left side-left occipital pain and I get tingling in left side of neck but have a few bulging cervical discs too. I woke at 3am last night with chest pain on left side and numb arm which improved once I got up and moved around, so it got me thinking about thoracic outlet syndrome again as a possible root cause and then I found your article. I am from Australia and know a doctor in Queensland who has discovered a lot of pots patients have thoracic outlet syndrome and/or popliteal artery compression. It is all very interesting and your article made a lot of sense and has finally explained the symptoms I had lying down at the end of the day. Earlier on in the day I would usually improve lying down, but after prolonged standing or sitting I got worse lying down. Thanks for your help and explanations, Lisa
I am in Australia too, Qld, and keep getting recommended to look at this research by Kjetil by my GP… fascinating isn’t it? How are you going with everything? I’m going around in circles as so many growing symptoms and diagnoses. Is it the TOS causing the dysautonomia and the ME/CFS and the Fibro… or is it the type 1 diabetes and heart conditions causing the POTS and miagraines and sensitivities to other things… or mast cell reactions or whip lash injuries or past surgery trauma.. or or ?? I’m also finding LDN and anti-histamines’ are helping a little bit with the brain-fog, I can now remember some notes I’ve taken the day before… but still sleeping so much and needing rests so often and even tried to go into the wrong apartment in my building yesterday as just not focused or with it some of the time. I’d love to exercise, but even on betablockers I still go from 60 sitting to 130ish standing and so light headed…crash for 2 weeks if i try and walk more than 200m.. not doing the stops anymore as lose my balance even after a few steps… I crave salt and electrolytes and water all the time.. Have you had any success with improving your TOS or POTS symptoms? I’m still trying to find the article with recommendations for exercise/ stretches for TOS as I’ve been advised my body would not cope well with more surgery… but who knows… maybe it could help?
This has absolutely blown my mind. I was given a diagnosis of idiopathic intracranial hypertension in 2019 and was immediately put onto diamox. I had two lumbar punctures to check CSF levels. The first went amazing but the second I had immense pain shooting down my right side followed by nausea and extreme headache. Fast forward to Nov 2021 and 48 hours after my second Moderna vaccination I was awoken in the night with what felt as if it was a heart attack, multiple hospital and doctors visit is later I have now been diagnosed with POTS and they have found a Left bundle branch block. I have a strange feeling that the diamox is causing more harm then good. I’m now taking diamox, atenolol and fludrocortisone. What you said about diamox really shocked me. Thankyou for this great information.
Would get off the cortisone and diamox right away.
This article came to me via someone who responded to a comment I left on YouTube regarding tinnitus. I’m so glad I read this.
My issue started after jerking my head while dancing at the beginning of pandemic to relieve stress. X-rays showed an old whiplash injury from decades ago. C4/5 are slightly out and curvature looking sideways should look like a C but instead looks like the left side of a Y. There is constant tightness in the neck and shoulders no matter how relaxed I am.
Six months of once a week Atlas adjustments have helped other issues but not the noise. B1 complex, magnesium, Bioflavanoids, L-theanine, ginko all had little effect. Sugar, carbs alcohol and salt intake makes it worse because of inflammation so those were reduced/eliminated. I found fasting, doing paleo/keto, meditation, yoga, hot epsom salt baths are the only things that reduce the noise.
A lot of what you mentioned about neck injury makes sense as when I move my neck with my ears to the shoulders the noise gets louder. I’m also doing trigger point therapy on my body using a massage gun and balls and use a neck shelf/pillow to lay on for a few minutes a day. Changing pillows also has not made any difference. But I also understand that T is ringing in the brain, not the ears.
Is there an exercise other than the McKenzie method, neck stretching, tapping, flicking the back of the head with fingers to reset the brain or going through the process of TRT? Thank you.
I was reading your article here on POTS, and some of your key words jumped out at me, because I’ve been using them in describing my hyperadrenergic POTS to my doctors. I’ve been telling them that I seem to just vasodilate for no reason. Also, regarding my “coat hanger” area, I’ve told doctors I feel like I’m bracing all the time. I have a low mental stress life, as I mostly stay home, but apparently my POTS causes a high physical stress on my body from walking around. I mainly sit in a semi-reclined(rounding my whole body somewhat) because if I sit straight up, I eventually feel like passing out. After reading this article, I feel like that position may be “opening up” vessels in the neck are so they can drain maybe? One last thing that clicked after reading this–I normally have slept with my head/neck elevated at night, and now I know why. But, a few months ago I decided to work on strengthening my upper back/neck to improve my posture(my poorly thought out design). I was lying flat in bed and squeezed my shoulders together and pulled them down. On about the third squeeze, the room started spinning. It scared me, but I’m now guessing it had something to do with the high pressure from lying flat and it was aggravated. LIke I said, your article pulled a lot of stuff together that I’ve seen in my own case. Anyway, after reading this whole article, is there something you can help with all this? I only saw you spoke of surgery, so wasn’t sure if YOU had a plan that can help all this. Thanks for your great article, as I always thought my POTS was a mechanical issue, but couldn’t put my finger on it.
Hi Karen,
I experience improvement in my chronic stress activation from POTS when I round my body like you describe. I think when we go into good posture, because our musculature in the thoracic outlet and neck region are so weak, they become very tight under the increased weight bearing on them in the improved posture and when we induce a rounding of our body it enables these muscles to relax more, thus allowing the veins to have better patency. Reply to this comment if you want to chat further about all this, I sincerely hope you’ve been able to get some improvement!
This is correct, flexing in reduces the tension in the scalenes and pectoralis minor muscles which in turn reduce arterial head pressure. It is an acceptable short-term trick to reduce symptoms during bad spikes, but treatment of the underlying problem should be done for long term benefits.
Could this be POTS? I have TOS due to 2 bilateral cervical ribs.
These are my symptoms
I would love your option as my Dr is at a bit of a loss as to what to do for me.
I get episodes of excessive burping and when this happens I feel off, brain fog, off balance like I’m going to tip over or like I’m walking on a boat type of feeling. Legs are heavy, I feel like there is air in my rib cage on my left hand side near my heart. Shortness of breath while the burping is happening and find it exhausting to talk when I feel like this. I have bursitis in my right hip and this leg gives way on me occasionally when really bad but it’s like an annoying ache most of the time in my groin that I feel I want to stretch out all the time. When I do stretches it does feel better and I hear my insides gurgling. I feel my hip pain and digestive issues are connected and when I eat my stomach sometimes feels heavy and then feels like it is pulling on my lower back and that gets sore. I have a very weak core and stability/balance is shot! Bit of history i have had 3 csections the first was an emergency csection, first csection scar also got infected. I had human hormone injection when I was around 4 years old but my parents didn’t want to continue with the rest of the treatment. Not sure if any of these incidents could of triggered anything? I am very sensitive to strong smells/chemicals and used to work in a photography lab developing film etc so not sure if this could of started things? I can’t wear makeup/moisturizer/sunscreen on my face as it makes me sleepy or perfume as it gives me a headache and brain fog. I don’t get any rashes but I am allergic to lupin and I do get a rash if I have consumed it. I get extreme anxiety while I’m having these burping episodes and this has all been more noticeable having my third son 2 years ago and I also had a tubial ligation at the time of the csection. I could almost feel a chemical release happening in my system not long after having him and breastfeeding at the time, which was a weird sensation. I’m also wondering if getting my tubes tied could be the cause of my hip pain/tight ligaments/muscles. My bum sticks out and I have a dished lower back, which I believe is caused by tight hip flexors. I also have a bit of scoliosis so my posture could be the cause of my digestive issues too and balance issues? Or even scar tissue from the csections as sometimes it hurts along that area with trapped wind or if a stool is moving along that area. I do feel a bit better after I have had a pooh I feel like the tension on my groin area is released a little. I feel the need to urinate more often too as this also releases the tension in my groin.
I have also had some people mention histamine intolerance to me. There is probably a bit of cross over of symptoms going on maybe. But would love to hear your thoughts and advise.
I’m currently eating gluten free and dairy free on the advise of my nurse practitioner, I have tried low FODMAP diet. She is trying me on different probiotics at the moment to try and get my gut microbiome balanced. She has put me on progesterone as my estrogen levels were high. I had an iron infusion as my ferretin level was 12. Iron is back to normal levels now but still feel tired. My periods were heavy but only on day 2 like i was getting it all on one day and then pittered down to nothing much at all for the rest of the cycle, on medication for this now when I have my period.
I’m 44 years old any ideas? Thanks for listening it was a bit of a long one!
Oh one other thing I feel a bit shaky if I don’t eat on time like my blood sugar level drops, but not all the time and feel very anxious at this point too. I feel tight in my neck and shoulders all the time and my neck clicks when I put my ear to my neck or turn my head to the left like it’s clicking over a knot. I see a chiro fortnightly but my neck side ant seem to feel any better?
Apologies, this is too long for me to read outside of consultation.
Hi, thanks for sharing your theories here! Have you heard of amlodipine being used as a treatment option for this?
Completely useless drug for POTS management.
I have EDS and had a dural puncture during a cervical steroidal injection in 2008, with spinal fluid leakage, migraines, and postural headaches, then 2 small strokes (I also have heterozygous factor V.) I have usually low-normal BP (100-110/60-70), have orthostatic hypotension, bilateral tinnitus, cervicogenic migraines, fatigue (with two periods of 2-3 months with severe fatigue and brain fog), and was just diagnosed with moderate-advanced arterial TOS (arterial and venous on the right side.) I’m on a number of meds for pain, GERD, and insomnia, and am on Vyvanse for my AD/HD, which is of course a stimulant and vasodilator- is that contraindicated? I’m seeing a Vascular surgeon in a few weeks for the TOS- anything you’d recommend telling her? Thanks!!
If you were my patient, with this history, I would never recommend nor permit the usage of this drug. But you have to discuss this with your doctor who knows your case properly.
What a surprise to come across your article. I guess I stopped looking. Big mistake.
I had four TOS surgeries at UCLA, the last in 2001. I was diagnosed via physical exam, some special MRI, and an EMG nerve block. My TOS symptoms were vascular to my hands and also to my head. I remember my fingers were freezing cold, with purple nail beds almost all the time.
I got diagnosed with TOS incidentally. I had a bad headache after a severe viral encephalitis, so had been referred to the headache specialist. After her physical exam, she got me to the diagnostic neurologist, the radiologist who had come up with the new (at the time) protocol to evaluate vascular integrity/ impingement (I think), and the fantastic vascular surgeon.
Hands are still pink and warm 20 yrs later.
You do a service to answer the posts that you do. Many thanks.
I’m in the midst of a sure diagnosis. Older dx include fibro, chronic fatigue, recurrent major depression, anxiety, social phobia, and small fiber neuropathy diagnosed by skin punch bxs x 4. I’m pretty miserable and worried about suggested treatments, especially since I feel so crappy already and I can only imagine how adding another rx to the mix is going to make me feel. I found your Very Interesting Research Publication by googling “does POTS affect vertebral arteries” because of some recent brain MRI findings telling me it must!! Wish you were in practice in the US, Florida! I would certainly trust you with my care!! Know anyone who thinks like you in my state?
I was wondering if there could be a connection with POTS and Eagle Syndrome. I was diagnosed with Eagle Syndrome on my left side last year and POTS two year before that. Seeing that the styloid process is near the jugular vein and the vagus nerve and reading your text about CVH it almost seems logical.
I don’t think Eagle is a major player in this disorder. But the venous congestion won’t help…
Is there a relation to mitral valve regurgitation & diastolic dysfunction/failure with this theory? I have both issues along with the ME/POTS diagnoses and it struck my amateur understanding that the mitral valve regurgitation could be a coping mechanism to reduce cranial pressure(while also freezing my feet as a side effect.)
Likewise my dramatic worsening after eating & ever lowering HR tolerance before unconsciousness/severe cognitive impairment could be the conflicting needs of the brain for less cardiac output & the digestive system for more.
I don’t know. It’s possible, as CVH will reduce cardiac output. I guess that in some specific circumstances, especially if the patient has other predisposing factors for cardiopathy (eg. preexisting hypertension, hypervolemia), that it could double up and cause valvular failure. But as I said, I am not sure.
Hi Larsen!
Can conservative treatment of Thoracic Outlet Syndrome improve POTS, along with elevating the head at bedtime, without medication?
I am very intolerant to medications, propranolol left me with insomnia for three days in the three days I took it!
Every symptom that is mentioned here, I have been having for years and I have been to every specialty MD possible. I have severe neck pain with disk compression c3 through T1. I’ve been diagnosed with Fibromyalgia or Small fiber neuropathy, chronic fatigue, gastric paresis etc. I have severe TMJ, Tinnitus, Vertigo and suffer from POTs type symptoms including increased cranial pressure upon exertion. I have temp dysregularity and sudden adrenaline rushes thatvwake me up at night. I suspect some sort of autonomic dysregulation. I have yet found a proper diagnosis and I feel the pain in my neck is directly related to all the other symptoms due to the fact that as the pain increases, so do all the other symptoms. I wish I could find a Dr here in the states near Atlanta GA that knew about this subject and would listen to me. I feel like this article perfectly describes everything I’ve been experiencing and no one will listen.
Hello, when the article says sleeping with your head flexed, does it mean sleeping with your chin tucked in or your head raised upwards?
No. It just means forward.
Hi Larsen!
Can conservative treatment of Thoracic Outlet Syndrome improve POTS, along with elevating the head at bedtime, without medication?
I am very intolerant to medications, propranolol left me with insomnia for three days in the three days I took it!
30 Years ago I was diagnosed with postural dysautonomia ( congenital) after a sudden non provoked incident of severe vertigo upon waking up. They did a tilt test. Their RX take Na Cl. daily worked fie w/ot recurrence till 8 years ago when I had minor soft tissue trauma C6/7 at back of neck which elicited chronic low grade migraines and mild balance issues. Botox since failed. Due to debilitating migraines I opted for”occipital nerve decompression surgery. Surgery worsened migraines/equilibrium.New brain fog, moderate insomnia, intermittent hot flashes, tiredness, nocturia, and severe overall tiredness. Post surgery C spine flex/extension x rays, and MRI which show no areas of narrowing or instability. My quality of life has severely impaired. Do you believe the surgery was indicate in absence of any physical encroachment to the neural canal/ foramina/ vasculature? The surgery brought above mentioned symptoms. Was this surgery indicated? What can be done to regain quality of life ?
Hi, how are you?
At a glance I don’t think this was ever an occipital nerve problem, no.