This article will explain in depth how to measure and correct the atlas joints, both at the much neglected atlanto-occipital junction, and the more popular atlantoaxial junction. It will reveal what I consider to be the main exacerbating factor behind atlas misalignment, why I believe that many approaches are missing crucial aspects and measurements of atlantal alignment, as well as essential factors that prevent correctives from sticking.
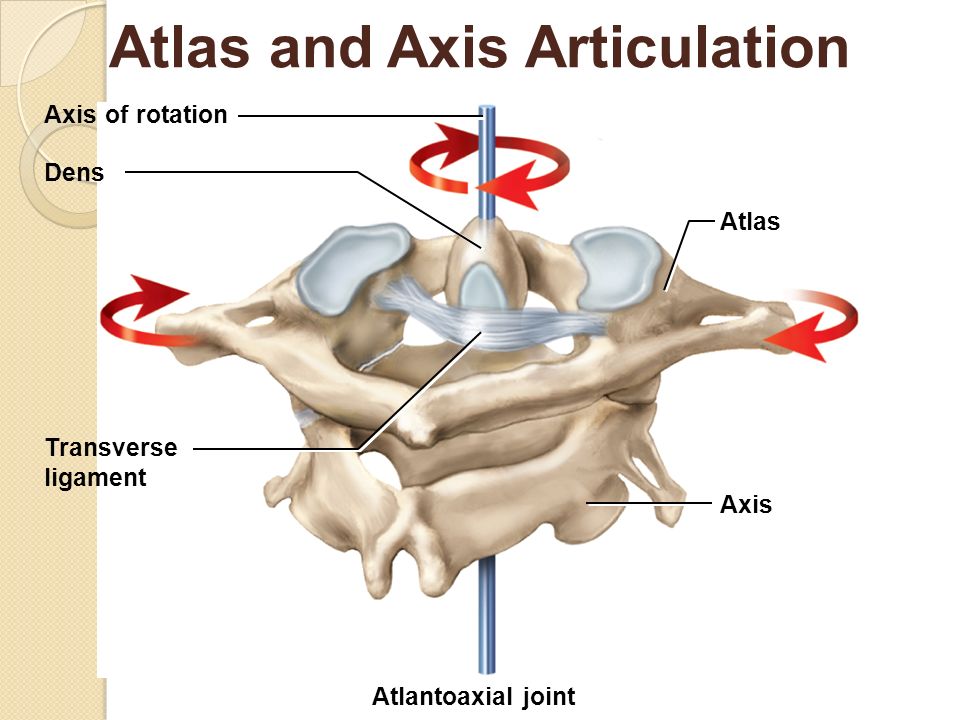
The atlas is the first and top cervical vertebrae (C1), holding the head (occiput) and thus forms the atlanto-occipital joint (A-O). The second cervical vertebrae, is the axis, or C2. The atlas (C1) pivots on the axis of the dens, making it a unique type of joint compared to the other vertebral joints. It’s called the atlantoaxial joint or A-A (C1-C2).
Thick ligaments hold these joints in place, but patients with atlas misalignment often have ligament laxity after e.g whiplash injuries and/or years of improper cervical posture and movement patterns. Most of the time, despite some level of ligamentous laxity, great and lasting results can be achieved by re-establishing proper postural and cervical movement habits, as well as significantly strengthening the muscles that stabilize and syncronize the movements of the atlas joints. The key lies in changing the patient’s habits.
Fig. 1
What do I mean by that? What does our habits have to do with atlas misalignment?
Certain factors either ‘make you or break you’. For instance, certain muscles stabilize and syncronize the atlas joints’ movements and position, as I mentioned above. These muscles are greatly reliant on proper cervical posture and movement patterns to function properly. If these structural dependencies are compromised, the muscles will be as well. A downward spiral with loss of tensegrity (i.e loss of muscle tension and stability), muscle dysfunction and imbalances, compensatory patterns, tightness and pain tend to develop.
Once the muscles do not move nor hold the spine in proper position any more, excessive motion tends to develop between the A-A or A-O joints, over time leading to atlas joint hypermobility and misalignment. This is why normalizing and even optimizing craniocervical habits, as well as other factors, are key to resolve atlas misalignment in my experience.
Let’s move on and have a look at the most important anatomical aspects of the atlas joints.
This article is written for educational purposes only. It does NOT promote self-treatment for patients. Playing around with the craniocervical junction is NOT risk free!
Anatomy of the atlas joints
As mentioned already, the atlas joints are made up of the A-A and A-O joints. The atlantoaxial (A-A) joint is a special cervical level, as it yields more rotation than the other cervical vertebrae. According to some medial literature, it makes up 50% of total cervical rotation. It is however relatively limited with regards to flexion and extension (10 degrees) and side flexion (5 degrees – Magee, D. Orthopedic Physical Assessment)
The movement within the atlanto-occipital (A-O) joint, is the opposite. It yields about 30 degrees of total flexion-extension in the sagittal plane, but only about 15 degrees of lateral flexion and 5 degrees of rotation. Thus these two joints complete each other by providing more of the movements that its counterpart does not. The remaining movements come from the lower cervical spinal segments. Because the atlas bone holds the cranium, it craves stability. Compromisation of the A-O joint is common is long-standing neck injured patients, but lacking measurement criteria causes it to be neglected in most cases. Thus vital information on craniocervical alignment will remain hidden.
Fig. 2
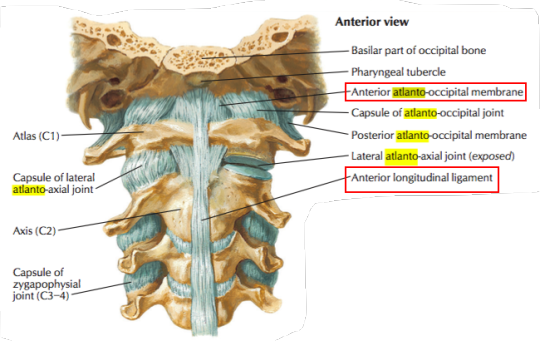
The outer layer of ligaments, roughly stabilizing and restricting excessive movements between the A-O and A-A joints, are the posterior and anterior atlanto-occipital and atlanoaxial ligaments. Connecting the atlas joints (articulate surfaces), we have the A-A and A-O capsular ligaments. These restrict greater joint movements in all vectors, making up the rougher atlas joint stability foundation. Running from the occiput and down to the C7 is a thick ligament called the nuchal ligament. It is the cervical version of the supraspinous ligament. Because the spinous processes between C2-7 are relatively short, the muscles of the neck that would normally attach to the spinous process, such as the trapezius muscle, instead attaches to the nuchal ligament.
Laxity of the above mentioned ligaments would cause inappropriate increase in A-A and A-O joint articulation, such as increased rotation, side flexion etc. This could cause the occiput to improperly glide forward, backward or to the side on the atlas bone. Additionally, it may predispose the axial (odontoid peg’s attachments) ligaments to injury, due to the abnormal movement ranges or joint positioning.
Between the axis (C2) and the C3 vertebrae and further down the spine, runs the flaval ligament. In similar fashion it will restrict movement between the axis and C3, C3/C4 and so on. The first spinal disc is located between the axis and C3 vertebrae, and this is also where the zygapophysial (45° facet joints) first appear.
Fig. 3
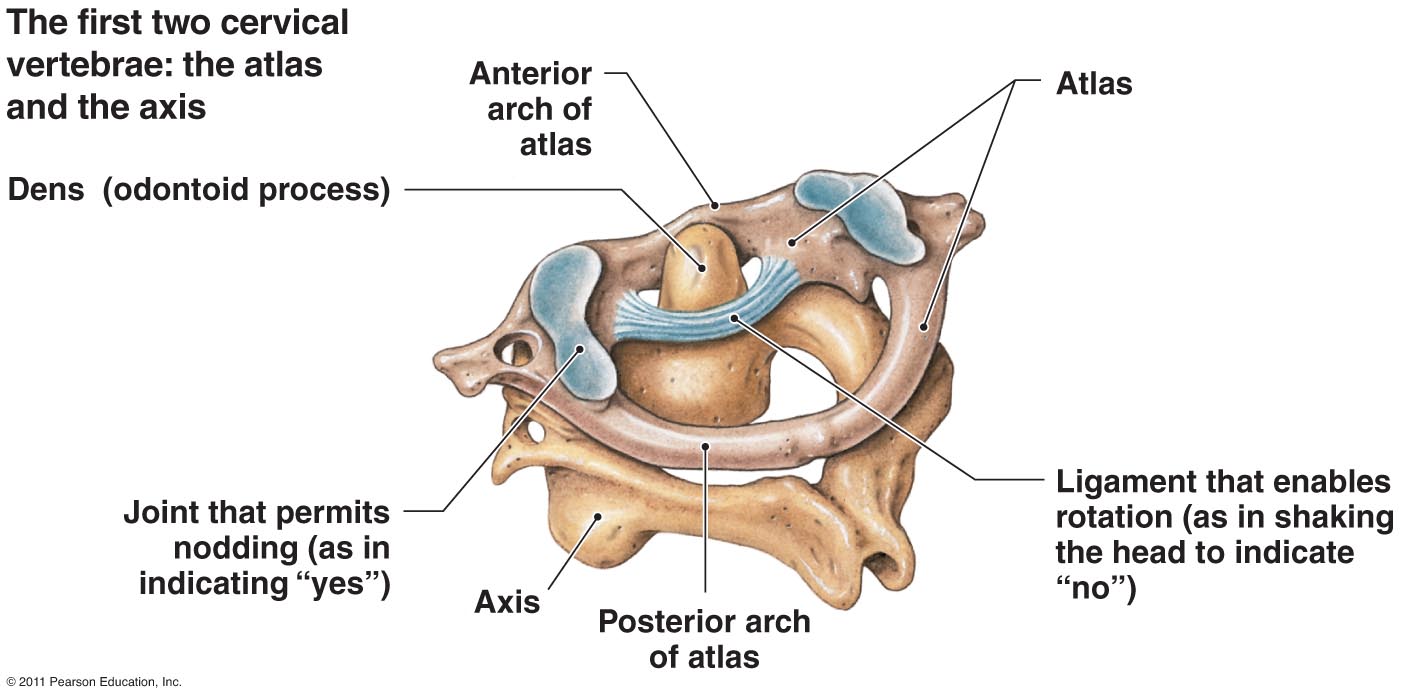
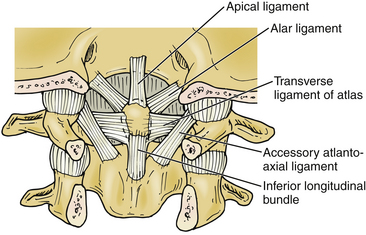
The integrity of rotational symmetry and positioning between the A-A and A-O joints is maintained by ligaments that ensure a proper axis of rotation within the region. Some of the most relevant ones, are the apical ligament (anterior to the longitudinal part of the cruciate ligament), alar ligament and transverse (cruciate) ligament that connect the odontoid process to the C1 and occiput, and also maintain axis of rotation (see fig. 2). Behind these, are the tectorial (proximal part of posterior longitudinal) ligament.
The odontoid process, C1 and occiput are tightly held in position of optimal axial rotation by the above-mentioned ligaments. If they get stretched, the axis (spine) and occiput will no longer move in proper symmetry, as the external ligaments do not uphold axis of rotation in the same manner. This may thus result in improper gliding and rotation between the A-A and A-O joints, leading to many potential problems which will be addressed later on in this article. Considerable injuries to these ligaments will usually require surgery. This article is primarily focused on treating chronic injury and not acute injury.
Fig. 4
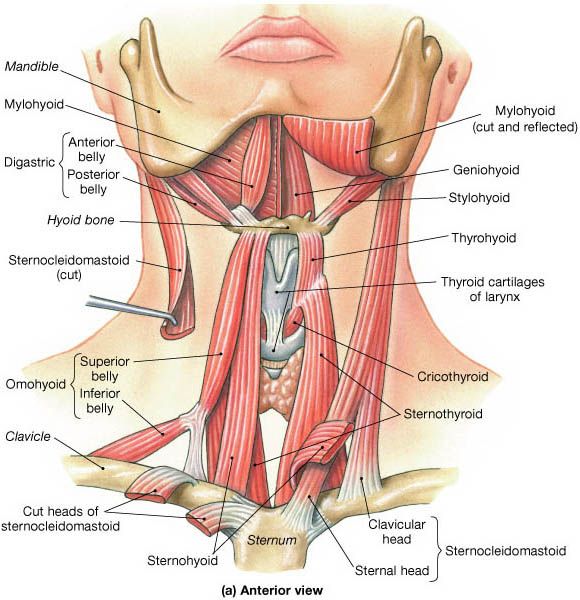
Muscular anatomy
Thankfully, the ligaments are not left to handle all the strain by themselves. Several muscles stabilize the atlas joints, both proximally (shorter muscles) and regionally (longer muscles). When these muscles activate properly, movement of the head and neck will pull the A-A and A-O joints symmetrically, so that the ligaments do not overburden due to improper vertebral movements. There are many muscles in the neck, but I’ll elaborate on those whose functions are more often compromised and causing imbalances.
Tightness of certain structures may also restrict optimal axial rotation of the cervical spine, and is also an important potentially exacerbating factor for misalignment and hypermobility. Let us have a closer look at the muscles that insert into the atlas, its functions and connections.
The suboccipitals
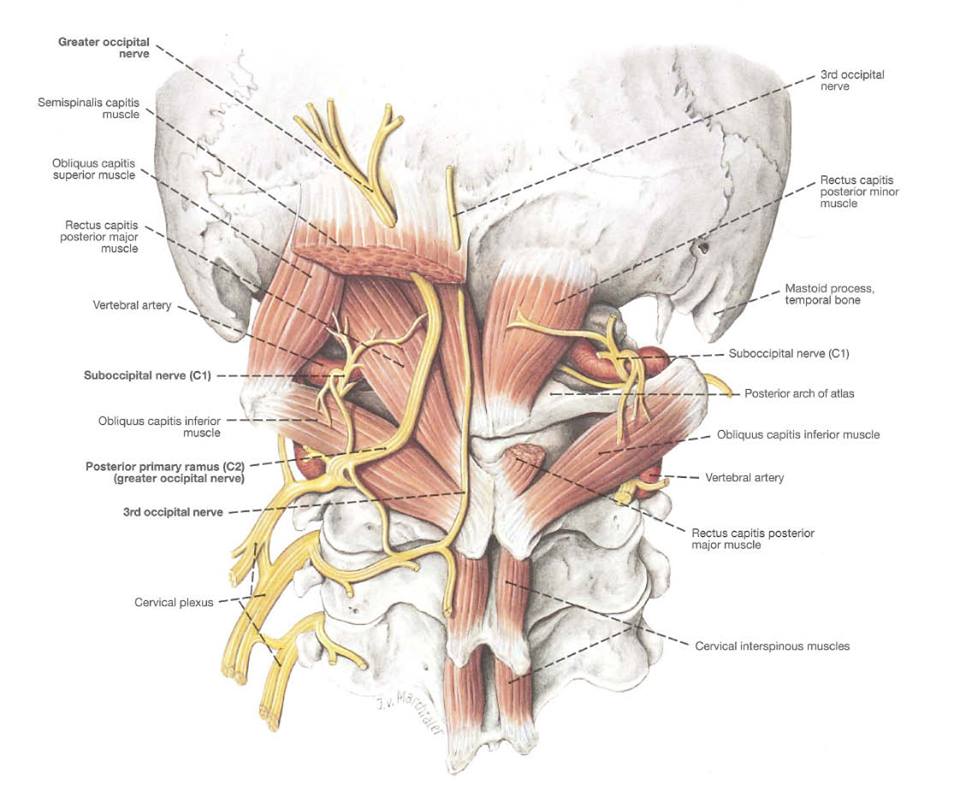
The suboccipital muscle group mainly attach between the atlas, axis and occiput, and are thus greatly involved in atlanto-occipital as well as atlantoaxial stabilization, both with regards to posture and craniocervical movement. The posterior suboccipital triangle consist of four main muscles, one set on both sides.
- Rectus capitis posterior minor & major (RCP min/maj)
- Obliquus capitis superior & inferior (OCS / OCI)
All of these muscles, except the OCI contribute to occipital extension and prevent posterior glide of the occiput on the atlas joint. Additionally the RCP major will cause ipsilateral rotation of the occiput, and OCS contralateral rotation of the occiput. It’s useful to understand these pulling vectors in order to know which muscles are imbalanced when the atlas joints are not positioned or moving symmetrically, but not paramount. Generally they all require significant strengthening in the typical atlas patient. The seemingly contradictory muscle fiber orientation of the muscles within the suboccipital triangles will ensure that the atlas joints move symmetrically together with the occiput. Their coactivation will thus also contribute to joint centration.
Fig. 5
The suboccipital muscles will also level the head in the sagittal and coronal planes, ensuring levelled eye sight. These muscles are in fact intrinsically connected to the eyes to such a degree, that if you palpate them while moving the eyes, you’ll feel the suboccipitals respond directly to your eyes’ movement. Research has shown that the suboccipitals have a tremendously high spindle cell density. The spindle cells are (amongst other things) responsible for proprioception, which simplified means control and awareness of the respective limbs. Not a surprise, as these muscles hold the head itself.
The distribution and arrangement of spindles within the muscle and their arrangement was studied. The spindle density of superior oblique muscle was found to be 190, that of inferior oblique was 242 and the rectus capitis posterior contained 98 spindles per gram of muscle. – Kulkarni et al., 2001
Muscle spindle density is extremely high in the deep muscles of the human neck. – Liu et al., 2003
Scientists have found that the cervical muscles muscles and especially suboccipitals, are often atrophied in patients with whiplash, neck pain and vertigo (Kristjansson 2004, Andary et al. 1998, McPartland et al. 1997, Elliott et al. 2015). It has also been shown that saline and procaine injections into the suboccipitals significantly relieved symptoms of vertigo, disequilibrium (lack of balance), and pain levels (Campbell, 1944; Hinoki, 1972; Gimse, 1996).
Based on the above, it’s clear that the suboccipitals have tremendously important functions in the body. Stabilizing and symmetrically pulling the A-A and A-O joints, intrinsic relations to our vision, balance and posture. It therefore makes me cringe when I see therapists and patients release (needle, massage, stretch) the suboccipitals; I consider it iatrogenic treatment. These muscles are unique and should be handled with the utmost care. Rarely (never!) is it appropriate to release the muscles; they should be strengthened to ensure proper function.
Asymmetrical A-A or A-O articulation, vertigo, headaches, whiplash, etc are all indicators of potential suboccipital compromisation, and means that they should be assessed. The best way to assess their functions is by strengthening them, or by MMT. The MMT for the suboccipitals are too complex to detail in this article, but if the exercise is heavy then they will often need significant strengthening. Palpative examination is also useful. They are often atrophied and very tight, and squeezing into them may cause great pain, headaches and migraines for the patient. I reiterate; this is NOT an indicator that they need release, but rather means that they are in need of strengthening.
The cruveilhier’s plexus
The cruveilhier’s plexus, also called the posterior cervical plexus, is a bundle of posterior rami nerves stemming from the upper three cervical levels, C1 to C3. Through the suboccipitals and more superficial neck extensors (such as the trapezius and splenius capitis) emerge the suboccipital & occipital nerves. When these muscles are severely inhibited and can not function properly, the nerves may get entrapped within their fibers, leading to occipital neuralgia.
Fig. x
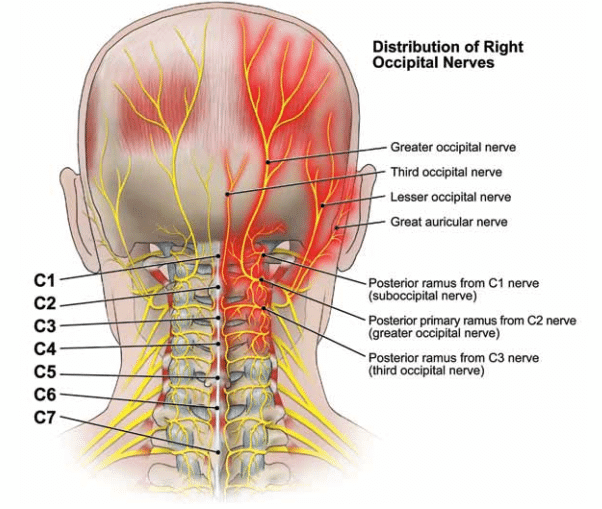
Occipital neuralgia can be devastatingly painful, in similar fashion to trigeminal neuralgia (which you can read more about in my TMD article), and may cause severe neuralgic pain, radiating into the posterior neck and head. It is sometimes described as an electric shock, a sharp and stabbing pain.
The solution to this issue is to exercise the suboccipitals along with the more superficial cervical and occipital extensors. Exercising these muscles may lead to significant exacerbation of the patient’s symptoms initially. This phase may last between 1-6 months. Symptom exacerbation is usually a confirmation that the exercises are done properly, but degree of exacerbation can be controlled by starting ‘slow and easy’, not doing too high intensity training of these muscles until they are capable of doing so. In other words, gradually increasing load and volume as the muscles improve.
Fig. x
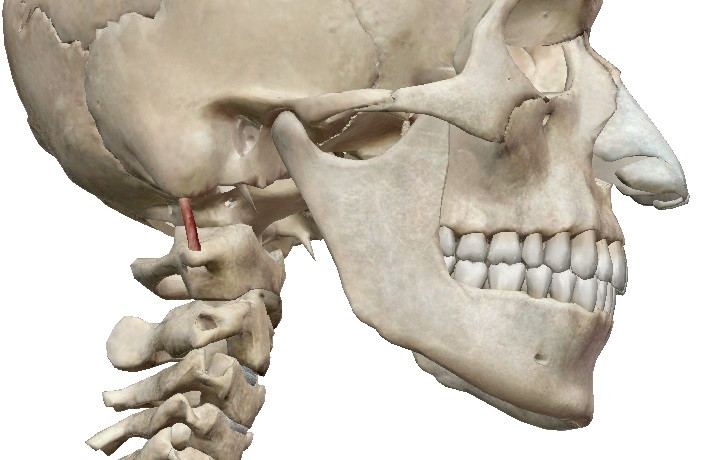
The rectus capitis lateralis
The rectus capitis lateralis muscles control and restrict lateral gliding as well as excessive rotation of the occiput on the C1, and it attaches from the skull’s jugular process to the C1 transverse process. If exercised unilaterally, they may also cause lateral translation of the C1 (or contralateral translation of the occiput), especially if the atlanto-occipital ligaments are lax.
Having strong rectus capitis lateralis muscles is beneficial, because it restricts excessive movements within the A-O joint, however one must be somewhat cautious when working these special muscles, so that no unwarranted translation will occur between the C1 and occiput. Using equal intensity on both sides, and of course measuring the distance between the edge of the C1 transverse process and the lateral edge of the mastoid process both before and after the strengthening, to ensure that no unwanted lateral translation has occurred.
The measurement for lateral translation of the occiput, is measuring the distance between the lateral edge of the C1 transverse process and the lateral edge of the mastoid process. Estimate based on palpation whether or not the distance is greater on one side.
It may sound absurd that these small muscles can shift the whole head’s position on the atlas bone, but I assure you that this is the case if the patient has ligamentous laxity, and you will be able to detect this for yourself with the protocol outlined in this article.
Fig. 6
Rectus capitis lateralis exercise
The scalenes
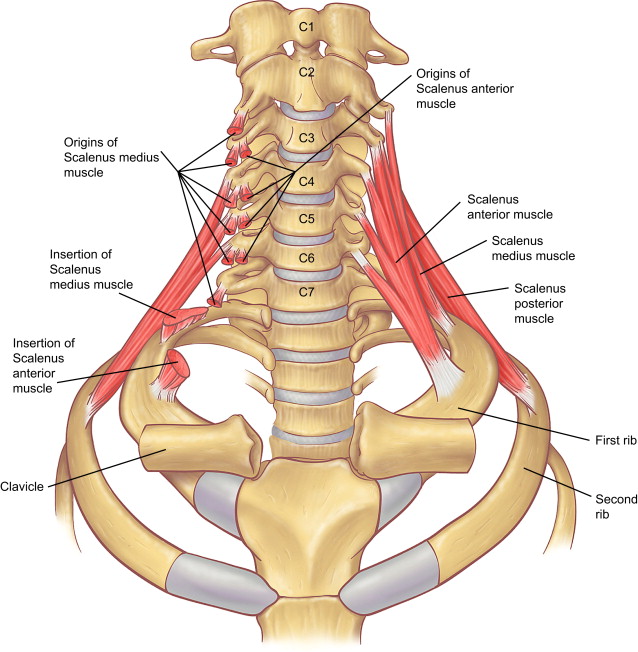
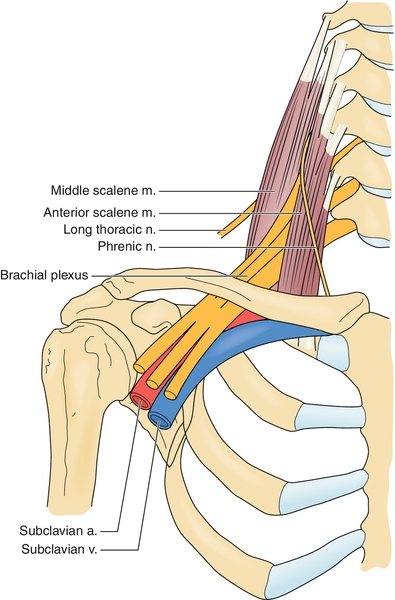
The scalenes are very important muscles as well, because of their relation to the brachial plexus, subclavian artery and subclavian veins. The scalenes are lateral flexors, lateral translators, and ipsilateral rotators of the cervical spine. They also elevate the ribs during inspiration.
There are three portions of the scalene muscle; the anterior, middle and posterior heads. The anterior scalene attaches from the first rib, to the transverse processes of C3-C6. The (largest) middle scalene, between first rib, and (some illustrations show that it also connects to the C1-TVP) C2-C7. And, lastly, the posterior scalene between the second rib and C5-C7.
Fig. 7
The scalenes are often very weak, due to postural abnormalities such as slouching shoulders and forward head posture. In turn, they may greatly restrict the movement of the cervical spine, especially with regards to rotation and extension. When there’s severe restriction in rotation, this may cause excessive movement to occur between the A-A (C1/C2) or axiocervical (C2/C3) joints, ultimately leading to ligament laxity and instability of the upper cervical spine, as I touched upon earlier.
Additionally, their tightness may entrap the nervous and vascular bundles of the thoracic outlet, causing thoracic outlet syndrome. An especially relevant point to note is that the vertebral artery that supplies the brain, is a branch of the subclavian artery. When the scalenes compress this artery, it may compromise the brain’s blood flow, and lead to many different problems such as vertigo, fatigue, migraines, and similar symptoms of vertebrobasilar insufficiency. So far I have yet to see a patient with noteworthy atlas misalignment who didn’t also have TOS, but fairly I have indeed seen many patients with TOS who did not have atlas misalignment.
The scalenes are usually weak, and it’s a huge mistake to release them, in my opinion. Strengthening is the key, but the exercise can cause tremendous pain if done too intensively in patients whose thoracic outlet is compromised within the interscalene triangle. Perform one gentle set per muscle unto mild fatigue, not more. Do this maximimally twice per week. I’ve seen dramatic symptoms occur in relation to these exercises many times. If they’re worked too hard, too fast, inflammation will occur and symptoms may greatly exacerbate. This will, of course, subside, but it’s better to start carefully and then gradually increase over time.
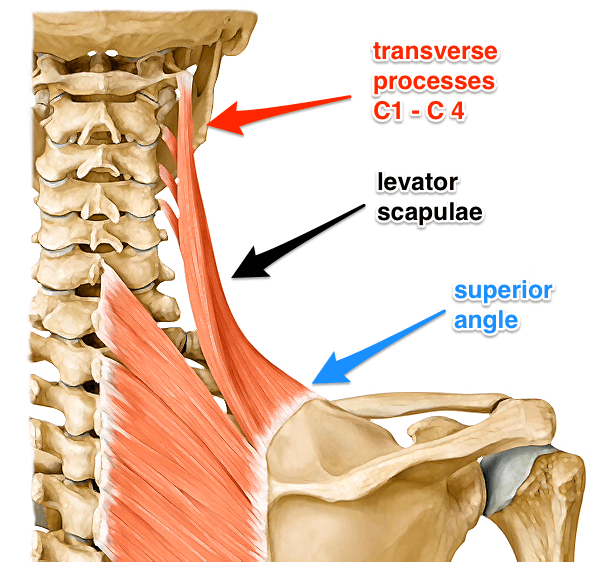
The levator scapulae
The levator scapulae is a contralateral rotator and lateral flexor of the cervical spine. It also elevates the shoulder blades and pull them into downward rotation and anterior tilt. The levator scapulae attaches between the scapulas superior angle and the C1-C4 transverse processes. Co-activation and balanced pull/tension from the levator scapulae will restrict anterior translation of the atlas joint and thus passively influence/restrict posterior gliding of the occiput, which are both commonly seen in these types of patients.
Because of its atlantocervical attachment sites, it has a great influence on atlas joint movement and stability. Tightness of the levator scapulae may restrict rotational range of motion in the cervical spine, often more on one side than the other. In such case it will cause continuous pulling forces to occur on the upper cervical transverse processes, often pulling these into a de-centrated position. Additionally the levator scapulae is a common cause of chronic headache, shoulder pain, and sometimes vertigo due to destabilization of the atlas joints.
Fig. 8
The main cause of levator scapulae dysfunction is faulty posture, and especially faulty resting position of the shoulder blades. I’ve written a detailed explanation about this in my TOS article that’s mentioned earlier, and thus won’t repeat that here. I’ve already written about it in my scapular dyskinesis article.
In short, though, continuous slouching of the shoulder girdles will cause inhibition and severe tightening of the scapular elevators such as the levator scapulae. The only long-lasting way to deal with this is through postural correctives. It is however also beneficial to strengthen the LS and trapezius muscles in a parallel manner, to support the postural re-education and speed up the the muscles’ healing. It is almost always injured and require strengthening in whiplash injury victims.
The levator scapulae may also be used in order to force symmetry upon the atlas joints. I’ll come back to this muscle in later parts of this article.
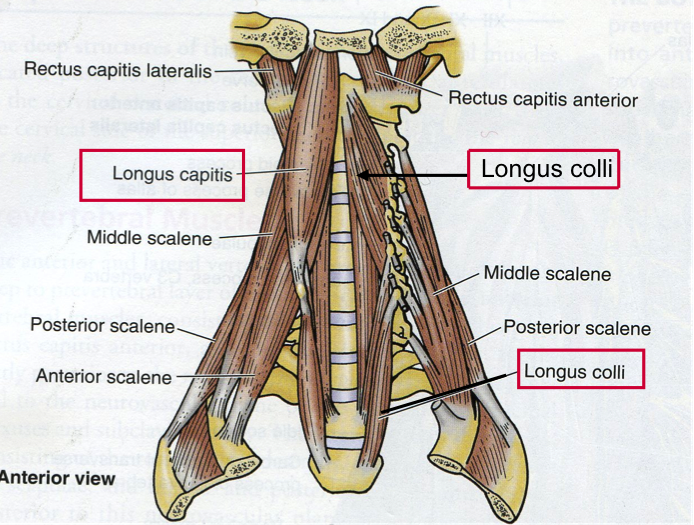
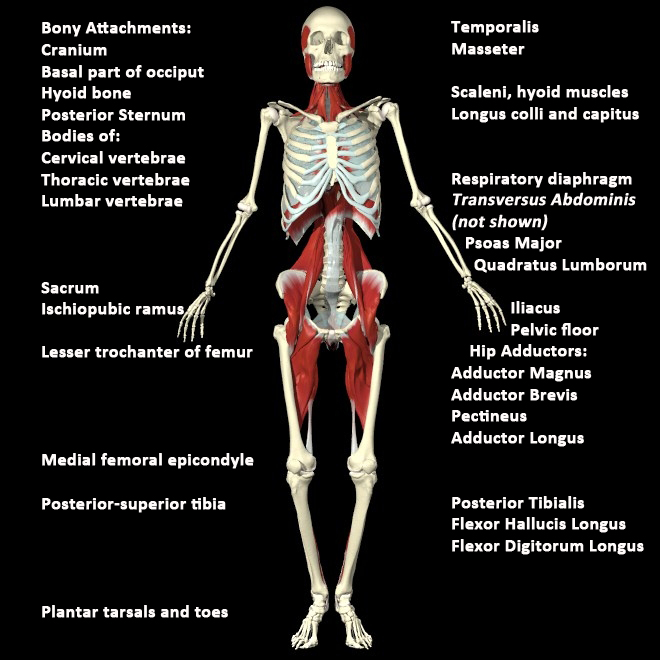
The longus colli and longus capitis
The longus colli and capitis muscles prevent anterior gliding of the atlas in relation to the occiput, as well as preventing hyperextension (“hinging”) on the cervical spine. They are therefore very important structures to be aware of when treating atlas and neck dysfunction. The longus capitis extends from the skull and down to C6, while the longus colli spans from the C1 and to the T3 vertebrae. Because they control cervical hyperextension, habitual (postural) hyperextension and hinging on the cervical spine will cause them to inhibit. Therefore they are usually weak and need to be strengthened significantly.
The alar fascia of the neck ties together the longi muscles and the sympathetic chain, i.e the cervical ganglia, in the anterior cervical column. Dysfunction of these muscles may cause irritation of these sympathetic nerves structures, causing diffuse issues. More about this later.
They longus capitis can be trained seated by pulling the chin down while maintaining a long neck (no hinging), and resisting downward movement of the chin with your hands. The longus colli can be trained supine, by tucking the chin down to the sternum and then flexing the neck. The suprahyoid muscles must be controlled and shouldn’t contract excessively.
Fig. 9
Longus colli
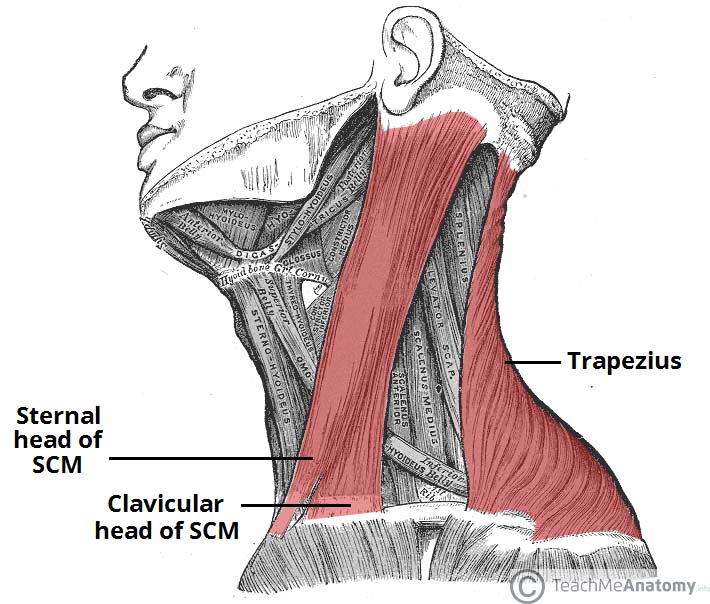
The sternocleidomastoids
The infamous sternocleidomastoid, or SCM in short. Often blamed for virtually any occipito-cervical pathology, ranging from neck pain, headaches, tinnitus, etc – You name it. In reality the SCM is a very important muscle, and very misunderstood. a neck flexor and occipital extensor, attaching from the mastoid process and splitting into two heads that attach into the clavicle and sternum. It also functions as a contralateral occipital rotator, raises the clavicle and sternum during inspiration, and prevents posterior A-O gliding of the occiput.
Contrary to popular belief, the SCM is often weak and requires strengthening, not releasing. Because the SCM is a neck flexor, and when a patient is hanging forward with their heads, this function is inhibited as the head is just hanging forward. It is absolutely NOT pulling the head forwarda nd down, as many mistakenly believe. Muscle test it and see for yourself, by having the patient pull their ear towards their sternum, while you resist at the back of the head. It will be weak!
Fig. 10
Between the SCM and the anterior scalene, lies the phrenic and vagus nerves. These autonomic nerves control an array of functions in the body, such as hiccups, coughing, heart rates, etc. The vagus nerve is also referred to as “the wandering nerve” because it is unique in innervating almost all of the organs in the abdomen, controlling many autonomic tasks. In addition to these nerves, the carotid sheath containing the internal jugular vein and internal carotid artery also resides, as the main blood suppliants for the brain.
Fig. 11 – 1: SCM, 2: anterior scalene, 9: vagus nerve, 10: phrenic nerve, 14, carotid sheath
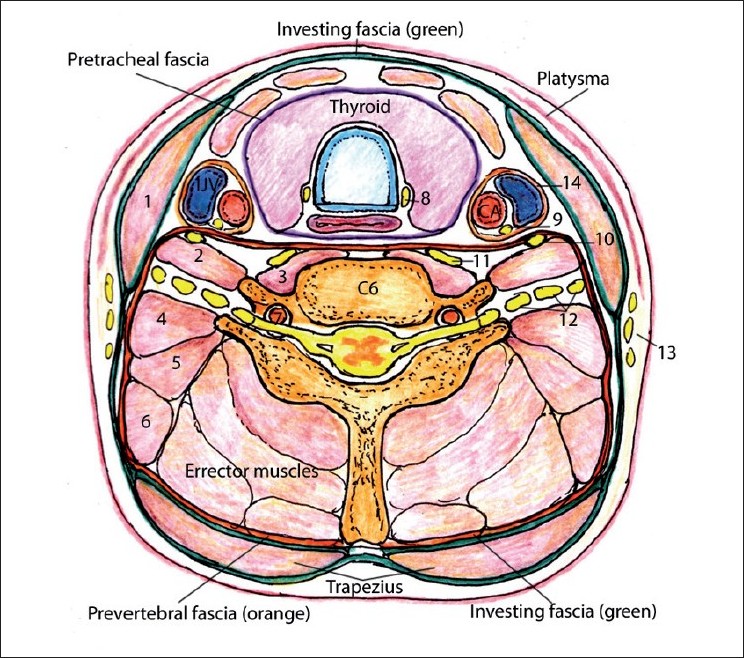
When the clavicular portion of the SCM and the anterior scalene becomes very tight (often when severely weak), this may cause entrapment of the above-mentioned nerves and vascular structures. Chronic cough, headaches, migraines, cervicogenic headaches and all kinds of different symptoms may be experienced as a result. I’ve treated several patients for chronic cough caused by vagal compression within the SCM / scalene interval.
Below is an exercise demonstration for the sternocleidomastoid.
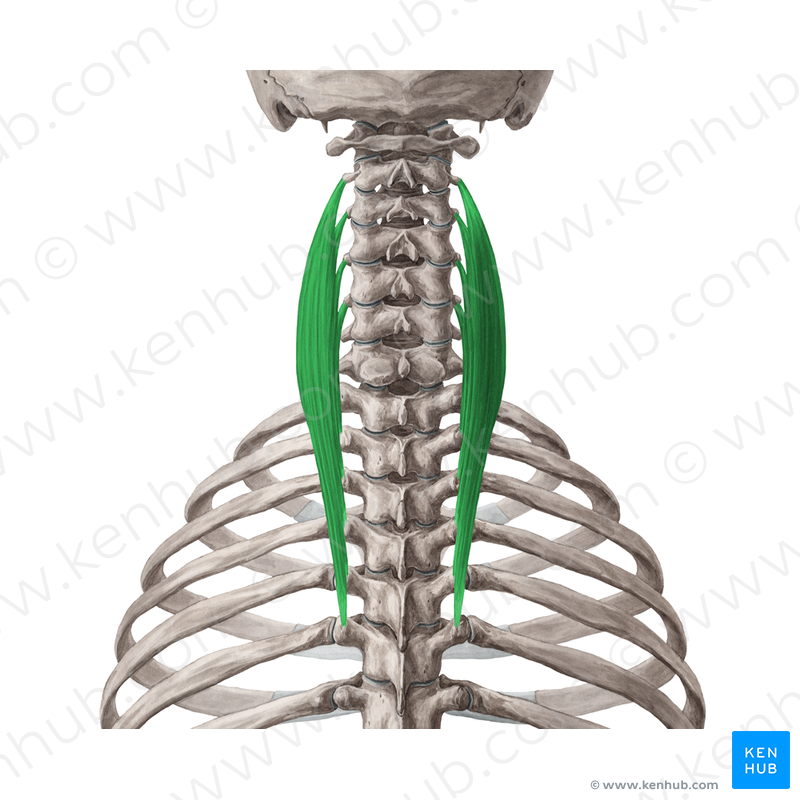
The splenius cervicis and longissimus cervicis
The splenicus cervicis is a cervical spinal erector, and spans between the transverse process of the C1 & C2, and down unto the T6 vertebrae. It also contributes to some ipsilateral flexion and rotation of the cervical spine.
Because it attaches to the atlantoaxial joints, it may restrict the motion between these vertebrae and thus promote excessive movement at the atlanto-occipital junction, if there is significant tightness, perhaps due to forward head posture or similar factors.
Fig. 12

The longissimus cervicis does not attach to the atlas, but rather spans between the C2-C6’s transverse processes, and down unto the T1-T5. Similar to the splenius cervicis, it will contribute to cervical extension, as well as some ipsilateral rotation and lateral flexion.
Although it does not restrict atlantal movement, it will restrict mid- and lower cervical movement if there is severe tightness. Restricted axial rotation of the cervical spine may, as mentioned several times already, lead to excessive atlantoaxial movement, compromised joint integrity (laxity, subluxations), and so on. The main factor for this is once again forward head posture. As you know, there’s much greater movement at the A-A junction than the A-O junction, so the margin of error is much greater here than at the above level. Even minor laxity at the A-O junction, which may occur if the atlantoaxial joints are both restricted, can be quite detrimental. More on this throughout this article.
Fig. 13
Here is an exercise demonstration for the cranio-cervico-thoracic extensors.
Common causes of misalignment
This has been touched on already, but this section will address the various causes of atlas joint instability and misalignments. The most common precursor is forward head posture with cervical hinging, or cervical injuries such as whiplash. This will cause massive instability and may often pave the way for atlas misalignment down the lines. Furthermore the jaw will also affect posture and cervical stability, as will scapular positioning and resting habits.
The head weighs between eight and 14 pounds. It must remain in perfect alignment in order to prevent interference in every brain-to-body function. Misalignment can result from automobile accidents, poor posture, falls and countless other causes. When the head becomes misaligned, it reacts adversely with pain and poor health. – Dr. Peter Gott M.D.
Fig. 14

The jaw’s effect on posture and the upper neck
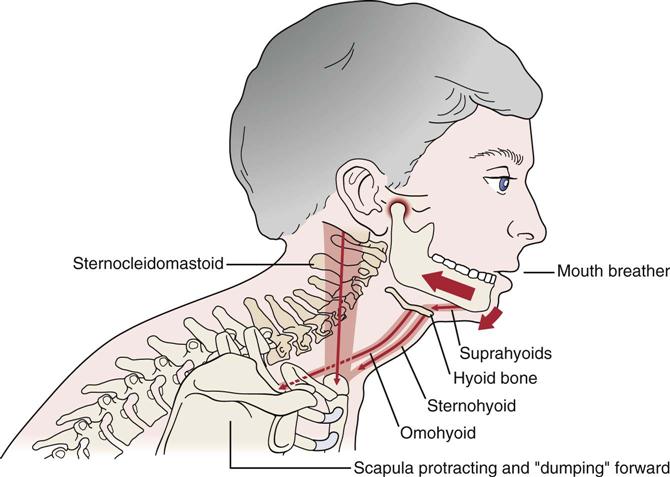
Crooked atlas positioning is also often related to temporomandibular dysfunction (TMD). Many studies have shown significant associations between tooth occlusion (the bite) and posture. For example, people with tooth crowding have a significantly higher chance of getting forward head posture (Solow et al., 1998). Now, it is not the only cause of FHP, but I want to address this topic before addressing FHP and the corrective strategy I use for it.
Many dentists agree that the most common trait of people who have dental crowding and improper development of the upper jaw, is that they are walking around with the mouth open, breathing through it instead of through the nose, and that their tongue is not properly situated in the roof of their mouths in posture. When the jaw remains open and the tongue is lying down, not only will the face and cranial bones develop asymmetrically, together with the occlusion, but cervical tensegrity is lost along with it. When tensegrity is lost, the neck becomes unstable, and over time this may cause atlantal misalignment. Furthermore, underdevelopment of the maxilla may cause TMD in many circumstances.
If we look at Thomas Myer’s ‘deep front line’, we can perhaps understand why the jaw is so intimately connected with cervical stability. The longus colli and longus capitis, whose functional integrity are absolutely essential for neck posture and stability, are directly connected to the tongue and muscles of mastication through fascial bonds. Research has shown that a staggering 30 to 40% of muscle force transmission actually occurs through these bonds, and not the muscle itself (Huijing et al., 2003; Stecco et al.,). These bonds continue all the way down, through the core and unto the foot. Then, when [especially] the tongue is not properly positioned, and the muscles of mastication are not stimulated properly, the subsequent loss of tensegrity may cause a spiral effect through all of the deep front line, affecting our posture.
Fig. 15
I do have some more hypothetical thoughts with regards to why malocclusion may directly affect posture through changing the alignment of the sphenoid bone (through whom all of the ocular nerves pass), as I’ve found that stimulating the pterygoid muscles in certain ways, will contribute to relatively predictable craniocervical movements. For instance I’ve found that the medial pterygoid will promote contralateral cranial tilt, and the lateral pterygoid, contralateral cranial rotation. However, this topic is too esoteric and will probably end up in an article on its own, rather than being elaborated upon here in this one.
I must elaborate on an important topic with regards to the occlusion vs. posture phenomenon. It has become a popular notion within dentistry and related communities, that posture is impossibly altered without addressing dental occlusion. While I agree that dental occlusion will help, it is without a single doubt NOT necessary to balance occlusion to improve posture with permanent gains. It is a false claim.
Dental occlusion does guide posture to some degree, I think this is well proven in much literature as well as clinically, however it is paramount to understand that we can override this guided dysfunction by being aware of our habits, and incorporating good habits. Poor occlusion can not override our efforts. For instance, poor dental occlusion may increase the patient’s tendency to hang forward with the head, due to reduced cervical tensegrity. However, being aware of this, we can easily change it.I know that many claim otherwise, but I can assure you that I’ve resolved a lot of patients postures who had significant malocclusion. It is absolutely doable with some work and discipline. Here’s some interesting research on the topic of occlusion and posture. I’ll address this in the next section.
A clear pattern of associations between crowding and craniocervical posture was found. – Solow et al., 1998
According to the literature reviewed, we believe that there are real correlations between posture and the SS (stomatognathic system). In this way, an increase in postural swaying may indicate a general malaise caused by problems in the SS. – Cuccia et al., 2009
The individual’s postural position can suffer biomechanical alterations due to stomatognathic alterations, causing clinically visible changes in dysfunctional individuals and affecting the performance of the involved structures. – Strini et al., 2009
Significant correlations could be obtained with respect to the facial axis and the lordotic angle, the facial axis and the pelvic inclination, the inner gonial angle and the lordotic angle, the inner gonial angle and the pelvic inclination, the mandibular plane angle and the lordotic angle, the mandibular plane angle and the pelvic inclination, as well as the facial depth and the pelvic inclination. – Lippold et al., 2006
Five animals received no alteration on their bite. Bite was increased on 10 animals and molar teeth were extracted on 10 other animals. Frontal and lateral radiographs were taken on days 0, 7, 14 and 21. Distances from landmarks to a true vertical line were measured on both radiographs. Results: Repeated measures analysis showed statistically significant differences between the amount of the curvature at the cervical and thoracic spines on frontal and lateral radiographs over time Ramirez-Yanez et al., 2014
The data that is available points to the existence of a correlation between posture and occlusion and also asserts the prevalence of associations between cranio-facial anomalies and idiopathic scoliosis in adolescents. – Amat et al., 2009
The data confirmed a beneficial effect of balancing the occlusion with an acrylic wafer on the following paired postural muscles: sternocleidomostoid, erector spinae, and soleus. – bergamini et al., 2008
Based on these findings, it was concluded that changing mandibular position affected body posture. Conversely, changing body posture affected mandibular position. – Sakaguchi et al., 2007
The findings indicate that eye dominance and direction of head rotation are strongly associated in both TMJ and control subjects. Further, in TMJ subjects mandibular deviation occurred in greater frequency than in controls and tends to occur in the contra lateral direction of head rotation. – Pradham et al., 2001
Postural problems were significantly more common among children in the group with mouth breathing syndrome, highlighting the need for early interdisciplinary treatment of this syndrome. – Conti et al., 20111
High mouth breathing prevalence without significant statistical difference between genders,age and type of mouth breathing. There was no association between behavior characteristics and type of breathing. There were significant differences between physical traits and breathing pattern. – Braz, 2006
It was observed that mouth breathers do maintain an extended head posture, which was evident from a decrease in distance between the occiput and dorsal arch of atlas vertebra. – Kumar et al., 1995
The mouth breathing group exhibited reduced cervical lordosis, increased thoracic kyphosis, increased lumbar lordosis and the position of the pelvis was tilted forward. The distance traveled outwards by the diaphragm muscles of mouth breathing children was shorter than that traveled by the muscles of nose breathing children. – Yi et al., 2008
Mouth breathing children presented pathologic adaptations in the postural and morphological characteristics of the stomatognathic system. This suggests the importance of early diagnosis in order to avoid orofacial alterations. – Cattoni et al., 2007
TMD exacerbated by cervical instability
When the neck is unstable, many patients may start to habitually clench the suprahyoid muscles in order to create some cervical stability. The suprahyoid muscle complex can mimic the functions of the longus colli and longus capitis, by pulling the head into flexion and may thus somewhat restrict forward head posture (although not effective in preventing cervical hinging).
Fig. 16
One massive problem with this strategy is that the suprahyoid pulls the mandible backward, and when the mandible is pulled back, TMJ shear forces greatly increase, over time causing disc ruptures and TMD symptoms. This is why many people also get jaw pain after first acquiring cervical issues (e.g after a neck injury), but the opposite may of course also occur, as TMD exacerbates cervical instability as well, as shown above.
Fig. 17
TMD is mainly caused by underdevelopment of the maxilla, resulting in a dental occlusion that is established too far back. This will cause the mandibular condyle to rest too far back, and thus jam too hard into the TMJ, and wear the joint down over time.
This can be relatively easily resolved by getting the mandible forward in posture, strengthening the pterygoid muscles, and establishing proper tongue posture, as all of these factors contribute to decompression of the TMJ. However, if cervical stability is not regained, and the patient keeps clenching their suprahyoid muscles, this will most likely make it impossible for the patient to alter their mandibular posture, and thus also very difficult to cure TMD. Once again, a multifactorial approach is required to resolve this issue.
Read my TMD-article for more detailed information on this topic. I can not possibly include it all in this article; it’ll become so long that no one will read it!
Forward head posture and ‘the dreaded cervical hinge’
As I see it, forward head posture and neck hinging is perhaps one of the most detrimental habitual factors with regards to cervical stability. Virtually every patient with atlas misalignments will have forward head posture and cervical hinging. Let me explain why I think this is such a big deal, and why it will affect atlantal stability and alignment.
The first rule that we need to know about, is that if the patient is in swayback posture, it is almost impossible to correct forward head posture in solitude. If the pelvis is anterior to the thorax in posture, the nervous system will attempt to maintain equilibrium by pulling the head and shoulders down and forward. Thus it is close to impossible to get lasting results with regards to craniocervical positioning if swayback posture is not addressed first. I’ll talk more about this in the treatment section as well as demonstrate it in a video.
In continuation; if the cervical spine is too kyphotic (forward head posture) and especially if there’s a hinge at one of the cervical levels, this may cause severe movement impairment of most of the cervical spinal segments, as axial rotation is compromised. In turn, this will cause abnormal increase of movement to occur within the upper vertebral segments, especially the atlas joints, in order to uphold normal daily life cervical mobility. Over time, the protective ligaments of the upper cervical spine will loosen up and will thus no longer be able to withstand excessive motion between the A-A and A-O joints. Atlanto-occipital, and perhaps more commonly noted, atlantoaxial laxity and hypermobility will often occur as a result.
Fig. 18

In the image below we see patient whose lower cervical spine is hinging, and over time this has caused a buildup of connective tissue at the region of dysfunction (Langevin et al., 2009 has a good paper talking about this phenomenon, in the lumbar spine). The hump that occurs is called dowager’s hump aka buffalo hump. In addition to being a common cause of disc injuries at the given spinal segment as well the proximate levels, ‘the hinge’ will cause regional muscular dysfunction. This is indeed serious if it’s not getting noticed nor addressed. The reason for this is that muscular structures need to have a solid holding point in able to pull origin toward insertion or vice versa. When the muscular origin, such as the transverse or spinous processes of the neck are ‘loose’ due to an unstable foundation (the level of the hinge), most of the muscles that attach in the region will become inhibited by the nervous system, as the nervous system do not allow pulling on unstable structures.
Fig. 19

When muscle testing cervical structures of patients who have this dysfunction, global cervical inhibition is often present. And, of course, the patient is usually in pain. Headaches, migraines (hinging may occlude the vertebral artery and vein, more in my migraine article), muscle pain, stiffness, disc herniations, spondylotic injuries and so on. Again, global cervical loss of tensegrity will often occur, which is why it is of paramount importance to identify and treat the cervical hinge.
To identify the hinging pattern, first have a look at the patient’s posture. The neck will usually be visibly hyperextended at one level of the cervical spine, usually at the lower or middle levels. Additionally, and also as a double check if there’s no obvious hinge, run your fingers down the spinous processes and feel for an asymmetrical indent (divot) between these spinous processes. For example, when palpating the spinous processes at the C6-7, which is where most patients hinge on their neck, you’ll feel an obvious decreased prominence of the C5-6 spinous process, which should be just slightly anterior to the C7 spinous process.
If the hinge is identified, this means that the patient’s habits are poor, and that the longus colli and longus capitis (i.e the deep neck flexors) are inevitably weak and inhibited by this nasty habit. Yes, their dental occlusion is probably also poor, but changing habits is free where as fixing occlusion is a very slow and expensive project, and finding a truly skilled dentist (such as Michael Mew or Anthony Sims) is very difficult. And, a more or less unnecessary project if one knows how to treat posture and the TMJ conservatively. I know that this challenges the current paradigm, i.e the unwritten law of therapy for chronic jaw and neck pain sufferers. Much because dentists are some of the only professionals that are able to help these patients.
This is not, though, because dental approach is the only approach. It is because current conservative postural and corrective means are simply of poor value. Common practices for postural and muscular correctives often lack important nuances and tend to be wrong, and even downright detrimental. I know this is tough to swallow for some of you, especially if you are a therapist yourself, but let’s face it; these patients are rarely being helped by conservative measures. If the current therapeutic means were effective, they would be better. Let’s not fool ourselves – And let’s keep an open mind. With proper TMJ and cervical postural correctives, no occlusive work is needed in my experience.
To get the patient out of the hinge, it is not sufficient to simply strengthen the deep neck flexors. We need to consciously change the patient’s habits (the cause), and strengthen the deep neck flexors (the symptoms). When we address both the cause and the symptoms, the patient will get better, faster. If we address just the cause, it’ll take forever to get well. If we address the symptoms, most often it won’t be an effective treatment, and other times it simply won’t give lasting results. It depends.
So, back to the point; once the hinge has been identified, the patient needs to learn to be ‘long in the neck’ by pulling the back of their head up toward the roof, and gently pull the chin down (cue courtesy of Evan Osar’s book from 2012) . Re-palpate the spinous process after the correction, and if done properly, the spinous processes will now be of natural symmetry, indicative of proper alignment. This will restore tensegrity (i.e muscle function and tension) and proper alignment in the cervical spine and pave the way for healing. This is not a mere exercise, it’s a permanent postural change. The patient must learn to stay there forever, and it’ll be hard in the beginning but they’ll get used to it, and then it will feel tremendously better.
As already mentioned, forward head posture and cervical hinging will often lead to hypermobility of the upper cervical junction, as the spine’s movement is impaired and is thus not able to rotate axially as one unit any more. It will also often cause hypermobility in regards to extension, and ability to properly extend the occiput is often lost.
If you recall, the sternocleidomastoid and suboccipital muscles are the ones that mainly extend the head, and of course these muscles will become inhibited and atrophied as the years go by without them being properly utilized. Sadly these muscles have gotten an infamous reputation for being “over-active and tight”, but this could not be further from the truth. Seeing therapists needle and massage these muscles, only to, potentially exacerbate the patient’s dysfunction down the line (many get this ‘treatment’ for years on end).
Muscles should be thick and and have a decent amount of tone, if they are strong and working properly. It’s a great misconception that muscles should be sloppy and soft; they should NOT. Rather, soft and hypotonic muscles are most often inhibited, and thus weak, tight and painful (both to touch and otherwise). Using muscle tests and exercise strength tests as well as evaluating tonus and thickness of muscles, will help to get a true status of the given muscle’s function and ability, rather than ‘tightness’ alone, which means absolutely nothing when interpreted in solitude.
Back to the point; after years of cervical hinging, many clients thus lose their ability to extend the occiput properly. This will exacerbate spinal hyperextension and promote dysfunctional movement- and muscle activation patterns, which in turn causes a worsening of atlas joint instability. It is of utmost importance to not only re-establish proper cervical alignment, but to also teach the client how to rotate and extend the neck and head without falling back into the hinging pattern. In addition to this, of course, we will exercise the suboccipital, longus colli and longus capitis muscles, which I refer to as the ‘trio of success’, as they both stabilize the atlas joints, syncronize their movements and maintain a ‘long neck’ position during craniocervical movements.
Palpation of these muscles, especially the suboccipitals in patients with severe cervical dyskinesia and misalignment, will commonly reveal significant hypotrophy and lack of tone. When the suboccipitals aren’t firing properly, they’re not able to syncronize the cranium with the eyes’ motions, and thus vertigo, sea sickness, car sickness and similar symptoms of seemingly vestibular origin will occur. In reality, it is craniocervical instability.
It is of paramount importance to identify and treat the cervical hinge, and restore proper cervical kinematics. This is a topic not widely discussed; rather, it is like the beast of cervical dysfunction that no one are talking about nor treating. Therefore, as I touched upon already, most symptomatic treatment will not prove very fruitful, especially in the long run. The hinge MUST be corrected if supplementary therapy is to be successful, in my experience. It is definitely not enough to normalize dental occlusion, in my experience.
Scapular depression
Another common association with swayback posture, is scapular depression. I.e, improper resting position of the shoulder blades. When the scapula is resting too low in posture, the trapezius, levator scapulae and scaleni muscle groups will commonly inhibit and become very tight. The tighter they become, the greater they will restrict normal cervical posture and movement. This may once again lead to hypermobility of the upper cervical region, cervical hinging, and so on, which are all common denominators that pave the way toward atlas misalignment issues. Furthermore, It is almost impossible to resolve forward head posture, if the shoulderblades are situated too low, as it will pull the neck down and forward, often into a hinging pattern.
The scapula should be resting between the T2 and T7 vertebrae height wise, which means that the superior scapular angle should be in level with the T2, and the inferior angle in level with the T7. Lower than this, and the trapezius will inhibit. Higher than this, and it usually indicates a dysfunction of the levator scapulae, which is also not beneficial. The trapezius should be mildly active in posture, NOT relaxed as many mistakenly, and iatrogenically claim. The trapezius muscle is the main stabilizer and load bearer of the scapula, and is thus an extremely important muscle. When the trapezius inhibits in posture, bad things tend to happen, both to the neck and to the shoulders!
Below you can see two images of improper, and proper scapular resting position. On the right we see significant depression and some scapular winging, a very common appearance for people with neck and shoulder pain. On the left, however, we see proper upward rotation and height in resting position, caused by a healthy and functioning trapezius muscle. Do not pay attention to the muscle mass, that’s not at all the point here. The point is the scapular positioning.
In addition to normalizing scapular resting positioning, I recommend strengthening the trapezius. The levator scapulae can also be strengthened, but I’ll get back to exactly how and why a little further down, as this muscle greatly affects the atlas joints. If you want to learn more detailed information about scapular posture and movement, you’ll have to review my scapular dyskinesis article.
Fig. 20

Other contributing factors
Other factors could be work with extremely monotonous movement patterns, especially on one side or toward a certain direction. I could impossibly list all such examples, but just make sure that you balance out whatever the patient is doing at work, with the correctives that are prescribed.
As a therapist, for example, I look down a lot. Looking down in large portions of the day will inhibit the suboccipitals (this is quite common for many professions who look down a lot, such as hair dressers), and it will therefore be necessary to do maintenance work on these muscles in order to keep them adequately functioning. Certain machinery may require the operator to continuously look toward a certain direction, or continuously load and use the arms very differently.
The hairdresser below, for example, would be required, first of all to use a better general posture, but because looking down a lot every day is more or less inevitable, it would be beneficial to strengthen the neck flexors and suboccipitals.
Fig. 21

Monotonous cervical and occipital movement is perhaps a greater precursor to dysfunction than imbalanced shoulder loading, but all of these kinds of factors should be considered. If the person has a job or hobby that promotes monotonous movement patterns, it’s a good idea to balance this out with regular maintenance work for the muscles that aren’t being stimulated. I generally do not recommend much stretching when it comes to dysfunction, but dry needling or massaging of certain muscles may prove beneficial in these exceptional circumstances.
The sideways forklift seen below is another example, and is a pretty horrible piece of machinery. It promotes extremely monotonous and downright detrimental cervical habits. Yes, so does the hairdressing, but continuously looking to one side (rotation) is genereally worse than flexion/extension patterns. Problems that would arise at the below situation is that not only will be left levator scapulae become stretched, and pull the atlas into leftward rotation, but it’ll also become weak. The right levator will shorten and is unlikely to get tense enough to balance the atlantal pull and encouraged torsion that is coming from the left side.
In cases like this, extremely good posture while working, as well as cervical flexibility will required. Furthermore, maintenance correctives to the atlas, although not optimal, is probably inevitable. Moreover the suboccipitals, left levator scapulae, right SCM, right scalenes, as well as the deep neck flexors would all most likely require maintenance strengthening. If you drive a lift like this, however, and I’m talking about those who do so for large portions of the day; the best option is probably to demand another machine, or to find another job!
Fig. 22
![]()
These are of course just examples. A thorough examination is key, together with good questions, to reveal any potential cause of dysfunction. An evaluation will have to be made with regards to whether or not the monotonous work or hobby is or is not a burden too great for the patient’s condition.
Potential consequences of misalignment
Extremely many conditions are associated with atlas misalignment, however I can not possibly include every single association, as there are so many, and I have mentioned several things already throughout this article, so I will try to stick to new information rather than reiterative rambling.
If you search for it on the internet, you will find that many claim it to be the cause and solution to virtually anything. I agree that many things are associated with atlas misalignment, but I do not necessarily agree that they’re all caused by atlas misalignment. In my experience, however, the same causes of atlas misalignment may also cause issues such as thoracic outlet syndrome, severe muscle imbalances, headaches, postural abnormalities, and so on. In this section I will try to address the symptoms that I think are more or less directly related to atlas misalignment.
What came first, the hen or the egg?
Potential direct symptoms caused by atlas misalignment are: upper neck pain, vertigo, intracranial vasal hypertension, vertebrobasilar insufficiency (from atlantal torsion), imbalanced posture, cerebellar herniation (chiari). Even stroke and death can occur in extremely rare & severe cases (don’t get scared; people also die driving cars, so take a deep breath and relax. I must mention these things if I am to get all the necessary information into the article.) Thankfully though, in extreme cases, any conventional ERs will more than likely identify such an issue, e.g vertebral artery dissection or brain stem compression.
Usually though, the underlying cause and exacerbative factor of the atlantal instability, will carry many symptoms on its own. Such underlying causes may often be whiplash injuries or extremely poor postural habits and/or dental occlusion, over time leading to forward head & generally poor posture with neck “hinging”, thoracic outlet syndrome, cervical disc herniations, vertebrobasilar insufficiency (from TOS), headaches, muscle imbalances and muscle pain.
Vertigo / dizziness
Atlantal misalignment is a common cause of symptoms that may appear to be of sole vestibular origin, but rather originate from upper cervical dysfunction. The three most common causes for this are 1: thoracic outlet syndrome, causing symptoms of vertebrobasilar insufficiency (by occluding the vertebral artery), 2: dysfunction of the suboccipital muscle complex, and 3: Compression of the internal jugular vein. There is also a fourth and more rare cause, called bow hunter’s syndrome, where the A-A or A-O joints have become very lax, and therefore compromised.
Fig. 23

Compression of the internal jugular vein is probably the factor most relevant to the vestibular system, as it may prevent drainage of endolymphatic fluid from the cochlea and vestibular chambers.
The inner ear senses both balance and hearing based on movement of hair cells within the vestibular chamber and scala media of the cochlea. These hair cells are moved by a fluid called endolymph. For hearing and balance to be normal, endolymphatic fluid must be in homeostasis (balance). Increase of endolymphatic fluid will cause hearing loss and excessive movement of the hair sensory organs within the semicircular canals, causing vertigo, which is often the case with Meniere’s disease patients, vestibular migraines and similar.
Many studies show the correlation between excess endolymphatic fluid and dizzness, but also hearing loss and migraines. The reason for this is mainly that compression of the internal jugular vein, which is a common problem patients who hinge at the neck and/or have atlas torsion, will cause impaired venous drainage from the inner ear and thus increase susceptibility to endolymphatic hydrops (excess endolymphatic volume and pressure). It may, of course, also cause generalized craniovascular hypertension in various degrees of severity, which may cause migarine.
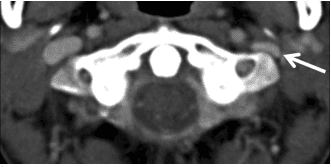
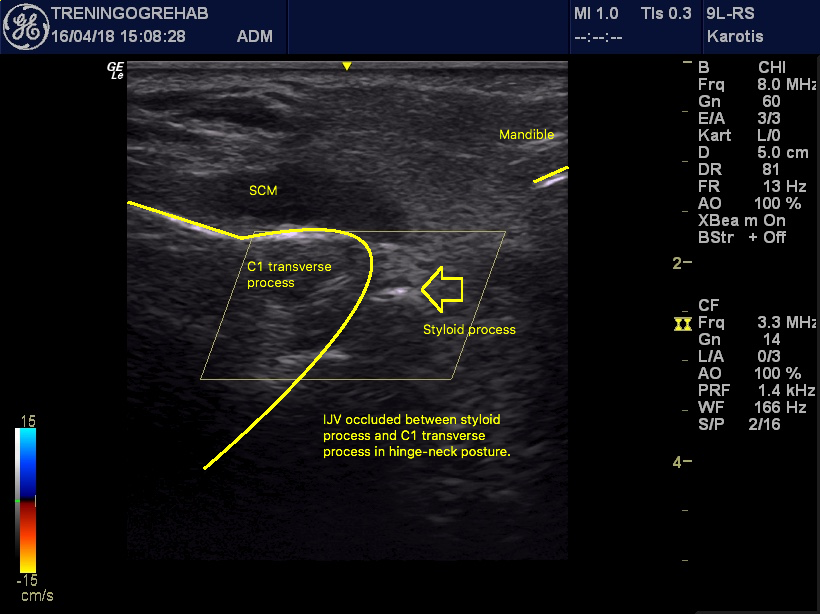
The CT scan below shows that the left IJV is compressed by the atlas vertebrae’s transverse process in a migraine patient, as it has torsioned toward the right. Symptoms were only present on the compressed side (left). Note the difference between the transverse process and the mandibular ramus on the left and right sides. Arrow shows compression of internal jugular vein.
Fig. x – Gweon et al., 2011
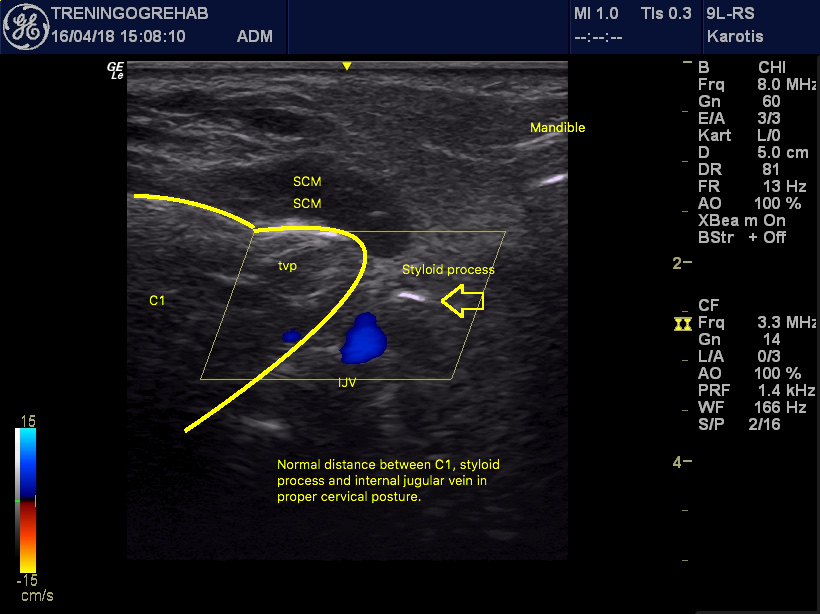
On ultrasound you can also see, even in healthy patients with no anterior translation or rotation of the atlas, the neck-hinging may obstruct the internal jugular vein. A sensation of craniovascular hypertension may build up within seconds. Much more so if there is atlantal misalignment.
In the image below, where there is good cervical posture, there is a decent margin between the IJV and atlas.
Fig. x
When the neck hinges backward, however, the atlas drives forward into the IJV and occludes it, causing craniovascular hypertension. Seen in realtime in this video.
Fig. x
It has been demonstrated that internal jugular vein (IJV) compression aggravates headache intensity in patients of migraine. In the result, the venodilatation of IJV in response to each level of Valsalva pressure in patients with migraine was significantly less than that in normal individuals. – Chung et al., 2010
We aimed to assess whether migraine is associated with changes in the distribution of the venous drainage through primary and secondary pathways by using phase-contrast magnetic resonance imaging (MRI). Cine-phase contrast scans with high-velocity encoding were employed to quantify arterial inflow and flow in the primary venous channels (right and left jugular veins), whereas scans with low-velocity encoding were employed to quantify flow in the secondary venous channels (epidural, vertebral, and deep cervical veins). CONCLUSION: Migraine patients showed a significantly larger percentage of venous outflow through secondary channels. The mechanism of this alteration remains to be elucidated. Potential mechanisms include repeated release of vasoactive substances or growth factors. – Koerte et al., 2011
The diameter of IJV and distance between the styloid process and lateral mass of the atlas at IJV obstruction side in obstruction group were 1.6 ± 1.0 mm and 4.1 ± 2.1 mm respectively, which resulted in statistical significance (p<0.01). The maximum area of lateral mass of the atlas at IJV obstruction side in obstruction group was 103.4 ± 25.3 mm2 which is significantly larger than in control group (p<0.05). – Gweon et al., 2011
Episodic vertigo is usually due to endolymphatic hydrops, distension of the inner ear membranes, and may be primary (Ménière’s disease) or secondary (otic syphilis, delayed endolymphatic hydrops, Cogan’s disease, recurrent vestibulopathy). Patients with typical Ménière’s disease have recurring attacks of vertigo, sensorineural hearing loss, tinnitus, and, sometimes, a fluctuating fullness in the ear. – Smouha & Wanna, 2009
The symptoms of progressive endolymphatic hydrops can be correlated with two principal types of pathologic change: (1) distentions and ruptures of the endolymphatic system,2,3 and (2) alterations in the cytoarchitecture of the auditory and vestibular sense organs, sometimes accompanied by atrophic changes. Coincident with rupture, there is sudden contamination of the perilymphatic fluid with neurotoxic endolymph (140 mEq/L of potassium) that causes paralysis of the sensory and neural structures and is expressed clinically as episodic vertigo, fluctuating hearing loss, or both. – Schuknecht, 2010
In animals with surgically induced hydrops, similar anatomical changes are found to those in patients, including degeneration of fibrocytes in the lateral wall, loss of spiral ganglion cells, disruption of hair cell stereocilia, and eventual loss of hair cells (Nadol, J. B., Jr. et al., 1995) – Harris & Salt, 2008
Micromechanical indentation of the horizontal canal (HC) duct and utricular vestibule was used to simulate sinusoidal head rotation and fluid volume injection. Single-unit neural spike trains and endolymph pressure within the ampulla, on both sides of the cupula, were recorded simultaneously. ΔP averaged 0.013 Pa per 1°/s of sinusoidal angular head velocity and P0 averaged 0.2 Pa per 1 nL of endolymph volume injection. The most responsive afferents had a threshold sensitivity to ΔP of 10-3 Pa and to P0 of 5 × 10-2 Pa based on a discharge modulation criterion of 1 impulse/s per cycle for 2 Hz pressure stimuli. Neural sensitivity to ΔP was expected on the basis of transverse cupular and hair bundle deflections. Analysis of mechanics of the end organ, neuronal projections into the crista, and individual neural firing patterns indicates that P0 sensitivity resulted from pressure-induced distension of the ampulla that led to a nonuniform cupular deformation pattern and hair bundle deflections. – Konrádsson et al., 1994
The pathogenesis of isolated headache in cerebral venous thrombosis (CVT) in the absence of intracranial hypertension, SAH, meningitis or intracerebral lesion is unknown but may involve changes in the walls of the occluded sinus. Hence MRI/MRV should be used to look for signs of CVT in all patients with recent headache (progressive or thunderclap) even when the CT scan and CSF examination are normal. – Cumurciuc et al., 2005
Normal venous drainage of the vestibular organs through the vein of the paravestibular canaliculus (PVC) may be crucial to inner ear fluid mechanics. It is proposed that increased venous pressure, with resultant venous insufficiency of the vestibular organs, may result in endolymphatic hydrops unless collateral venous circulation develops. Certain variations in pattern of venous drainage where the vestibular organs drain predominantly through the PVC vein may be a predisposing factor. In patients with Meniere’s disease, different mechanisms can cause venous insufficiency. One suggested mechanism is morphologic change in the microcirculation of the intermediate portion of the endolymphatic sac. Microcirculation changes may be associated with fibrosis of the perisac tissues or shortening of the intermediate sac region or might be physiologically determined. Venous insufficiency may also result from anomalies of the PVC vein – Gussen, 1983
Entrapment of the cervical ganglia and sympathetic chain
Neck hinging will cause dysfunction of the longus colli and longus capitis muscles, as explained earlier. Between these muscles and the alar fascia, resides the sympathetic chain and its cervical ganglia. Studies have shown that dysfunctional musculature cause increased density, thickness and rigidity of connective tissue. This is why we so often see nerve entrapment syndromes nearby dysfunctional musculature (more on this in my lumbar plexus entrapment article). Thus, fascial restrictions may develop subsequent to dysfunction of the longi muscles, causing friction and reduced neural tissue gliding, leading to irritation of the cervical ganglia and sympathetic chain.
Fig. X
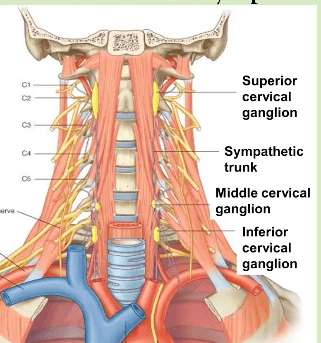
Fig. x
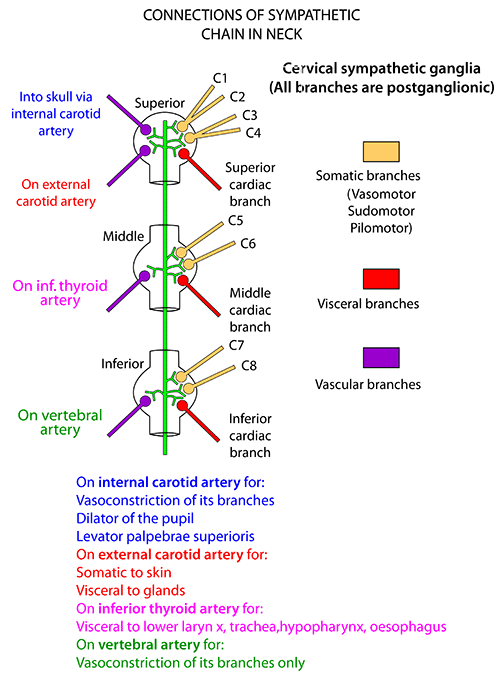
The cervical ganglia controls a lot of processes in the body, and the symptoms may therefore be quite diffuse. Knowledge of this phenomenon and its associated potential symptoms is required in order to detect and treat the issue.
For example, the superior cervical ganglion innervates the vestibular system, the eyes, carotid bodies, pineal gland and so on. Not surprisingly, Ménière’s disease, which is a vestibular disorder of supposed idiopathic origin, has been associated with dysfunction of the superior cervical ganglion. Tinnitus has been associated with the cervical ganglia as well. I’ve also found irritation of these nerves to cause itchy ear syndrome, which is a problem often reported by Ménière’s sufferers.
With regards to the eyes, they control dilation and constriction of the pupils, and may thus affect vision, concentration and so on. Moreover, it has been documented that both tinnitus and ocular impairment may occur post whiplash injury. It may even explain why the term “book worm” came into play; meaning, the child’s maladaptive vision may be caused by improper cervical postures, which in turn cause irritation of the cervical ganglia. The latter, though, is hypothetical, but not so far fetched in my opinion. I cited a somewhat relevant study below, where kids with myopia (near-sightedness) and hearing loss (hearing loss has also been somewhat associated with sympathetic disturbances (Bielefeld & Henderson, 2007)) had a tendency to have poor craniocervical postures. It is, however, unsure whether or not the poor postures occurred first.
Complex regional pain syndrome pain syndrome has also been correlated with disruption of the cervical sympathetic chain (Yucel et al., 2009; Meredith C.B. Adams, Robert W. Hurley, in Practical Management of Pain (Fifth Edition), 2014), along with Reynaud’s diease (Shreeve & La Rose, 2011) and probably many other diffuse topics.
Fig. x
Myofascial entrapment of the cervical sympathetic chain and ganglia may be relieved by optimizing cervical posture, atlantal alignment and strengthening the longus colli and longus capitis muscles. All of these measures are detailed throughout this article.
Note: Because of the great amount of possible references, I have had to limit the quote quantity below. More research definitely exists, and may be found by searching for it.
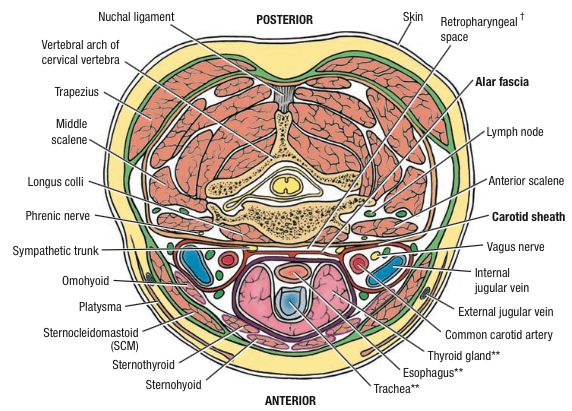
The sympathetic chain is enclosed within the alar fascia, a thin fascia that separates the cervical sympathetic chain from the retropharyngeal space. The carotid sheath is connected to the alar fascia by a mesothelium-like fascia. The fascial plane that encloses the sympathetic chain may be in direct communication with several spaces and structures, including the brachial plexus, vertebral artery, endothoracic fascia, and the thoracic wall muscle at T1-T2. At the C6 level, the cervical sympathetic trunk is located posterolaterally to the prevertebral fascia on the surface of the longus colli muscle. – Adams et al., 2014
The cervical sympathetic chain lies anterior to the longus colli and longus capitis muscles and deep to the prevertebral fascia – Civelek et al., 2008
The effect of novocain block on vertigo of Menie’re’s disease.-I have had the satisfaction of abruptly terminating two cases of Meniere’s disease during acute severe attacks by means of a procaine block. One case occurred at the Wembley Hospital. The patient was wheeled into the theatre lying curled up vomiting, with nystagmus, pallor and sweating. 5 ml. of procaine were injected in the stellate ganglion and within three minutes the patient had recovered sufficiently as to walk back unaided to the ward. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus
Superior cervical ganglion neurons project to the dilator pupillae muscle of the iris to control pupil dilation. Ocular blood flow is controlled both via direct autonomic influences on the vasculature of the optic nerve, choroid, ciliary body, and iris, as well as via indirect influences on retinal blood flow. – McDougal & Gamlin, 2015
It is generally believed that the cause of Meniere’s disease is related to autonomic dysfunction (Hilger’, 1950; Beickert’, 1953; Watanabe10, 1955; Hisaki’, 1960; Williams”, 1965). The positive rate showing a response of either the sympathetic hyperreactor or sympathetic hyporeactor type in the cases with Meniere’s disease and aural vertigo was 79% and 87% respectively in the acute stage when nystagmus was present. – Uemura et al., 1972
After local anesthetic was applied to the facet joints, patients reported within 10 minutes that their tinnitus had diminished significantly. Simultaneously, mydriasis disappeared. In one patient, tinnitus was controlled completely. Tinnitus can temporarily be reduced by the application of local anesthetic to Cl-C2 facet joints and buprenorphine analgesia of the superior cervical ganglion in patients with Cl-C2 facet joint disorders. – Franz et al., 1998
Whiplash or indirect injuries to the neck as a consequence of motor vehicle collisions are a common occurrence in which the frequency of ocular complications is largely unknown. Ophthalmic and oculomotor function was investigated in a longitudinal study of 39 cases who had their initial ophthalmological assessment within one week of the whiplash injury. Ten of 39 cases had ocular symptoms and signs which developed shortly after the accident. – Burke et al., 1992
Frequently, patients report the development of tinnitus after traumatic injuries. However, to which extent this specific etiologic factor plays a role for the phenomenology of tinnitus is still incompletely understood. – Kreuzer et al., 2012
Symptoms of cervical spine disorders, such as head and neck/shoulder pain, were all significantly more frequent in the patient group than in the control group. Most of the patients (75%) reported a strong association between head neck movements in the atlanto-occipital and atlanto-axial joints and triggered attacks of vertigo. Also, 29% of the patients could influence their tinnitus by mandibular movements. Signs of cervical spine disorders, such as limitations in side-bending and rotation movements, were significantly more frequent in the patient group than in the control group. Tenderness to palpation of the transverse processes of the atlas and the axis, the upper and middle trapezius, and the levator scapulae muscle were also significantly more frequent in the patient group. The study shows a much higher prevalence of signs and symptoms of cervical spine disorders in patients diagnosed with Meniere’s disease compared with control subjects from the general population. – Bjorne et al., 1998
The results of this study indicate that visual and hearing impairments can affect the head and neck alignment of children and this alignment has a significant relation with some of the anthropometrical dimensions. – Daneshmandi et al., 2014
Thoracic outlet syndrome
Thoracic outlet syndrome can lead to symptoms of vertebrobasilar insufficiency, such as vertigo, confusion, and blurred vision, especially during cervical rotation and/or extension. It may also cause migraines, thunderclap headaches and more. And, as mentioned, although this may seem to be a vestibular dysfunction, it may turn out to be of vascular origin. It may also cause entrapment of the vagus and phrenic nerves, as well as the whole brachial plexus, affecting the autonomic nervous system and causing many diffuse issues, such as coughing, tinnitus, clogged ear syndrome, chest pain, heart pain, dry throat, hiccups, difficulty breathing and even atrial fibrillation. Read more in my thoracic outlet syndrome article.
The easiest way to diagnose whether or not there is TOS, is to squeeze into the interscalene triangle. If it reproduces severe neuralgic symptoms (patient will jump in pain on the treatment table), it’s likely TOS. The vertebral artery dissection test (VAD) may also be positive if the patient has TOS, reproducing the symptoms that are described above. I’ll quote some interesting research below the illustration.
Fig. 24
Thoracic Outlet Syndrome (TOS) causes dizziness because of positional compression of the vertebral artery with resultant symptoms of vertebrobasilary insufficiency. Compression of 7,C8,and T1 nerves fibers is responsible for the neck pain. – Selmonosky, 2007
Chest pain or pseudoangina can be caused by TOS. Dorsal sympathectomy is helpful for patients with sympathetic maintained pain syndrome or causalgia and patients with recurrent TOS symptoms who need a second procedure.
Compression of the sympathetic nerves in the thoracic outlet may occur alone or in combination with peripheral nerve and blood vessels. The sympathetics are intimately attached to the artery as well as adjacent to the bone. They may be compressed or irritated in primary or recurrent TOS. Atypical chest pain (pseudoangina) simulates cardiac pain (48). Major indications for dorsal sympathectomy include hyperhidrosis, Raynaud’s phenomenon or disease, causalgia, SMPS, reflex sympathetic dystrophy, and vascular insufficiency of the upper extremity.
Cough attacks elicited by movement of the neck and right arm are reported in a patient who had sustained several shoulder injuries and who had an anterior scalenectomy. The coughing was accompanied by weakness in the right upper limb. At exploration, the phrenic nerve was found adhered to the brachial plexus. The cough attacks disappeared, and the weakness of the right upper limb improved somewhat after lysis of the adhesions between the phrenic nerve and the plexus and after external neurolysis of the upper, middle, and lower trunks. Postoperatively, the patient could elevate his right arm without coughing. – Yamagami et al., 1994
Symathetically mediated atrial fibrillation is observed in the presence of any heart disease, the first effect of which is to provoke a vagal withdrawal. The role of the autonomic influences should be taken into consideration every time conventional antiarrhythmic treatment is insufficient. – Coumel, 1994
A 44-year-old female presented with severe right posterior neck pain and vertigo followed closely by thunderclap headache that was confirmed as right VAD (V4 segment) with delayed right dorsal medullary infarction two days later. Her headache, vertigo, and truncal ataxia were completely improved one week later. – Hsu & Sung, 2014
Dysfunction of the suboccipital muscles
As I mentioned earlier, the suboccipitals syncronize the head with the eyes’ movements. If this function is compromised, vertigo may occur, especially during certain eye- or cranial movements. These patients will virtually always be hinging on their necks, as this promote inhibition of the suboccipitals. Because neck hinging also contributes to TOS, it’s important to distinguish where the symptoms are coming from. Especially IF the patient has TOS as well, which they often do.
A common presentation is that dizziness occurs when looking in certain directions, whilst in certain cranial positions, or after loading the neck. When the atlas is (very) out of alignment, the suboccipital muscles attaching to the C1 and C2 will lose optimal tensegrity, and not be able to function properly. Some will be pulled too far and some become lax. Poor function of the suboccipitals may also migraine-like symptoms in and around the eyes.
Bow hunter syndrome
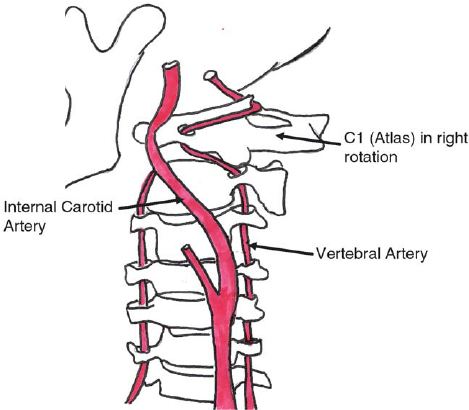
Through the transverse foramen of the (C6-) C2 and C1 vertebrae, through the posterior atlanto-occipital membrane and into the foramen magnum, passes the vertebral artery. The V.A supplies the brain with blood. If there’s instability such as severe hypermobility with regards to rotation, this may strain or occlude the vertebral artery (Bow hunter’s syndrome), leading to symptoms such as confusion, migraine, headaches, blurred vision, lack of concentration, etc. In extreme and rare cases, this may rupture the vertebral artery, causing stroke and even death. Occlusion of the vertebral artery, be it from TOS or the atlas joints, may also cause migraines.
A pathognomonic finding of BHS is the improvement of symptoms when the patient is in a neutral position, even after he claims to have dizziness or blackout when he turns his head to one side. When BHS is suspicious, considerable authors used digital subtraction angiography as the diagnostic modality1). In our cases, clinical symptoms were aggravated when patients turned their head to one side; symptoms were improved when the patients’ heads returned to a neutral position. Prior otolaryngological evaluations were unremarkable. – Go et al., 2013
Leftward head rotations in a patient with a rotational vertebral artery occlusion syndrome elicited recurrent uniform attacks of severe rotatory vertigo and tinnitus in the right ear. These attacks were accompanied by a mixed clockwise torsional downbeat nystagmus with a horizontal component toward the right. – Strupp et al., 2000
In our series, symptoms of vertebrobasilar insufficiency were reproducible with rotational head movement. Compression of the vertebral artery was demonstrated angiographically. The correct site of occlusion of the vertebral artery was apparent only by dynamic angiography with progressive head rotation. All of the patients presented in the illustrative cases had occlusion at the C2 level; however, one patient had been previously misdiagnosed and another had an additional site of occlusion. The anatomic course of the vertebral artery is described in addition to the sites of rotational occlusion. Rotational vertebral occlusion is an important cause of vertebrobasilar symptoms, which may lead to permanent neurological deficit if left undiagnosed. Dynamic angiography is the established method of diagnosis. Great care must be taken to avoid misdiagnosing the site of occlusion or missing a second occlusive site. For this reason, it is crucial to have a thorough understanding of the anatomic course of the vertebral artery and the muscular and tendinous insertions, which may cause rotational occlusion. – Kuether et al., 1997
A 41-year-old male developed dizziness and light-headedness during chiropractic manipulation when his head was turned to the extreme right position. Computed tomography angiography (CTA) of the neck and selective digital subtraction angiography (DSA) of the vertebral arteries revealed that when the patient turned his head to the extreme right position the dominant right vertebral artery was compressed between the posterior aspect of the thyroid cartilage and anterior aspect of the right transverse process of C6 resulting in focal stenosis, while the left vertebral artery is severely compressed with significant flow limitation at the level of C1-2. – Dabus et al., 2008
What is known is that the greatest mechanical stress affecting the contralateral artery occurs at a position of cervical rotation and extension. Furthermore, if this position is sustained, the arterial flow takes longer to return to normal.32 In addition to the C1–2 portion, the VA is vulnerable to compression in the portion that courses through the transverse foramen from C6 to C1. Because of its fixation to the spine in this segment, subluxations of one vertebral body on another may exert undue tension and traction on the artery. Positions of the cervical spine can cause compression of the VA.19,33 Rotation–extension–traction appears to be the most stressful, followed by rotation–extension, rotation alone, side flexion alone, extension alone, and then flexion.19,33,34 – Dutton’s orthopaedic examination evaluation & intervention, 4e, 2016
Fig. 25
Migraine
There are three, perhaps four major ways that altas misalignment can contribute to migraines.
- Compressing the internal jugular vein
- Pulling on the vertebral artery
- Pseudomigraines caused by weakness of the suboccipitals
- Theoretically, extreme atlantal torsions may also compress the internal carotid artery
Read more about migraines in my migraine article. The above points are also connected to other dysfunctions that are described more in detail both above and below.
The jugular foramen and carotid canal
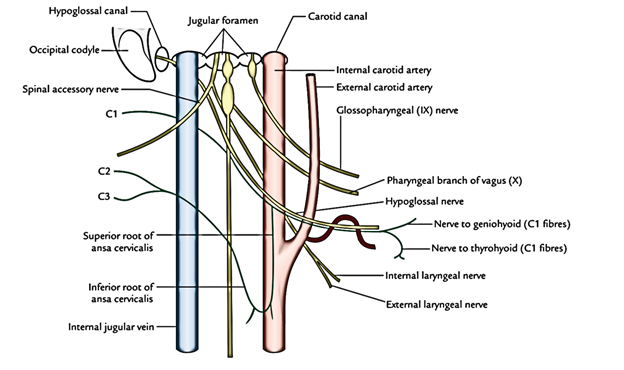
Right in front of the atlas vertebrae’s transverse process emerges the neurovascular bundle coming out of the jugular foramen, carotid canal and hypoglossal canal. As seen in the illustration below, these are the internal jugular vein, internal carotid artery, hypoglossal nerve, vagus nerve, accessory nerve and glossopharyngeal nerve. These nerves are all controlling many autonomic processes, and these may be disturbed if they become compressed, causing varying degrees of dysautonomia. They may of course also cause pain, tingling and similar common indications of somatic nervous irritation. If the transverse process of the atlas vertebrae comes forward, it may compress these structures to varying degrees between itself and. the styloid process. The CN 9-12 transmit between the TP and SP in about 66% of the population (Kim et al., 2014).
Anything related to autonomic nerve dysfunction is a massive rabbit hole. I’ve written about this in my TOS and lumbar plexus compression syndrome (LPCS) articles as well. It is almost impossible to list or even estimate all of the potential consequences in some of these circumstances, especially if a whole plexus is affected as with TOS and LPCS. Although there’s no plexus entrapment with regards to compression of the emerging structures from the jugular foramen, the vagus nerve does innervate most of the body’s organs, and it is therefore difficult to realistically estimate the level of possible dysfunction.
Fig. 26
The vagus nerve controls the cough reflex. It also opens and closes the eustachian tube by controlling the salpingopharyngeus and levator veli palatini muscles. It is not uncommon that irritation of the vagus nerve can lead to ‘clogged’ ears, tinnitus, and chronic cough. Many of these patients also have bowel issues, and considering the fact that the vagus nerve stimulates secretion of hydrochloric acid and digestive enzymes, a lack of such will likely cause maldigestion and gut issues.
Moreover it is commonly known that the vagus nerve slows the heart rate. Now, I am not saying that this is always an issue, but it is definitely an association that I’ve noticed in several patients with vagus nerve entrapment. I truly do not know how many problems this *could* *realistically* cause, but I am discovering new and interesting things all the time. I have seen some unthinkable things happen with regards to lumbar plexus compression syndrome, such as atrial fibrillation both caused and resolved, prostate dysfunction (involuntary seminal discharge), urinary inconsistency and so on. Autonomic entrapment issues caused by muscles and/or atlas misalignment is more or less an uncharted area, but I prefer to tell you what I have discovered, not because I have all the answers, but to create awareness and interest in these somewhat mysterious and generally rarely spoken of topics.
The accessory nerve originates from the C1-6 levels of the spinal cord. It then separates into two divisions, the spinal and cranial divisions. The spinal division exit via the jugular foramen, pierces the sternocleidomastoid muscle before it ventures into the dorsum, between the levator scapulae and trapezius muscles. Posterior to the sternocleidomastoid muscle, it also anastomosis (connect) with the cervical plexus. Accessory nerve pain may be generated along its path if there is entrapment within the myofascial structures, or at the craniocervical level.
Fig. x
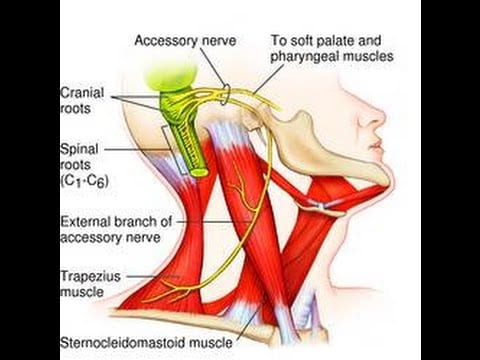
Fig. x
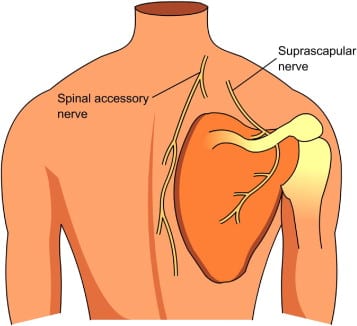
Further, it controls the sternocleidomastoid and trapezius muscles. These are often affected in dystonia patients. Could the atlas be the cause? I don’t know, but it’s plausible. For your information, Dr. Anthony Sims DDS (et al., 2007, 2009) claims that continuous noxious input into a nerve may cause such symptoms, especially with regards to TMD and the trigeminal nerve. I have also talked to patients whose pulling sensation have ceased temporarily after getting certain atlas adjustments (not my treatment).
The hypoglossal nerve controls the movements of the tongue. Additionally, it supplies movements including clearing the mouth of saliva and other autonomic activities. The hypoglossal nucleus also interacts with the reticular formation, which amongst other things suboconsciouly affect speech and articulation. There could be a relation between this nerve’s dysfunction and tourette’s syndrome (Sims & Stack, 2007).
The glossopharyngeal nerve interacts with several structures as well, such as the tongue, tonsils, parotid gland and the trigeminothalamic tract. It is also forms a part of the pharyngeal plexus along with the vagus nerve. Disturbances within all of these regions may thus potentially occur if the glossophargyneal nerve is irritated, such as salivary production, taste, tonsilar hypersensitivity. Perhaps most interestingly, interaction and dysregulation via the trigeminothalamic tract may cause disturbances in perceived touch, temperature, and pain, which are relatively common symptoms in many chronic sufferers.
If you have a look at the illustration below, it is obvious that these important structures are lying very close to the atlas and its transverse process. Now, in a perfect world, the atlas should not move significantly on the occiput, and thus it would never get a chance to jam into either of the neurovascular bundles. Sadly, though, this may definitely occur. Furthermore, they emerge between the rectus capitis anterior & longus capitis muscles posteriorly, and the alar fascia anteriorly, the first-mentioned both of which prevent prevent posterior occipital gliding, A-O torsions, and also protect the neurovascular bundle from rubbing against the atlas’ transverse process and anterior vertebral body.
Fig. x
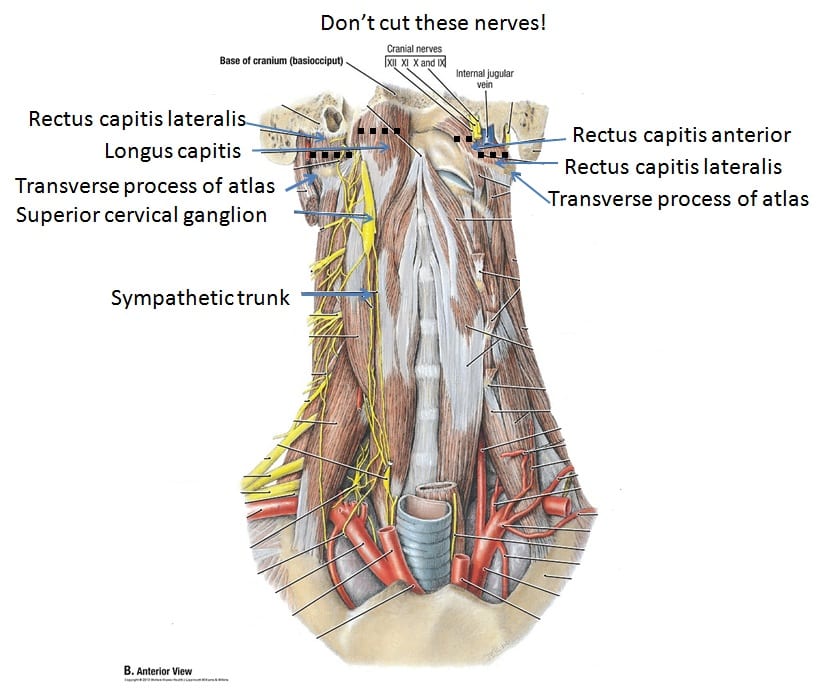
This is also why it is important to at least evaluate the atlas joint when treating patients with migraines for instance, as the jugular venous outlet or even carotid inlet may be occluded by the atlas vertebrae. This is a scary thought indeed, and some may claim it to be impossible, but I have seen some scary cases with tremendous A-O misalignments in my clinic. We should both consider and understand, that years upon years of faulty movement patterns (such as severe cervical hinging) will cause laxity and lead to joint movements that were never supposed to happen. Of course, to varying degrees once again. I have seen patients who have been whiplash injured whose atlas was lax, but A-O joint relatively well positioned, and I have seen the dead opposite. Don’t assume anything until a proper examination has been conducted.
Fig. 27 – 3: Vagus nerve, 4: IJV, 5: ICA
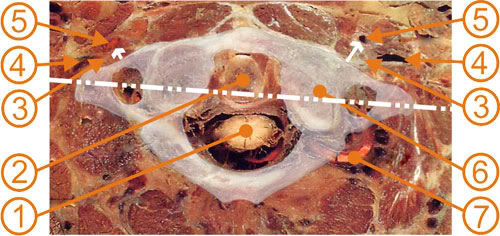
Temporomandibular joint compression
Atlas misalignment can [mildly] contribute to TMD. It’s not a large factor. I do consider the opposite relationship, i.e jaw influencing the atlas joint as a more important factor, but when the head tilts to one side, be it due to occlusal issues or atlas misalignment (e.g due to whiplash injury or longstanding cervical dysfunction), the mandible tends to shift to that side.
When the mandible shifts to one side, the shearing forces within the ipsilateral TMJ will be greater. 1-2 millimeters of lessened space between the mandibular condyle and the TMJ’s glenoid fossa may be enough to trigger shearing within the joint and eventually wear it down over time. This may also compress the trigeminal nerve, and cause a lot of difficulties.
Fig. 28
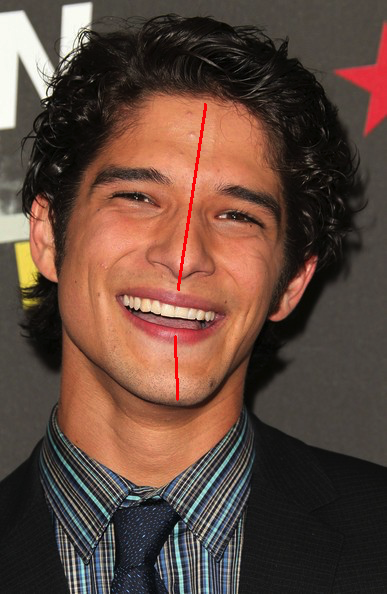
The actor in the picture above has probably had malocclusion since a young age and thus the cranial bones have not developed symmetrically. It’s not expected to see such a great cranial dysmorphia if the atlas alone is the underlying factor, unless, perhaps, it happened at a very young age. Either way it does nicely illustrate how the jaw follows cranial tilt, which is why many get more symptoms on one side. A droopy eyelid will usually also occur on the higher eye, i.e the opposite eye of cranial tilt’s direction.
Another factor that I also mentioned above, is that many patients clench their suprahyoidal muscles in a subconscious attempt to force neck stability. The suprahyoid muscle complex promotes posterior translation of the mandible, and may thus increase shearing forces in the temporomandibular joints.
Fig. 29
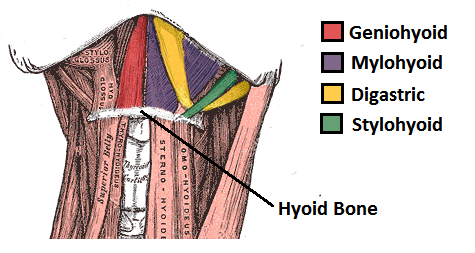
Trigeminal nerve dysfunction
I have covered this in my TMD article, but I’ll briefly address the trigeminal nerve. The trigeminal nerve is the largest cranial nerve, also known as cranial nerve V, or 5. It has three main branches, the ophthalamic (V1), maxillary (V2) and mandibular (V3) branches.
Fig. x
The trigeminal nerve is often affected in patients who have TMD and underdeveloped upper jaws. Its auriculotemporal branch can be compressed between the mandibular condyle when it’s resting too far back, which is, as I mentioned earlier, a very typical occurrence for TMD sufferers. Furthermore, some of its branches, such as the buccal and and lingual nerves, pass through the lateral pterygoid muscles which are also commonly found to be extremely weak in TMD population.
Because it has both autonomic as well as motor and sensory nervous functions, and connects to most cranial ganglia, a lot of diffuse problems may arise when it is affected. Involuntary tear secretions, facial, palatal and tooth numbness, toothaches, tremendous stabbing headaches in the temple and facial region (trigeminal neuralgia), eye pain, salivary gland pain and even swelling, tinnitus (as it controls the tensor tympani and tensor veli palatini muscles, which again control sound modulation and the eustachian tube within the ear), and so on. It also has sensory innervation of the cranial vessels, and research has shown an association between it, and migraines.
Fig. x
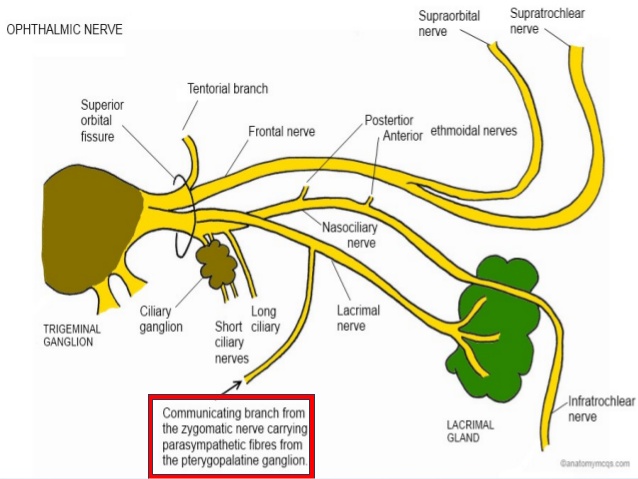
Once again, read more about this topic and its respective treatment strategy in my temporomandibular joint disorder (TMD) article. However, in short, we want to get the mandible forward in posture as well as retrain the pattern in which the mouth opens and closes. The mouth should open with protraction, not retraction, as this is very detrimental and increases shear forces within the joint and thus also the degree of compression and noxous input imposed on the auriculotemporal nerve. Furthermore, it is beneficial to strengthen the pterygoids, as they both help to bring the jaw forward, in opening it properly (without retraction), and relieve tension on the buccal and lingual nerves.
Posture
When the head moves, the body will move. It is a well known anecdotal ‘fact’ that when the head either rotates or tilts in one direction, the whole body will zig-zag in compensation in order to get the cranium back into equilibrium and the eyes levelled.
Commonly, if the head tilts to one side, the neck will rotate contralaterally. The body zig-zags all the way down, where one shoulder is up and one down, similarly with the pelvis, and one femur will be externally rotated where the other internally rotated. These are not rules, but common occurrences and observations I have made.
Fig. x
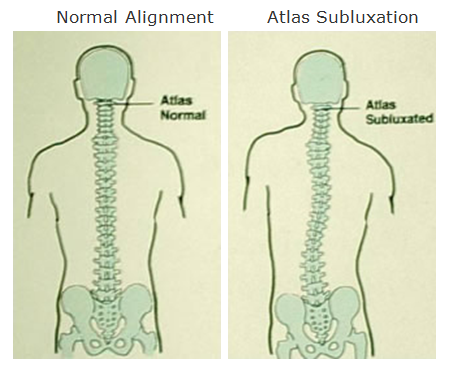
Now, this is where I somewhat disagree with many others. I disagree that minor discrepancies should be always considered as pathology. I also disagree that atlas correctives will resolve all of the body’s compensatory patterns; they will usually require to be addressed individually, especially if the issue has been long standing.
It is common to have some asymmetry. Sometimes the perceived “misalignment” may even be bone (osseous) anomalies, and not at all misalignment! Thus, use discernment and common sense while evaluating and treating asymmetries. It is also my impression that many chase extreme detail with regards to minor issues, such as a minor hip height difference, leg length, or femoral rotation. Although sometimes important, it seems to me that more important principles are often neglected in this process, especially in the sagittal plane, such as ignoring proper pelvic extension, removing the cervical hinge and so on; things that are of much greater importance. Working on minor issues while neglecting or being oblivious to more major problems, will not yield optimal results, in my experience.
Moreover, my experience is that when the neck is not hinging, the pelvis is extending and the patient isn’t slouching with their shoulders, the body will be able to handle quite a bit of asymmetry just fine. You don’t need perfect symmetry to be healthy (does perfect symmetry even exist?). That said, a top athlete may have a much greater requirement for symmetry and ‘flawless’ function than someone that goes to the gym twice per week, for instance. Honestly, I rarely treat minor discrepancies in patients who aren’t high level athletes, unless they specifically want me to (i.e because it’s important to them to fix it).
And, when we correct the atlas, these compensations have often been present for so long that they will not resolve by mere cervical correction, without also being targeted with specific individual exercises. A weak hip for example, won’t miraculously resolve by aligning the atlas. It will require rehabilitation just like the atlas, shoulders and neck will. Any significant weak point will cause compensation and thus alter structural alignment. It is important to address both the symptoms (e.g significant hip weakness) and the main causes (habits, atlas, jaw, etc).
I have seen a lot of patients that have received so-called postural corrective “cures”, both by dentists and atlas correction practitioners. Yet when I examine them, their posture is still way off, they’re still in pain, and muscles have not adapted to any corrective what so ever. I do think that most of these practitioners believe in their approaches and that they genuinely want to help their patients, but I also think it’s very naive to believe that a single correction to one joint (be it the jaw or the atlas) will resolve all of the body’s problems. I hope I have made it clear in this article how deep these problems really go, and that they must be, in my opinion, individually addressed for optimal results.
Chiari malformation (tonsillar descent)
Posterior occipital gliding may lead to cerebral herniation, i.e cerebral chiari, in severe cases. This is a condition where the cerebrum is herniated out of the foramen magnum and into the spinal canal. Statistical research have shown that neck injured population such as those who have gotten whiplash, are of much greater risk of cerebral herniation. I strongly believe that this is the case, because the distance between the posterior brain stem and the foramen magnum becomes greater as the occiput glides backwards on the atlas vertebrae, increasing risk of caudal cerebral herniation.
Chiari malformation is defined as herniation of the cerebellar tonsils through the foramen magnum, also known as cerebellar tonsillar ectopia (CTE). CTE may become symptomatic following whiplash trauma. The purpose of the present study was to assess the frequency of CTE in traumatic vs non-traumatic populations.
Cervical MRI scans for 1200 neck pain patients were reviewed; 600 trauma (cases) and 600 non-trauma (controls). Half of the groups were scanned in a recumbent position and half were scanned in an upright position. Two radiologists interpreted the scans for the level of the cerebellar tonsils.
A total of 1195 of 1200 scans were read. CTE was found in 5.7% and 5.3% in the recumbent and upright non-trauma groups vs 9.8% and 23.3% in the recumbent and upright trauma groups (p = 0.0001). – Freeman et al., 2010
Atlanto-occipital misplacement also causes jugular vein compression, which in turn causes brain swelling. This swelling, usually subtle volume increase of the brain, results in narrowing of the ventricles, the CSF cisterns, and may also push the cerebellar tonsils downward into the foramen magnum. The renowned neurosurgeon Atul Goel found that reestablishing craniocervical stability in this patient group may reverse the cerebellar descent. Because his technique also frees the jugular vein, I think that reduction in brain swelling is also a large contributing factor to this phenomenon.
Fig. 30
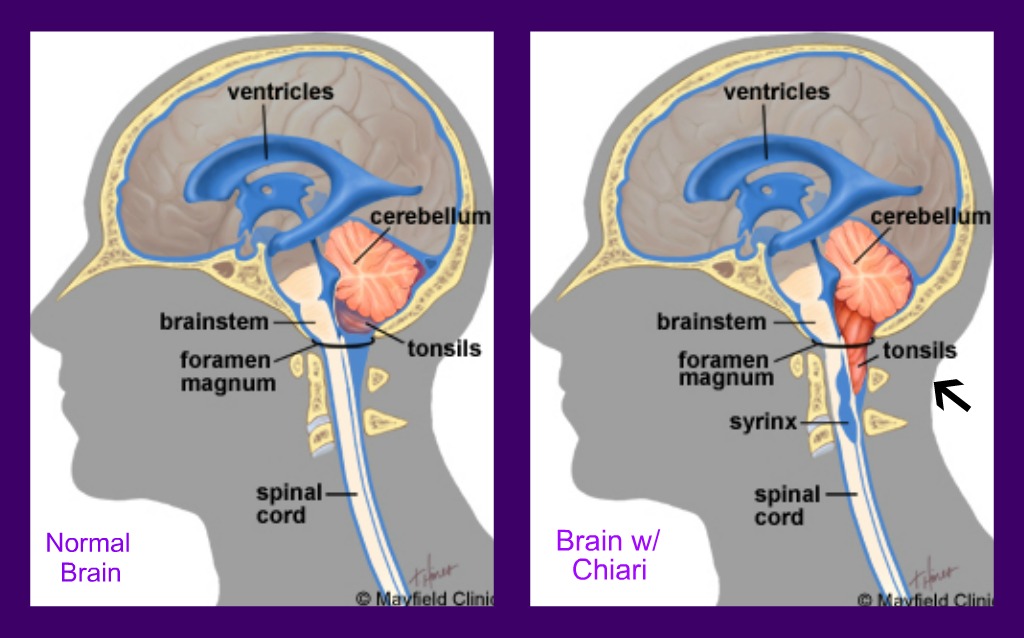
Proper atlantal measurements & identification
There are many techniques today claiming to measure atlantal misalignment, but the problem is that most of these measurements look for serious pathology, and not for chronic misalignments which are more common. Therefore many will have an MRI, but be deemed ‘healthy’ although they feel that something is unmistakenly wrong.
There are some radiologists measuring atlantal torsions, but as far as I know, they are measuring for torsions and subluxations between the axis and atlas, and not between the atlas and occiput. This is in my opinion a relatively big mistake, because a torsion between the C1 and occiput is much more serious than between the atlas and axis, because the atlantoaxial joint is supposed to have a lot of movement, where as the atlanto-occipital joint is supposed to be fixed. Now, this is not to imply that a loose A-A joint is optimal; of course it is not, as I have also made clear earlier in this article. The point, however, is that the margin of error is a lot slimmer at the A-O joint than the A-A joint due to a potentially altered position of the foramen magnum in relation to the spinal canal, as well as potential compression of the neurovascular bundle emerging from the jugular foramen and carotid canal.
I have seen quite dramatic atlantoaxial torsions as well as atlanto-occipital torsions in long-standing neck pain sufferers. The torsions are sometimes so great that I dare not to touch these clients until I have a radiologist assess their cranial vessels and confirm their integrity. This is also why I am generally opposed to performing regular upper cervical manipulative techniques, as the patients who ask for this often already have upper cervical laxity, and the manipulative treatment may cause rupture of the vertebral artery, which may lead to stroke or death in worst case scenario (very, very rare, but not a chance we’d like to take if the patient’s atlas is in obvious torsion, now is it?).
Vertebral artery (VA) occlusion by rotation of the head is uncommon, but can result from mechanical compression of the artery, trauma, or atlantoaxial instability. – Tominaga et al., 2002
Fig. 31
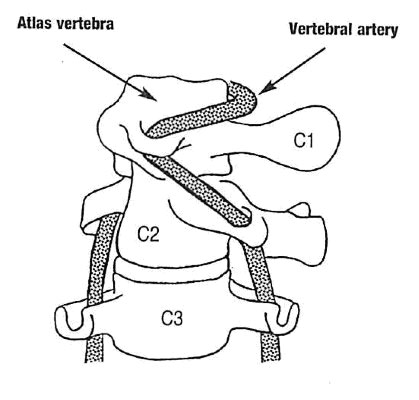
One of the reasons this occur, is that the measurements for the atlas joint that many practitioners use, do not account for atlanto-occipital torsion. Thus, a practitioner may find himself “correcting” the A-A joints, unaware that the A-O joint is extremely misaligned. This can be EXTREMELY DANGEROUS and is why I do not recommend upper cervical manipulation for anyone with possible A-O torsion.
To address this safely, one must first know how to properly measure the atlas joint. We then need to know how to palpate the landmarks, as well as some rules for positioning.
The patient must be lying flat, supine, without a hinge at the neck. Put the bench pillow at the occiput rather than mid-cervical, to prevent hinging. Improper position can and will skew the measurements.
- Measure C2 spinous process in relation to C3-4 spinous process
- Measure cranial mastoid process in relation to C1 transverse process (TVP)
- Lateral gliding can be measured by comparing the lateral edge of the mastoid process and the tip of the C1 transverse process. You are then looking for lateral occipital translation and not torsion.
- Estimate A-A alignment based on step A-O and axiocervical measurements
Fig. x – Good atlantooccipital alignment
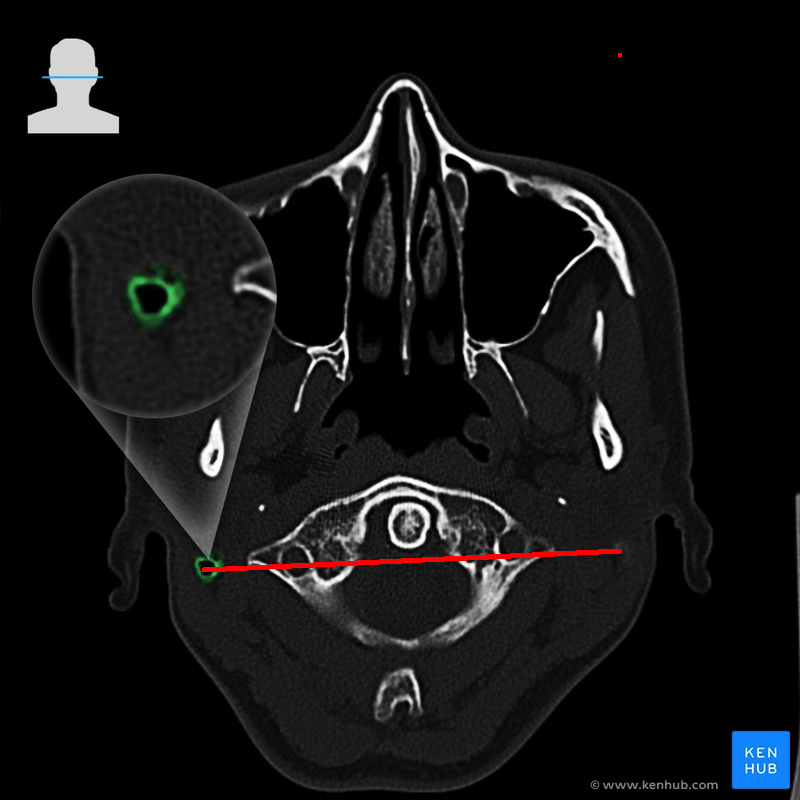
The spinous processes should be lined up, naturally. But to measure the occiput and C1, one needs to be aware that the C1’s transverse processes should be situated directly below the mastoid processes. Not behind, not in front. Sometimes I will find one transverse process far anterior to the mastoid process, and the opposite side properly lined up. This means that a facet joint subluxation has likely occurred. Other times one transverse process will be anterior to the mastoid process while the opposite side will be posterior to it. This usually implies ‘mere’ rotation.
Lateral occipital translation may be measured by comparing the distance between the lateral edge of the C1 transverse process, and the lateral edge of the mastoid process. If it’s greater on one side, the occiput may have shifted slightly to one side. We are talking millimeters here, and it’s difficult to know whether or not an osseous anomaly rather than true gliding is the cause of such a discrepancy, when the margines are so small. Use healthy judgement when assessing and treating lateral gliding.
The whole C1 may also translate forward in relation to the cranium when there’s ligamentous laxity, in which the transverse processes will be anterior to the mastoid processes on both sides, unless one is further back due to co-occurring C1 rotation. This will increase the opening of the foramen magnum posterior to the brainstem, and may in extreme circumstances it cause the cerebrum to herniate down into the spinal canal.
If the C1 transverse process is thought to be anterior to the mastoid process, make absolutely sure that you are not indeed palpating the styloid process of the skull. They may seem similar, but the difference is that the styoid process is thinner and longer, and can be tracked toward the skull, where as the transverse process is thicker and will not track superiorly. In some patients, the styloid process may be abnormally long. DO NOT mistake the styloid process for the transverse process of the atlas. If you are unsure, do not correct anything.
Manual palpation of the C1 TVP can be very accurate and likely to direct a manual therapist or other health professional to the intended diagnostic or therapeutic target. As another potentially confounding issue, craniocervical anomalies are found in 1–4% of the population. Possible anomalies include elongated mastoid processes, lateral ponticles, and ossification of the stylohyoid ligament.19–22 – Cooperstein et al., 2015
Fig. 32
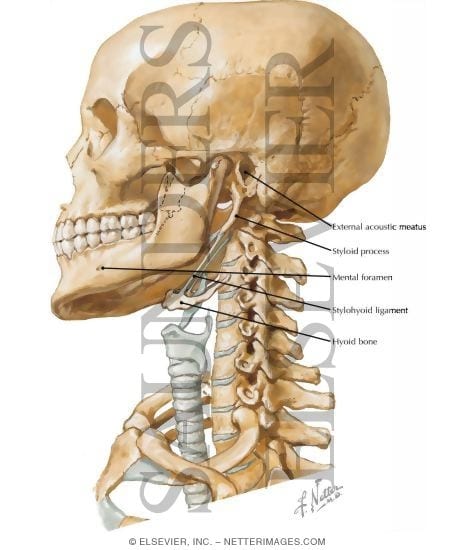
Officially, non-severe atlanto-occipital misalignments is a topic of diffusivity, as far as I am aware, as valid landmarks of measurement are not established. Therefore its milder (mild as in not a complete subluxation or dissociation, i.e serious trauma) degrees of subluxation and interpretation is an uncharted waters. I do hope, though, that this article will contribute to stopping that, and help practitioners to evaluate the A-O joints with greater accuracy and confidence. The below illustration shows degrees of atlantoaxial subluxations, especially post trauma. They are not 100% fitting what I am talking about here, but it still gets the point of mechanical behaviour and of course also the potential severity of these issues across.
Fig. 33
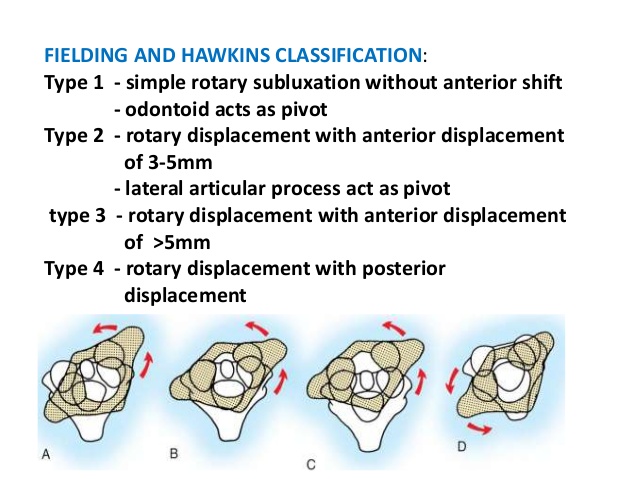
I received a patient with long standing neck pain, which occurred after a car accident years ago. She had been to visit a specialty clinic, whose radiologist was an expert of assessing atlas misalignment. She also underwent a special atlas adjustment at another clinic (I won’t mention any names, but it was done with a device and not manually) right after having the MRI, and this was all just two months prior to visiting my clinic.
I read the report before seeing this patient. The MRI report said that the A-O junction was indeed nicely aligned, but the A-A was not. Since I didn’t know how to measure the MRI by myself at the time, I trusted the expert’s measurement. It was a radiological measurement after all, so why wouldn’t I?
Let me quote the report:
At the craniocervical junction, there is good symmetry between the right and left occipito-atlantal joints.
Now, when I assessed the client in person, I was shocked. The left C1 transverse process was far anterior to the mastoid process on the left side. So far forward that I had to make the patient protract the jaw in order to find it! This, despite having both an MRI claiming its symmetry and receiving a special atlas correction, which was even followed up with an x-ray that was said to demonstrate the corrective’s success.
I went back to the MRI images to identify the landmarks and make my own measurements. Something was obviously not right. What I discovered, was that the MRI showed exactly what I observed in clinic; a significantly anterior left C1 transverse process demonstrating rightward rotation of the atlas (i.e leftward occipital rotation on the atlas, if you will).
Let’s look at the MRI. The yellow line (not drawn by me) shows A-A subluxations, which were also noted in the report. The mastoid process’ alignment is shown by the green line, where as the C1 transverse processes are indicated by the red line. The C1 has translated extremely far forward, and rotated toward the right.
How could this have been missed? …Unless it was never looked for?
Fig. 34 – Partial obstruction. of the right and complete occlusion of the left internal jugular veins
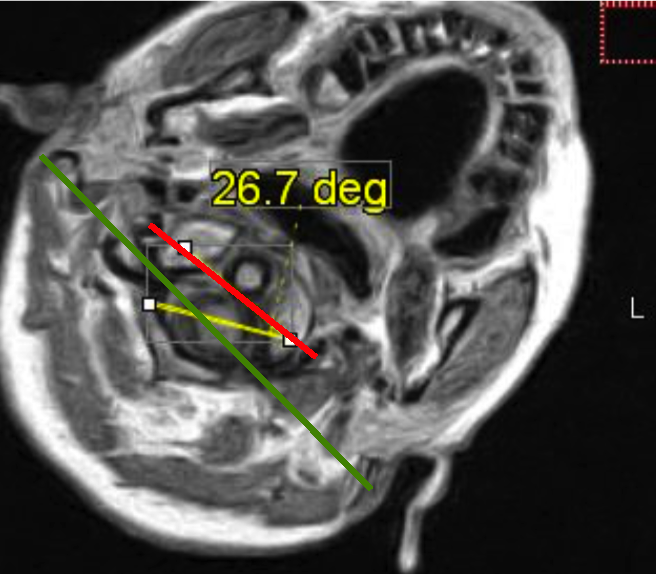
Here is another patient of mine who became disabled after severe neck trauma. As you can see, the atlas has translated forward and rotated to the left. Upon examination the patient was severely ‘hinging’ at the neck, has TOS, and many other problems.
Fig. x
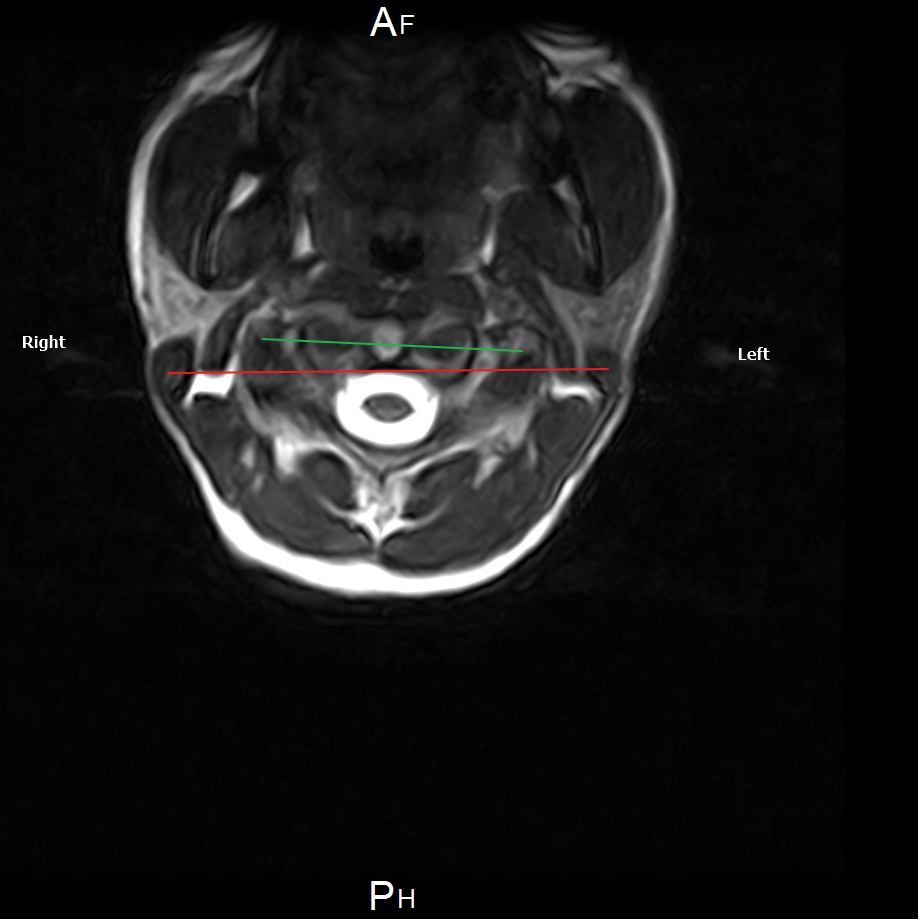
Another patient with chronic migraine and dizziness after whiplash injury. Large forward translation of the C1; 11 mm anterior to the mastoid process.
Fig. x
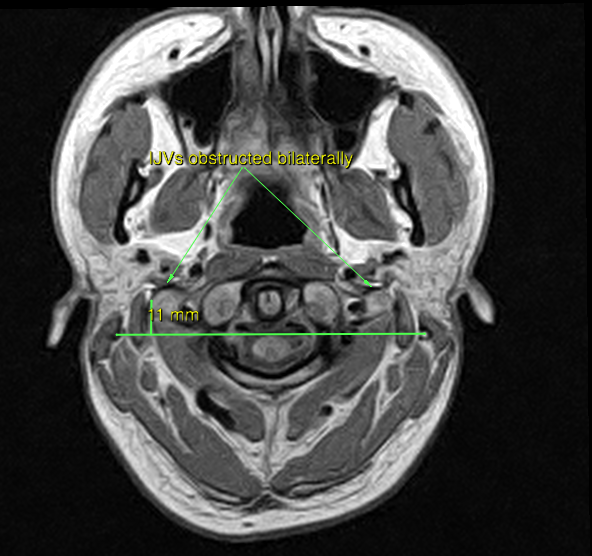
Fig. x – 6,4 mm forward subluxation of the AO facet in a patient with intracranial hypertension
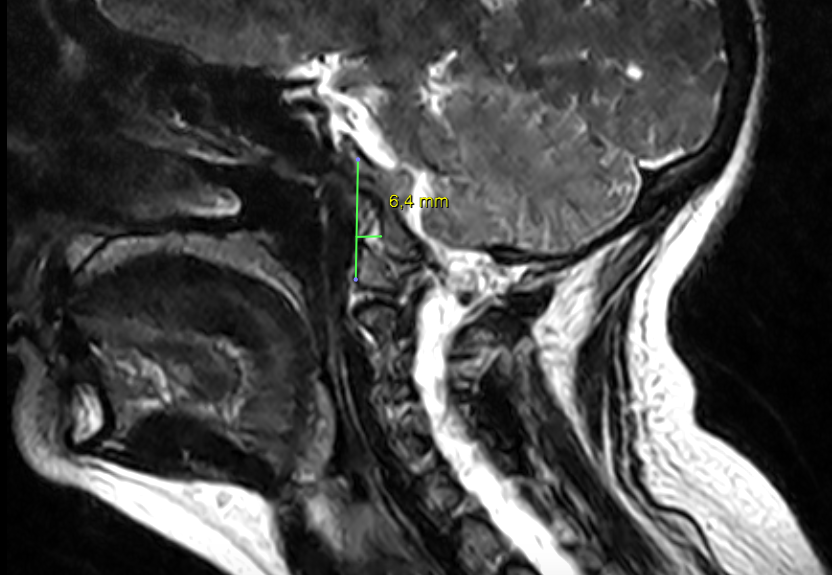
I am writing this, not to mock or bash anyone, (I sincerely believe that most health professionals do try their best to help their patients), but rather to shed light on what I perceive to be obvious lack of knowledge and measurement criteria with regards to “moderate” (i.e non-acute) torsions of the atlanto-occipital joints. If such criteria existed per this date, it is unlikely that I would be able to point out an obvious torsion that was missed by several atlas specialists.
Furthermore, and as I already mentioned, this patient was [mistakenly] assured that her atlas had been aligned, and was even showed demonstrable ‘proof’ of this in a follow-up x-ray. This, although she still had a significant, elusive atlanto-occipital torsion. So, based on the above case study and many similar cases, it is my impression that there does not exist a protocol per this date that properly measures and corrects the atlanto-occipital joint. For the very same reason I am making this article’s information available, for free.
Now that we have learned how to evaluate atlas misalignment by using certain landmarks, let us move on to the treatment section.
Treatment strategies
As implied several times by now, the approach to resolve misalignment of the atlas joint must consist of more than just the correction itself, or a mere occlusal appliance for that matter. An atlas correction will not last if the underlying cause is not addressed; hinge neck and muscular dysfunction. It is absolutely necessary to rehabilitate the muscles that stabilize the atlas joints, as well as reestablish proper craniocervical habits, i.e movement and postural patterns.
If the ligaments of the atlas have become excessively lax, i.e to the degree that vigorous rehabilitation of muscles and posture do not cause adequate stability, prolotherapy injections of the ligaments may be necessary. Of course, if there’s a full blown rupture of the ligaments holding the A-O and A-A joints together, surgery will likely be required. In circumstances like the latter, though, the patient will usually be diagnosed and get the necessary surgical intervention at any conventional ER room.
Once again, this article is focused on assessing and resolving chronic dysfunction and not acute trauma. I usually setup the corrective sequence in the following manner:
- Postural corrective
- Muscular corrective
- Movement corrective
- Hobby/work corrective
The reason posture comes first is that it’s the simpler thing to change, and is also the most detrimental and exacerbative factor when it’s dysfunctional. To support the postural changes and lay the foundation for proper movement, the muscles that stabilize the cranium and cervical spine (i.e the trio of success) will be strengthened as a daily or every-other-day routine homework. Once posture and the muscles are greatly improved, I will address the patient’s cervical movement pattern by teaching them to extend, flex and rotate the neck without compromising alignment, which more or less means to avoid cervical hinging. Cervical hinging MUST vanish if the patient is to get lasting results.
If there’s no risk of serious injury, or massive misalignment of the A-A or A-O joints, I’ll correct the atlas first by using the protocol outlined further down. If there is severe atlas misalignment, especially at the A-O junction, I may not dare to touch ut until a radiologist has cleared the vertebral artery. Even then, sometimes it’s better to let the body sort it out on its own and just starting with the postural and muscular correctives. That is, if the patient has really bad atlas misalignment. In most cases, slowly but surely things will get back to normal once important underlying factors are addressed. Either way, it will prevent things from getting worse, should there be a rare case where the atlas will not accommodate the improved structural habits and muscular functions.
After all this work I will evaluate the patient’s progress. If everything is looking good, but misalignments keep occurring (this is relatively rare), their hobby or work routines may need to be altered, or more specific homework to balance out certain structures may be necessary.
Postural correction
I have touched upon most of the these elements already, but it is crucial to understand that our postural habits greatly contribute to the atlas joint’s integrity. If the posture and habits are poor, it may compromise the atlas joints in several ways, as I’ve shown several times throughout this article. Without changing these, it will be close to impossible to resolve the cervical issues, in my experience.
Swayback posture must be addressed and corrected first, as it promotes forward head posture and shoulder slouching, which again promotes atlas misalignment and thoracic outlet syndrome, headaches, migraines, disc herniations and much more. If the patient keeps hanging backward with their chest, it will be close to impossible to correct forward head posture and scapular depression in the long term, because the body wants to regain an optimal center of gravity.
The woman in the picture below presents with a pretty common postural type in modern society. The pelvis is in posterior tilt with swayback posture, causing the low back to round (butt pointing down), and the thoracolumbar junction to hyperextend. Furthermore the hip joint hyperextends, the shoulders protract and depress, and the neck comes forward, often along with a nasty cervical hinge. Sadly many will mistake this posture for anterior pelvic tilt, and malcorrect the patient into a posture that exacerbates her symptoms. Please read my article on the myth of anterior pelvic tilt, to read some – in my opinion – damning evidence against this common malpractice and dogmatic belief.
Fig. 35

Moreover, to correct these patterns, it is ABSOLUTELY NOT enough to train the weak antagonists. Posture is a result of habits, not strength. Weakness is also a result of habits, which is why strengthening them is mere symptom-work. Symptom work is important too, don’t get me wrong, but it will not address nor correct the underlying cause(s). Treat both the cause and the symptoms, for quicker and long lasting results.
The patient has to correct his or her habits. We pull the pelvis back and up, get the chest gently forward, pull the shoulders gently up and remain long in the neck. Stay there, forever! This takes a lot of effort from the client and it’ll take a few months before it sits well, but it’s completely doable; I do it every day in clinic. In the beginning, the patient will feel tired and even like they’re in pain, and this may of course seem very contraintuitive. Keep on fighting, it’ll get better in a week or two, and as I said, normal in 2-3 months. You CAN do it, don’t let your excuses stand in the way of your healing.
Watch my video demonstration on this below.
Once the posture is good, and the ‘trio of success’ has been worked on and improved significantly, the patient will need to learn how to extend and rotate the head without falling back into the old cervical hinging pattern. I did explain this in detail as well as attach a video demonstration in the forward head posture section, and thus won’t do it again here. Review that section if you need to.
Posture, movement patterns, and muscles will need to be rehabilitated. It is hard work, but you will be repaid greatly if you do a good job. I have seen it happen time and time again, on cases deemed to be “impossible to treat”! I have resolved whiplash injured patients with more than 20 years of pain using this protocol. That’s not to brag, just to show that it can be done if the patient gets the [correct] job done. There is almost always a solution!
Now, I know that I also wrote extensively above about the relationship between dental occlusal factors and posture & muscular functions. However, it is important to emphasize, and I repeat the following FACT; we can override a guided dysfunction caused by occlusal factors by being conscious of our habits, as well as incorporating the proper corrective exercises for one’s individual dysfunction. Try and see for yourself. You are not damned to poor posture nor to having TMD just because you have malocclusion, but you will need to work a little harder to maintain a decent posture.
The muscle trio of success; re-stabilizing the atlas joints
In addition to re-establishing proper craniocervical posture and movement habits, and of course as well as correcting atlantal torsion, it is important to understand what needs to be done in order for the corrections to stick permanently. This is where the ‘trio of success’ comes in, namely the suboccipitals, longus colli and longus capitis muscles. I have explained the functions of these muscles already, in the initial sections of this article, so review those sections if you do not remember.
Most of the time, the atlas joints are ‘savable’ in terms of reestablishing stability, with very conservative measures, such as muscle and postural rehabilitation, even if it started out very misaligned. If the atlantoaxial, atlanto-occipital, and cranioaxial (such as the transverse, cruciate and alar ligaments) ligaments have become lax, a much greater responsibility will be put on the muscles to keep the joints syncronized and moving orderly. We therefore need to make sure that these muscles are working in an exceptional manner.
The longus colli and longus capitis will prevent posterior occipital gliding on the atlas, which is a very common form of misalignment in atlas misalignment sufferers, along with torsions, of course. The suboccipitals will also restrict anterior gliding of the upper cervical below the occiput, and it will syncronize and align cranial motion with atlantoaxial motion. These are key functions, and is why I refer to these muscles as the trio of success!
Accessory work
In addition to strengthening the ‘trio of success’, it is a good idea to strengthen the muscles that may restrict normal atlantoaxial and craniocervical motion. Tight muscles are virtually always weak muscles in my experience, and I’ve made many errors before coming to this conclusion, which is why I recommend strengthening rather than stretching and massaging for most of the circumstances. The scalenes, trapezius, levator scapulae (more on this one soon) are perhaps the most important ones here, but the splenius cervicis and longissimus may also be considered. The latter muscles may be strengthened by performing neck extension (no hinging!) while simultanously mildly rotating the neck ipsilaterally.
The trapezius may be strengthened by elevating the shoulders vertically. I did post exercise videos for the scalenes further up, but please be careful when starting these exercises as they may trigger tremendous symptoms initially, if performed too intensively, too early.
How manually correct atlas misalignments
We can correct torsions of the A-O joint by tractioning the levator scapulae muscle. Lateral gliding can be resolved by tractioning the rectus capitis lateralis muscle. Forward gliding is theoretically possible by pushing the patient’s head forward while they maintain an anteriorly rotated scapular position, to engage the levator scapulae bilaterally, but I’ve never tried it.
With regards to correcting and tractioning the A-O joint, one needs to understand that we do not play around with the bones that hold the cranium. Maltreatment of this region can, in utterly worst case scenarios, cause serious injury such as stroke and death. It is not a simple “pop” and we’re back in action. Such a pop could potentially dissect the vertebral artery and be fatal. Patients must NEVER play around with atlas corrections, and qualified practitioners must use a high level of caution.
Vertebral artery dissection in a patient practicing self-manipulation of the neck
A 42-year-old female patient sought care for left shoulder pain with a secondary complaint of left lower neck pain. Twelve days prior, she had had “the worst headache of her life,” which began in her left lower cervical spine and extended to her left temporal region. The pain was sudden and severe, was described as sharp and burning, and lasted 3 hours. She reported nausea, vomiting, and blurred vision.
Initial history and examination suggested that the patient’s head and neck pain was not musculoskeletal in origin, but vascular. She repeatedly requested that an adjustment be performed, but instead was referred to the local emergency department for further evaluation. Magnetic resonance angiogram revealed a dissection of the left vertebral artery from C6 to the C2-C3 interspace and a 3-mm dissecting pseudoaneurysm at the C3 level. She underwent stent-assisted percutaneous transluminal angioplasty combined with antiplatelet therapy (clopidogrel) and experienced a good outcome. – Mosby & Duray, 2011
Thus also a qualified practitioner must use the absolute fullest caution when attempting to treat these joints. It can be corrected relatively safely by pulling on the levator scapulae muscle, as it attaches to the C1 transverse process and may thus pull it posteriorly, as a sort of muscle energy technique, rather than twisting on the head, which pulls on the [unstable] joint itself, as it is done conventionally.
Lateral movements may be controlled by pulling on, or strengthening the rectus capitis lateralis. The rectus capitis lateralis will pull the C1 ipsilaterally, and the occiput contralaterally. So if you find the distance between the edge of the C1 transverse process and the edge of the mastoid process to be greater on the left side, that means that you may need to work the rectus capitis lateralis on that same side. As I said though, I consider NOTHING completely safe if the patient has massive torsion of the A-O joint. If manipulation is out of the question, strengthening the levator scapulae on the side that has an anterior transverse process, as well as the deep neck flexors and suboccipitals, will promote adjustment and realignment between the occiput, atlas and axis. The recuts capitis lateralis may also be strengthened bilaterally, just make sure to recheck coronal alignment afterwards.
Now to be fair and reasonable, I have seen some really banged up patients (with severe A-O torsion) who have been receiving conventional upper cervical ‘adjustment’ (therapist was of course oblivious to the massive A-O torsion, it was not identified and not treated) for up to four years, and is still alive. The body can handle a lot of beating. But, do you really want to test those limits? Take those chances? Of course not. I think that if the therapist in question knew how misaligned the in question A-O was, he would wet his pants. Ignorance can indeed be very dangerous. There are reports of patients dying from stroke after routine adjustments, but thankfully these are very rare and few.
I am, and I reiterate, not writing this to bash anyone. I really do believe that we all do the best that we can. Knowledge is key, however, and the current protocols for atlas measurement as well as corrections are not adequate. I hope that this has been made reasonably clear so far – A paradigm shift is needed so that awareness and knowledge related to both measurement and correction of the atlanto-occipital joint can spread out to the [qualified] masses.
Using the levator scapulae as a lever of traction
The side that the transverse process is identified to be anterior to the mastoid process on, is also the side you’ll also want to exercise the levator scapulae on. You can also traction it to immediately alter atlantal alignment, by having the patient gently raising and protracting their shoulder (to engage the L.S.), and then the practitioner simultaneously pushes the head diagonally forward to the opposite site while twisting it contralaterally. It is a static pull and no significant movement should occur, hence you’re just “pulling” the levator scapulae and using it to twist the atlas back.
Fig. 36
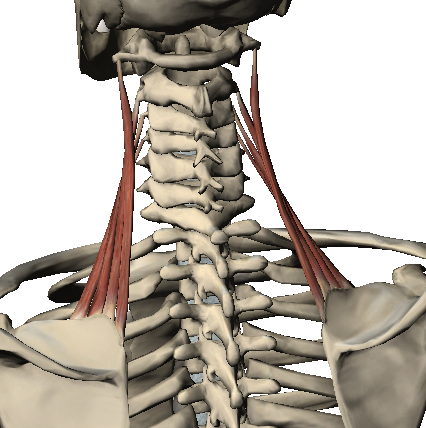
So, if the C1 transverse process is forward on the right side for example, the right shoulder is slightly elevated and protracted (by the patient), the head is pushed forward to the left while simultaneously rotating it toward the left (by the practitioner). The patient, of course, tries to resist your pulling (it should be a static hold, NOT a movement, and excessive force is NOT used). Repalpate the transverse process after correction and see whether or not it has come backward. Also palpate the opposite side; it should have come forward, unless there is a facet joint subluxation.
If there is a torsion between the atlas and axis, e.g atlas rotated to the left and axis to the right, it may be necessary to traction both of the levators in order to pull both back into position, but always correct the A-O joint first. Needless to say, you do not attempt the above if you don’t understand what you are reading, and also, naturally, if you are not qualified. Only perform this traction if you understand the protocol, you’re qualified, and are absolutely certain of what you’re doing.
Be aware though, that this should only be done if there is a light misalignment. If there is severe misalignment, ALWAYS refer the patient out to a radiologist first to take ultrasound of the cervical vessels, to ensure that you absolutely do not risk injuring the patient. You do NOT KNOW whether or not any of those vessels are compromised before you start working on their neck. The outlined protocol for correction in this article is quite safe, as it’s a muscular traction and not a pull on the joint’s ligaments. However, the vertebral artery can rupture upon mere sneezing, in patients who are greatly predisposed to injury (“the last drop”), and you really do not want your treatment to be that last drop. Get the patient checked out first, if it looks bad.
What about the vertebral artery dissection test, you may ask? The vertebral artery dissection test has been shown not be specific enough to reliably detect wearing of the vessel. It is a relatively reliable test once the damage is already done, but not to test general integrity of the vertebral artery. This is why a negative VAD test is simply not a sufficient confirmation of vertebral artery integrity, to go on with corrective procedures. Once again, this only applies if there are obvious severe misalignments of the atlas; not to minor ones. Or, of course, if symptoms of VAD are present. Beware though that TOS and VAD may both share some symptoms of vertebrobasilar insufficiency, and because the scalenes stretch during the VAD test, it may possible also cause similar symptoms and thus mimic a positive test.
Levator scapulae exercise
Prolotherapy
Most of the time, great results can be achieved with musculoskeletal rehabilitation, when it’s done right. And surgical or prolotherapeutic internventions will only address a specific injury, but not the whole system. Therefore it’s paramount to understand that these latter interventions, although sometimes mandated, do not substitute proper musculoskeletal rehabilitation. As I said, though, there may be times where the cervical ligaments are extremely stretched, so stretched that muscular and postural rehabilitation alone won’t be enough to adequately normalize jointal articulation and stability. In such cases, prolotherapy may be a relatively conservative and low-risk supplemental treatment option.
Some consider prolotherapy to be conservative treatment (it definitely is compared to surgery), others do not. I guess the truth lies somewhere in between, but who cares about formalities anyway. Prolotherapy has been shown to be an effective intervention against ligamentous laxity. It involves injecting a serum of dextrose into the ligaments, which will cause the ligament to inflame and then contract, restoring it to a better (shorter) length and thus increasing its stabilizing potential and function.
Especially post trauma, but also in relation to long standing cervical dysfunction, the transverse (a part of the cruciform) and alar ligaments of the atlas joints may lengthen or even rupture. Laxity of the atlantoaxial and atlanto-occipital capsules may also occur over time, if there is movement dysfunction.
Because most prolo-practitioners are afraid of hurting neck injured patients, they dare not to inject their neck, even when it’s ultrasound guided. I think a “the last drop” mentality is the cause of this, as they perceive such clients as fragile, which I can understand to some degree, because they often are fragile. In Europe it’s hard to find therapists who will inject the upper cervical. I do know that several American clinics do so, though.
Moreover, there is a clinic in the states that injects the deep alar and transverse atlantal ligaments. The prolotherapeutic injection is inserted through the articular gap located between the odontoid process and the articular facet joints. Very cool and pioneering work, in my opinion! The clinic is called Regenexx, and you can watch a video of this procedure in the link below the underlying pictures.
Fig. 37
Fig. 38
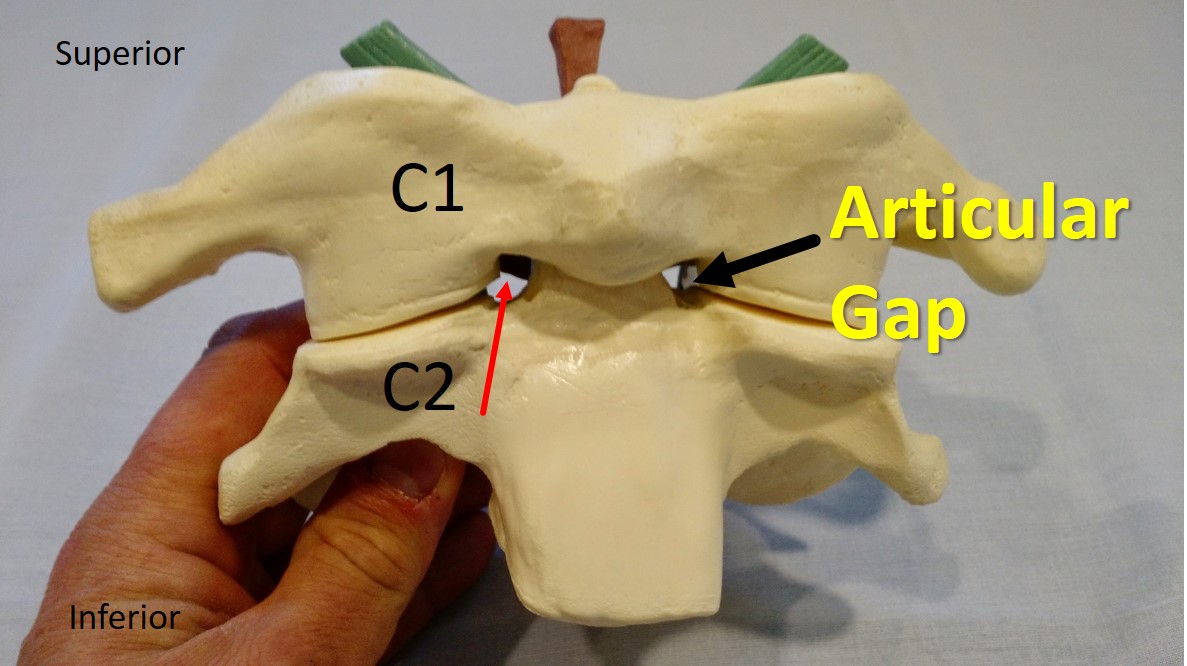
In patients with symptomatic anterior cruciate ligament laxity, intermittent dextrose injection resulted in clinically and statistically significant improvement in ACL laxity, pain, swelling, and knee range of motion. – Reeves et al., 2003
Prolotherapy injection with 10% dextrose resulted in clinically and statistically significant improvements in knee osteoarthritis. Preliminary blinded radiographic readings (1-year films, with 3-year total follow-up period planned) demonstrated improvement in several measures of osteoarthritis severity. ACL laxity, when present in these osteoarthritic patients, improved. – Reeves et al., 2000
Use of dextrose prolotherapy is supported for treatment of tendinopathies, knee and finger joint OA, and spinal/pelvic pain due to ligament dysfunction. – Hauser et al., 2016
Relaxation of ligaments and tendons occurs when fibers do not regain their normal tensile strength after having been sprained or torn. This condition causes more chronic whiplash and low back pain, more referred pain and more sciatica than does any other entity. Diagnosis may be confirmed by intraligamentous injection of a local anesthetic solution. An incompetent structure may be rehabilitated by intraligamentous injection of a proliferating solution which stimulates the production both of new bone and of fibrous tissue cells. Hacket et al., 1960
Summary
My goal for this article was to include all of the necessary material needed to assess and addresss the atlas joints. It is a truly a multifactorial problem, mandating a mutlifactorial approach in order to resolve the problem for good. Forward head posture and neck hinging is perhaps the most common denominator that contributes to and exacerbates atlas misalignments, as it will cause utter loss of tensegrity within the whole cervical complex.
I have yet to see a single whiplash or long-standing neck pain patient whose neck is not massively hinging. Neck hinging will, in addition to causing loss of tensegrity and massive muscular dysfunction, also restrict normal axial movement of the upper cervical, and may thus cause hypermobility and improper vertebral gliding within the joints.
Atlas joint misalignment is often associated with thoracic outlet syndrome, disc herniations, headaches, migraines, vertigo, TMD, and so on. Some of these are direct causes of atlas misalignment, others are not. The treatment approaches suggested in this article will, however, address both direct and most of the indirect associations of atlas misalignment.
I reiterate; the underlying causes of atlas misalignment must be addressed if one wishes to have lasting results. Cervical posture need to be optimized and hinging must be vanquished. The ‘trio of success’, namely the longus capitis, longus colli and suboccipitals will all require significant strengthening, as they are perhaps the most important stabilizers of the atlas joints. They prevent neck hinging, forward atlantal gliding, posterior occipital gliding, and syncronizes A-A and A-O joint movements. It is absolutely not a sufficient therapeutic measure to merely manipulate the atlantoaxial joint; it won’t deal with the real problem what so ever.
The atlanto-occipital joint is one poorly understood and vastly neglected. Many claim to address and correct the atlas joints, yet do not measure this joint at all, because no official measurement criteria exists. Most atlas joint ‘correctives’ today focus on the atlantoaxial joint. In this article, I propose a very easily palpable approach to measure these joints, by using the following rules and landmarks:
- C1 transverse process situated beneath mastoid process
- C2 spinous process in line with C3-5 spinous processes
By measuring the atlanto-occipital junction we can detect A-O torsions and improper glidings, both anterior/posterior and lateral. The A-A junction is estimated, not measured. The C2 is measured in relation to the cervical spinous processes. Once you have measured both the A-O and axiocervical landmarks, it’s easy to estimate whether or not there is also an A-A torsion.
Both atlanto-occipital and atlantoaxial torsion may be corrected by a traction maneuver with the levator scapulae muscle, whose muscle fibers attach to the C1-C4 transverse processes. But, if the correction is to last, the trio of success must be worked out, and posture as well as movement habits must be optimized. A non-qualified practitioner or even patient should and must never attempt to traction the levator scapulae.
A torsion at the A-O joint is much more serious than an A-A torsion, and because it’s virtually always missed (unless there’s severe trauma and subluxation), many will be oblivious to such factors. The main reason the A-O is more important, is that this joint is not supposed to move much with regards to rotation nor gliding, where as the A-A joint has great innate rotational capabilities, and is thus less critical to be out of alignment. It is of course not optimal, especially with regards to the vertebral artery, but less critical.
And, I feel the need to repeat, once again, that it is not my intention to bash on anyone. But because proper information on this topic is so tremendously important, I feel the urgency to reveal these things. This is all, of course, in my opinion and in my experience. My word is of course not God’s word, and I am not expecting everyone to agree with me either. Use your own discernment and make of it what you will.
I do hope that this article has shed light on this greatly important, yet controversial topic, and that many will read it and incorporate these measurements into their clinical practice.
References
- Kulkarni V, Chandy MJ, Babu KS. Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurol India. 2001 Dec;49(4):355-9. PMID: 11799407.
- Liu JX, Thornell LE, Pedrosa-Domellöf F. Muscle spindles in the deep muscles of the human neck: a morphological and immunocytochemical study. J Histochem Cytochem. 2003 Feb;51(2):175-86. doi: 10.1177/002215540305100206. PMID: 12533526.
- Kristjansson E. Reliability of ultrasonography for the cervical multifidus muscle in asymptomatic and symptomatic subjects. Man Ther. 2004 May;9(2):83-8. doi: 10.1016/S1356-689X(03)00059-6. PMID: 15040967.
- Andary MT, Hallgren R, Greenman PF, et al. Neurogenic atrophy of suboccipital muscles after a cervical injury: a case study. Am J Phys Med Rehabil. 1998;77:545–549. doi: 10.1097/00002060-199811000-00019
- McPartland JM, Brodeur RR, Hallgren RC. Chronic neck pain, standing balance, and suboccipital muscle atrophy—a pilot study. J Manip Physiol Ther. 1997;20:24–29.Elliott JM, Courtney DM, Rademaker A, Pinto D, Sterling MM, Parrish TB. The Rapid and Progressive Degeneration of the Cervical Multifidus in Whiplash: An MRI Study of Fatty Infiltration. Spine (Phila Pa 1976). 2015;40(12):E694-E700. doi:10.1097/BRS.0000000000000891
- Campbell DG, and Parsons CM. 1944. J. nerv. ment. Dis., 99, 544.
- Hinoki M, Hine, Kada Y. Neurological studies on vertigo due to whiplash injury. Equilibrium Research 1971;(suppl 1):5–29.
- Gimse R, Tjell C, Bjorgen IA, Saunte C. 1996. Disturbed eye movements after whiplash due to injuries to the posture control system. J Clin Exp Neuropsychol 18:178-186.
- Solow B, Sonnesen L. Head posture and malocclusions. Eur J Orthod. 1998 Dec;20(6):685-93. doi: 10.1093/ejo/20.6.685. PMID: 9926635.
- Huijing PA, Maas H, Baan GC. Compartmental fasciotomy and isolating a muscle from neighboring muscles interfere with myofascial force transmission within the rat anterior crural compartment. J Morphol. 2003;256:306–321.
- Stecco C, Gagey O, Macchi V, et al. Tendinous muscular insertions onto the deep fascia of the upper limb. First part: anatomical study. Morphologie. 2007b;91:29–37.
- Cuccia A, Caradonna C. The relationship between the stomatognathic system and body posture. Clinics vol.64 no.1 São Paulo Jan. 2009 http://dx.doi.org/10.1590/S1807-59322009000100011
- Strini PJ, Machado NA, Gorreri MC, Ferreira Ade F, Sousa Gda C, Fernandes Neto AJ. Postural evaluation of patients with temporomandibular disorders under use of occlusal splints. J Appl Oral Sci. 2009 Sep-Oct;17(5):539-43. doi: 10.1590/s1678-77572009000500033. PMID: 19936539; PMCID: PMC4327687.
- Lippold C, Danesh G, Schilgen M, Drerup B, Hackenberg L. Relationship between thoracic, lordotic, and pelvic inclination and craniofacial morphology in adults. Angle Orthod. 2006 Sep;76(5):779-85. doi: 10.1043/0003-3219(2006)076[0779:RBTLAP]2.0.CO;2. PMID: 17029510.
- Ramirez-Yanez G, Mehta L, Mehta NR. The effect of dental occlusal disturbances on the curvature of the vertebral spine in rats. July 2014Cranio: the Journal of Craniomandibular Practice 33(3):2151090314Y0000000017
- Amat P. Occlusion, orthodontics and posture: are there evidences? The example of scoliosis. J. Stomat. Occ. Med. (2009) 2: 2–10 DOI 10.1007/s12548-009-0001-4
- Bergamini M, Pierleoni F, Gizdulich A, Bergamini C. Dental occlusion and body posture: a surface EMG study. Cranio. 2008 Jan;26(1):25-32. doi: 10.1179/crn.2008.041. PMID: 18290522.
- Sakaguchi K, Mehta NR, Abdallah EF, Forgione AG, Hirayama H, Kawasaki T, Yokoyama A. Examination of the relationship between mandibular position and body posture. Cranio. 2007 Oct;25(4):237-49. doi: 10.1179/crn.2007.037. PMID: 17983123.
- Pradham NS, White GE, Mehta N, Forgione A. Mandibular deviations in TMD and non-TMD groups related to eye dominance and head posture. J Clin Pediatr Dent. 2001 Winter;25(2):147-55. doi: 10.17796/jcpd.25.2.j7171238p2413611. PMID: 11314215.
- Conti PB, Sakano E, Ribeiro MA, Schivinski CI, Ribeiro JD. Assessment of the body posture of mouth-breathing children and adolescents. J Pediatr (Rio J). 2011 Jul-Aug;87(4):357-63. doi: 10.2223/JPED.2102. Epub 2011 Jul 18. PMID: 21769416.
- De Menezes VA, Leal RB, Pessoa RS, Pontes RM. Prevalence and factors related to mouth breathing in school children at the Santo Amaro project-Recife, 2005. Braz J Otorhinolaryngol. 2006 May-Jun;72(3):394-9. doi: 10.1016/s1808-8694(15)30975-7. PMID: 17119778.
- Kumar R, Sidhu SS, Kharbanda OP, Tandon DA. Hyoid bone and atlas vertebra in established mouth breathers: a cephalometric study. J Clin Pediatr Dent. 1995 Spring;19(3):191-4. PMID: 8611488.
- Yi LC, Jardim JR, Inoue DP, Pignatari SS. The relationship between excursion of the diaphragm and curvatures of the spinal column in mouth breathing children. J Pediatr (Rio J). 2008 Mar-Apr;84(2):171-7. doi: 10.2223/JPED.1771. PMID: 18372937.
- Cattoni DM, Fernandes FD, Di Francesco RC, Latorre Mdo R. Características do sistema estomatognático de crianças respiradoras orais: enfoque antroposcópico [Characteristics of the stomatognathic system of mouth breathing children: anthroposcopic approach]. Pro Fono. 2007 Oct-Dec;19(4):347-51. Portuguese. doi: 10.1590/s0104-56872007000400004. PMID: 18200382.
- Langevin HM, Stevens-Tuttle D, Fox JR, et al. Ultrasound evidence of altered lumbar connective tissue structure in human subjects with chronic low back pain. BMC Musculoskelet Disord. 2009;10:151. Published 2009 Dec 3. doi:10.1186/1471-2474-10-151
- Osar E. Corrective exercise solution to common hip and shoulder dysfunction. Lotus Publishers; 2012
- Gweon HM, Chung TS, Suh SH. Evaluation of the Cause of Internal Jugular Vein Obstruction on Head and Neck Contrast Enhanced 3D MR Angiography Using Contrast Enhanced Computed Tomography. January 2011. Journal of the Korean Society of Magnetic Resonance in Medicine 15(1):41
- Chung CP, Chao AC, Hsu HY, Lin SJ, Hu HH. Decreased jugular venous distensibility in migraine. Ultrasound Med Biol. 2010 Jan;36(1):11-6. doi: 10.1016/j.ultrasmedbio.2009.08.007. PMID: 19900748.
- Koerte IK, Schankin CJ, Immler S, Lee S, Laubender RP, Grosse C, Eftimov L, Milde-Busch A, Reiser M, Straube A, Heinen F, Alperin N, Ertl-Wagner B. Altered cerebrovenous drainage in patients with migraine as assessed by phase-contrast magnetic resonance imaging. Invest Radiol. 2011 Jul;46(7):434-40. doi: 10.1097/RLI.0b013e318210ecf5. PMID: 21317790.
- Smouha E, Wanna G. Vertigo Lasting Minutes to Hours. Encyclopedia of Neuroscience, 2009
- Schuknecht HF, Boyev KP. Cochleosacculotomy. Otologic Surgery (Third Edition), 2010
- Harris JP, Salt AN. Audition. The Senses: A Comprehensive Reference, 2008
- Yamauchi A, Rabbitt RD, Boyle R, Highstein SM. Relationship between inner-ear fluid pressure and semicircular canal afferent nerve discharge. J Assoc Res Otolaryngol. 2002;3(1):26-44. doi:10.1007/s101620010088
- Cumurciuc R, Crassard I, Sarov M, Valade D, Bousser MG. Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatry. 2005 Aug;76(8):1084-7. doi: 10.1136/jnnp.2004.056275. PMID: 16024884; PMCID: PMC1739763.
- Gussen R. Vascular mechanisms in Meniere’s disease. Otolaryngol Head Neck Surg. 1983 Feb;91(1):68-71. doi: 10.1177/019459988309100112. PMID: 6405352.
- Benzon HT, Wu CL, Argoff CE, et al. Practical Management of Pain Book, Fifth Edition 2014
- Shreeve MW, La Rose JR. Chiropractic care of a patient with thoracic outlet syndrome and arrhythmia. J Chiropr Med. 2011;10(2):130-134. doi:10.1016/j.jcm.2010.09.002
- Meredith C.B. Adams, Hurley RW. Chemical Neurolytic Blocks. Practical Management of Pain (Fifth Edition), 2014
- Civelek E, Karasu A, Cansever T, Hepgul K, Kiris T, Sabanci A, Canbolat A. Surgical anatomy of the cervical sympathetic trunk during anterolateral approach to cervical spine. Eur Spine J. 2008 Aug;17(8):991-5. doi: 10.1007/s00586-008-0696-8. Epub 2008 Jun 12. PMID: 18548289; PMCID: PMC2518767.
- McDougal DH, Gamlin PD. Autonomic control of the eye. Compr Physiol. 2015;5(1):439-473. doi:10.1002/cphy.c140014
- Uemura T, Katsura M, Iwashima E. Repeated mecholyl tests on patients with vertigo. Equilibrium res. suppl. 3, 1972
- Franz B, Collis-Brown G, Altidis P, et al. Cervical Trauma and Tinnitus. International Tinnitus Journal, Vol. 4, No.1, 3/-33 (1998)
- Burke JP, Orton HP, West J, Strachan IM, Hockey MS, Ferguson DG. Whiplash and its effect on the visual system. Graefes Arch Clin Exp Ophthalmol. 1992;230(4):335-9. doi: 10.1007/BF00165941. PMID: 1505764.
- Kreuzer PM, Landgrebe M, Schecklmann M, Staudinger S, Langguth B; TRI Database Study Group. Trauma-associated tinnitus: audiological, demographic and clinical characteristics. PLoS One. 2012;7(9):e45599. doi: 10.1371/journal.pone.0045599. Epub 2012 Sep 26. PMID: 23049821; PMCID: PMC3458888.
- Bjorne A, Berven A, Agerberg G. Cervical signs and symptoms in patients with Meniere’s disease: a controlled study. Cranio. 1998 Jul;16(3):194-202. doi: 10.1080/08869634.1998.11746057. PMID: 9852812.
- Daneshmandi H, Majalan AS, Babakhani M, Karanian F. The Comparison of head and neck alignment in children with visual and hearing impairments and its relation with anthropometrical dimensions, Phys. Treat. : Specif. Phys. Ther. J. 2014; 4 (2): 69-76
- Yamagami T, Handa H, Higashi K, Kaji R. Brachial plexus injury with cough attack: case report. Neurosurgery. 1994 Jun;34(6):1084-6; discussion 1086. doi: 10.1227/00006123-199406000-00023. PMID: 8084397.
- Coumel P. Autonomic influences in atrial tachyarrhythmias. J Cardiovasc Electrophysiol. 1996 Oct;7(10):999-1007. doi: 10.1111/j.1540-8167.1996.tb00474.x. PMID: 8894942.
- Hsu YC, Sung SF. Spontaneous vertebral artery dissection with thunderclap headache: a case report and review of the literature. Acta Neurol Taiwan. 2014 Mar;23(1):24-8. PMID: 24833212.
- Go G, Hwang SH, Park IS, Park H. Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. J Korean Neurosurg Soc. 2013;54(3):243-245. doi:10.3340/jkns.2013.54.3.243
- Strupp M, Planck JH, Arbusow V, Steiger HJ, Brückmann H, Brandt T. Rotational vertebral artery occlusion syndrome with vertigo due to “labyrinthine excitation”. Neurology. 2000 Mar 28;54(6):1376-9. doi: 10.1212/wnl.54.6.1376. PMID: 10746615.
- Kuether TA, Nesbit GM, Clark WM, Barnwell SL. Rotational vertebral artery occlusion: a mechanism of vertebrobasilar insufficiency. Neurosurgery. 1997 Aug;41(2):427-32; discussion 432-3. doi: 10.1097/00006123-199708000-00019. PMID: 9257311.
- Dabus G, Gerstle RJ, Parsons M, Cross DT 3rd, Moran CJ, Thompson R, Derdeyn CP. Rotational vertebrobasilar insufficiency due to dynamic compression of the dominant vertebral artery by the thyroid cartilage and occlusion of the contralateral vertebral artery at C1-2 level. J Neuroimaging. 2008 Apr;18(2):184-7. doi: 10.1111/j.1552-6569.2007.00177.x. Epub 2007 Oct 22. PMID: 18298678.
- Dutton M. Dutton’s orthopaedic examination evaluation & intervention, 4e, 2016
- Kim SM, Seo MH, Myoung H, Choi JY, Kim YS, Lee SK. Osteogenetic changes in elongated styloid processes of Eagle syndrome patients. J Craniomaxillofac Surg. 2014 Jul;42(5):661-7. doi: 10.1016/j.jcms.2013.09.012. Epub 2013 Sep 28. PMID: 24161467.
- Sims AB, Stack BC, Demerjian GG. Spasmodic Torticollis: The Dental Connection. The Journal of Craniomandibular & Sleep Practice Volume 30, 2012 – Issue 3. Pages 188-193
- Sims A, Stack B: Tourette’s syndrome: a pilot study for the discontinuance of a movement disorder. J Craniomandib Pract 2009; 27(1):11–18.
- Freeman MD, Rosa S, Harshfield D, Smith F, Bennett R, Centeno CJ, Kornel E, Nystrom A, Heffez D, Kohles SS. A case-control study of cerebellar tonsillar ectopia (Chiari) and head/neck trauma (whiplash). Brain Inj. 2010;24(7-8):988-94. doi: 10.3109/02699052.2010.490512. PMID: 20545453.
- Tominaga T, Takahashi T, Shimizu H, & Yoshimoto, T. (2002). Rotational vertebral artery occlusion from occipital bone anomaly: a rare cause of embolic stroke, Journal of Neurosurgery, 97(6), 1456-1459. Retrieved Jan 22, 2021
- Cooperstein R, Young M, Lew M. Validity of palpation of the C1 transverse process: comparison with a radiographic reference standard. J Can Chiropr Assoc. 2015;59(2):91-100.
- Mosby JS, Duray SM. Vertebral artery dissection in a patient practicing self-manipulation of the neck. J Chiropr Med. 2011 Dec;10(4):283-7. doi: 10.1016/j.jcm.2011.01.007. PMID: 22654686; PMCID: PMC3315865.
- Reeves KD, Hassanein KM. Long-term effects of dextrose prolotherapy for anterior cruciate ligament laxity. Altern Ther Health Med. 2003 May-Jun;9(3):58-62. PMID: 12776476.
- Reeves KD, Hassanein K. Randomized prospective double-blind placebo-controlled study of dextrose prolotherapy for knee osteoarthritis with or without ACL laxity. Altern Ther Health Med. 2000 Mar;6(2):68-74, 77-80. PMID: 10710805.
- Hauser RA, Lackner JB, Steilen-Matias D, Harris DK. A Systematic Review of Dextrose Prolotherapy for Chronic Musculoskeletal Pain. Clin Med Insights Arthritis Musculoskelet Disord. 2016;9:139-159. Published 2016 Jul 7. doi:10.4137/CMAMD.S39160
- George S. Hackett (1960) Prolotherapy in Whiplash and Low Back Pain, Postgraduate Medicine, 27:2, 214-219, DOI: 10.1080/00325481.1960.11712804
Your article was eye-opening for me. I fell 14 feet onto my back in 2015 and survived well because I had been lifting weights regularly for 3 years(I did break my wrist, chip my ankle bone and have bump from hitting edge of patio and bump from large too that fell on forehead) and then had 6 car accidents in 2016 and 2017 when people hit me from sides and back of my car. My teeth are crooked and neck still uncomfortable when I sleep and posture I work on daily. In 2017 I worked with a medical massuese which helped my body and neck position some. What could be the one next step I could do, like exercises (your videos were so helpful). I live in Texas and am a retired teacher trying to get my health back- even weight lifting is uncomfortable! I see there is hope for me to get aligned again!!!! Thank you for your enlightening article, Kathy Balcer
Thank you for your comment, Kathy. Best wishes.
Your article was eye-opening for me. I fell 14 feet onto my back in 2015 and survived well because I had been lifting weights regularly for 3 years(I did break my wrist, chip my ankle bone and have bump from hitting edge of patio and bump from large too that fell on forehead) and then had 6 car accidents in 2016 and 2017 when people hit me from sides and back of my car. My teeth are crooked and neck still uncomfortable when I sleep and posture I work on daily. In 2017 I worked with a medical massuese which helped my body and neck position some. What could be the one next step I could do, like exercises (your videos were so helpful). I live in Texas and am a retired teacher trying to get my health back- even weight lifting is uncomfortable! I see there is hope for me to get aligned again!!!! Thank you for your enlightening article, Kathy Balcer
I hope to be neck pain and migraine free over the coming months by awareness and correction of my posture thanks to your article. Is there a pillow you can suggest? I find it very hard to real my neck muscles and get to sleep – I have tried a thin pillow and also no pillow and neither seems to work Thank you!
Thank you for this fabulous article! When I was six years old I fell out of the car at about 50 mph or so. -All my life I’ve had neck pain and migraine. DDD And arthritis in the neck causes a lot of my migraines. When I fell out of the car I rolled into a ditch and then up into a telephone pole and straddled the post. Also my left ankle was run over by the car. Freak accident And I have always thought my problems stemmed from this. I also have terrible posture forward head posture and slumped shoulders. Really bad. I have a reverse curve in my cervical spine. Can you tell me what sort of pillow to use? Also, Neck strengthening and no chiropractor? neck strengthening and no chiropractor? Thank you!
I agree, most likely it’s the cause of your affliction. The treatment for this kind of problem is complex and I can’t give you a “comment-answer”. However, lie on your side with a decent sized pillow. Never get neck manipulations if you have dizziness, migraines or similar as there’s a greater risk for vertebral artery dissection.
I hope to be neck pain and migraine free over the coming months by awareness and correction of my posture thanks to your article. Is there a pillow you can suggest? I find it very hard to real my neck muscles and get to sleep – I have tried a thin pillow and also no pillow and neither seems to work Thank you!
A high pillow if you sleep on your back, and keep your head forward if you sleep on your side. Don’t sleep on your stomach.
What an amazing article. I have never noticably injured my neck however I door have common bad posture and work at a desk. I went to the dentist Sep 27 and on Sep 30 went to the ER with a swelling right hand cheek bone and upper temple and 28mm jaw opening. ER concluded cellulitis and prescribed antibiotics. Since then i developed tinnitus, eustachian tube cracking, neck pain, migraines, sinus pressure, tender back of my head, tingling arms, offbalance/dizziness, blurry vision sllightly in one eye / inability to focus quickly. ENT, Rheumatologist, Opthamologist and Neurologist still haven’t been able to work out what is wrong. A brain MRI was done, blood tests etc and nothing out of the ordinary. 4 months later i’m back on antibiotics. Frustrated, I went to see a Physical Therapist who thinks I may have tight neck and she moved my C1 and C2 i believe. I seem to feel a little better. Can all of this really just be from my neck? It sounds like it can. Although I always go back to the weird temple swelling at the start of it all. ANyway, fab article, hopefully I’ll one day find out what is wrong. Jenny
Hello Jen, presuming that you have excluded temporal arteritis and other systemic etiologies, and that the situation is now indeed revered as “idiopathic”:
This is most likely a multifactorial problem and thus I don’t think it has one etiology. MRIs are usually noted as “normal” in patients with chronic, idiopathic pain. It depends who you ask and what you look for. Upper cervical facet joint subluxation and jugular vein compression can be visualized on typical capital MRI, however this is rarely if ever done (Goel 2015, Higgins 2015, Larsen 2018c).
I suggest that you are careful as to who you allow to treat your neck. I also suggest that you look into temporomandibular joint disorder, intracranial hypertension and thoracic outlet syndrome. I am not claiming that you have all these, but look into them and investigate for yourself. I have written extensively about these topics in this and other articles on my website, which are free to read.
Hi Kjetil,
thanks for the videos and information. I learned a lot thanks to this website and I’ve been trying to practice it for about 7 months. My neck and jaw no longer hurt and there is a physical change in my neck. The information here is really important and useful. But unfortunately there is no Rectus capitis lateralis exercise video. I’m really curious about this exercise video. Thank you.
Happy to hear that. I removed the rectus capitis lateralis as it may cause you more harm than good. It’s just too hard to monitor its progres and too hard to distinguish if you’re doing yourself harm rather than good.
are there any exercises/conservative therapy for facet joint sublixation at C1?
I’m talking about this situation “Sometimes I will find one transverse process far anterior to the mastoid process, and the opposite side properly lined up. This means that a facet joint subluxation has likely occurred.”. I thought that for facet joint subluxation treatment is different than using levator scapulae as pulling lever. So i can apply same exercises as for mere rotation of C1?
What an amazing article. I have never noticably injured my neck however I door have common bad posture and work at a desk. I went to the dentist Sep 27 and on Sep 30 went to the ER with a swelling right hand cheek bone and upper temple and 28mm jaw opening. ER concluded cellulitis and prescribed antibiotics. Since then i developed tinnitus, eustachian tube cracking, neck pain, migraines, sinus pressure, tender back of my head, tingling arms, offbalance/dizziness, blurry vision sllightly in one eye / inability to focus quickly. ENT, Rheumatologist, Opthamologist and Neurologist still haven’t been able to work out what is wrong. A brain MRI was done, blood tests etc and nothing out of the ordinary. 4 months later i’m back on antibiotics. Frustrated, I went to see a Physical Therapist who thinks I may have tight neck and she moved my C1 and C2 i believe. I seem to feel a little better. Can all of this really just be from my neck? It sounds like it can. Although I always go back to the weird temple swelling at the start of it all. ANyway, fab article, hopefully I’ll one day find out what is wrong. Jenny
I have been unwell for 7 years with severe headaches and pain at the base of my skull with vomiting when at its worse. I can barely open my mouth and a trip to the dentist takes me a week to recover from. I have seen neurologists, surgeons and have spent thousands and thousands of dollars on therapy, doctors etc. I have been seen by chiros who treated me with an Activator but had terrible consequences (vertigo) and am too terrified to go back. if I suspect atlanto-occipital torsion, what is my first step and who should I see? Thank you.
PS: your article is amazing.
I have been unwell for 7 years with severe headaches and pain at the base of my skull with vomiting when at its worse. I can barely open my mouth and a trip to the dentist takes me a week to recover from. I have seen neurologists, surgeons and have spent thousands and thousands of dollars on therapy, doctors etc. I have been seen by chiros who treated me with an Activator but had terrible consequences (vertigo) and am too terrified to go back. if I suspect atlanto-occipital torsion, what is my first step and who should I see? Thank you.
PS: your article is amazing.
Karen: My first recommendation is that you avoid getting your neck manipulated. As for treatment, I have written extensively about proper treatment for these problems. It’s not about who you see, but rather, about what the clinician actually does, i.e. the approach. If you want me to look over your images and prescribe a corrective plan, feel free to book a session via my website.
What a lot of fascinating information! I found my way to this article because I have Eustachian Tube Dysfunction. Some upper cervical chiropractors seem to be claiming that adjustments to address atlas/axis misalignment will help relieve my symptoms, but I’m not convinced, and even less so having read this article. I infer from what you write that you would NOT recommend chiropractic adjustment, and indeed I have begun to realise that such treatment for lower back pain (from which I have suffered all my life) is not necessarily the best way to go. Thanks to (among others) Dr. Stuart McGill, I have achieved better relief by strengthening my core musculature and stabilising my lumbar spine than from many years of chiropractic adjustment. But to the point: My ETD affects the left side, and is accompanied by impaired neck mobility (I can turn my head much further to the right than to the left), facial numbness on the left side, toothache on the left side and even wildly varying astigmatism in my left eye. Would you say that these symptoms could be caused by cervical misalignment (I have noticeable forward head posture)? Do you think the right way to go would be postural correction, rather than upper cervical chiropractic adjustment? If I were still living in Norway, I would almost certainly have consulted you in person. Unfortunately, I moved to Canada 17 years ago.
What a lot of fascinating information! I found my way to this article because I have Eustachian Tube Dysfunction. Some upper cervical chiropractors seem to be claiming that adjustments to address atlas/axis misalignment will help relieve my symptoms, but I’m not convinced, and even less so having read this article. I infer from what you write that you would NOT recommend chiropractic adjustment, and indeed I have begun to realise that such treatment for lower back pain (from which I have suffered all my life) is not necessarily the best way to go. Thanks to (among others) Dr. Stuart McGill, I have achieved better relief by strengthening my core musculature and stabilising my lumbar spine than from many years of chiropractic adjustment. But to the point: My ETD affects the left side, and is accompanied by impaired neck mobility (I can turn my head much further to the right than to the left), facial numbness on the left side, toothache on the left side and even wildly varying astigmatism in my left eye. Would you say that these symptoms could be caused by cervical misalignment (I have noticeable forward head posture)? Do you think the right way to go would be postural correction, rather than upper cervical chiropractic adjustment? If I were still living in Norway, I would almost certainly have consulted you in person. Unfortunately, I moved to Canada 17 years ago.
Takk Kjetil. Hva angår Skype er budsjettet mitt nokså stramt akkurat nå, så vi får se. Jeg vil imidlertid kommentere at etter å ha lest dine fascinerende artikler så har jeg prøv å være mye mer oppmerksom på min kroppsholdning, spesielt hva angår nakken. Jeg har lenge vært oppmerksom på at jeg har markert “forward head posture”. Det er mulig at det bare er innbilling eller ønsketenkning, men synes jeg opplever at når trykket i venstre øre kjennes som verst, kan jeg oppnå en liten bedring ved å innta en bedre stilling, dra hodet litt bakover og oppover og kanskje snu hodet LITT fra side til side. Slik jeg ser på det, styrker dette min overbevisning om at problemet med det eustakiske røret er på en eller annen måte forbundet med klemming av nerver, og IKKE, som to ØNH spesialister har påstått, at jeg hadde ørebetennelse som barn! Jeg skal lese gjennom denne artikkelen og den om Vestibular impairment igjen. Jeg vet at du har noen forslag til øvelser her og på YouTube, og skal prøve å prakisere disse litt mer systematisk.
I haven’t been able to read your full article but I’ve been with skimming through it and reading different things and I’m not doing very well..
I’m very scared I went to my dentist on December 5th 2018 and he filed a bottom tooth down but he also buffed or shaved some of the teeth on the back like took he out structure like he took out the density or something from the teeth from behind I know this because I’ve had braces and my teeth where totally different he should have never filed down any of my teeth and all I really needed to do is get like Invisalign or something put on the bottom to move those teeth in place..
I have an implant on top #9 and the reason why he filed a tooth so he says is because of a tooth that was sort of hitting the implant but it really wasn’t he also did a filling prior to this and that was a reason why I came in to see him on December 5th because I was getting some pain and I have some bone exposure because of where he put the anesthetic when he gave it to me my body went into shock like I literally shook and was like a convulsion this is what he did to filling and this was prior he also flattened that tooth he took out a silver filling and put in a white one he didn’t even do a very good job at that either..
I’m not really sure why I went back to him it’s a long story and I don’t even know if I have a case to stand on with this guy but right now
I just want to get my face back and my teeth back the way they were to some degree but what really important is getting my joints and my jaw in a better place ..
I know that things were totally different because I have retainers and when I first put my retainer on after he did the filing the retainer fit really tight and it never was like that it fit perfectly fineand I mentioned this to my dentist at the time and he says that doesn’t make any sense your retainer shouldn’t fit tighter it should fit looser because I took away structure so how could it fit tighter well it did and to me whatever he did he changed the occlusion and he also changed the structure which is not good to do and I have a feeling that this is where it all started…
My bottom teeth are shorter in the front than they were and structure was taken out from the back side because he did some type of buffing or filing on the backside of the teeth they are blunt so much that they’re like sharp on the backside..
It also changed how my tongue would position itself and now I feel like I do more thrusting on my bottom teeth and I never did that before and where that nerve is for me is on my left lower side of my jawI can feel that nerve radiate and I can feel pulling I can feel it go to the other side so the right side is getting worse I can feel like your neck is swollen there so many things and I’m scared to death..
I get problems with that area I’m getting numbness and pulling in my face my face sometimes looks distorted…
I will tell you this that I’m not doing very much activity and very depressed and I’ve been laying around quite a bit sleeping a lot I was also in the hospital because of this, because it mentally has caused me to not want to be here anymore which is not good….
I was wearing retainer on the top and the bottom of my teeth normally all the time and now I can’t wear the top one because of the alterations that were done to my molarsI also was wearing a night guard on the top but it’s a soft one was that really soft but it’s softer than like the harder ones and it’s kind of smaller in front and fatter in the back and I was told I really need a flat one…
I believe this has changed my occlusion because I know that your bottom teeth are supposed to protect your tongue and your upper teeth are supposed to protect your bottom lip from the inside being bit down on..
And that’s not the case I’m actually I’m not biting my tongue cuz my teeth are just short enough to not do that but it’s pretty close but I do sometimes kind of almost bit it and when I eat my teeth will clang against each other in a way that’s not normal how it normally was with how my structure was and how everything was in place..
I’m very upset that my teeth have been filed because it took the way the structure and he flattened the teeth so basically he weakened the teeth they are blunt or hard actually they feel weaker and not as strong it’s very upsettingto me teeth are three-dimensional and if you take away structure and start filing things to make things look sharp and blunt he basically took away that round this and that phone that I had which to me cut my teeth looking at least somewhat beautiful looking and healthy…
I can’t even tell you and even the way my smile is everything is wrong. I hate it so much.
I get this pulling on my face my face looks distorted at times symmetry is totally not right at times it’s weird and I know it’s because of all this..
I also have a bite issues as well because the dentist also did some buffing and filing down of a tooth and took the structure all the way down to the gumline because he did that I was in so much pain I had to go back and he had to put bonding material on the side of my tooth because he was just supposed to kind of take the edge off of this little scuffy area and instead he bought the tooth all the way down to the gumline taking structure away completely then I had to go back there he had to put bonding material on the side of the tooth and it liked overlapped and now there’s some bonding on the bottom of the tooth as well which is probably one of the reasons why my bite is not connecting correctly ..
Yeah I know this is crazy but I’m ready to cry I’m crying like every day because of this and after seeing 2 orthodontists there is deterioration and bad things going on with my jaw so I truly believe that these alterations all these things that have been done to my teeth have caused issues with my jaw to get worse meaning I was living thinking I was okay but really I probably wasn’t with my jaw but then you go and start doing things to the body and changing things and that will start to add extra stress to an area that’s already not doing well there going too be problems…
So to me it’s kind of like taking ball tires on the expressway and basically everything that’s been done to my mouth by the dentist is the expressway…
My tongue is not resting normally and the numbness and pulling of my face the radiating pain in my jaw, I feel like I can’t hear anymore I have tinnitus in my right ear and have had it on and off but it’s getting quite worse and my left ear is pretty bad now and my neck my bite aesthetically everything to me does not look as nice and beautiful as a sort of did it prior to December 5th or I should say prior really to when he did the filling because I had mentioned that I went into shock and my body and everything so I know if he hit a nerve but I have bone loss by that tooth where he did the injection..
I’m not really sure how I’m going to get this fixed and I’m scared I’m going to have to get jaw surgery or something down the road..
I also have rheumatoid arthritis and I don’t have any more cartilage early left in my hips I would get flare-ups different times and basically I wound up on disability because of it but I was doing pretty good but I know that I’m going to have to get them replaced regardless I’m sure…
But for me right now what’s going on with my jaw and my teeth and everything being all disfigured and everything to me that’s really the most important thing ..
I’ve lived with my hips for all this time I’m not somebody who’s overweight but if I were to gain a lot of weight I would imagine that would be no different than what the dentist has done to my teeth and that would be like again putting ball tires on the expressway having extra weight on would definitely cause that..
I am however noticing that I’m having more issues with my joints because I’m not being active as much and I am laying around and not doing anything and that is definitely causing some issues with my hips and joints through out my whole body…
And of course it’s winter over here right now and the weather is very strange at times I live in Chicago, Illinois and it’s not the greatest at times so I don’t do very well with this type of weather it can be pretty stressful on my joints depending on the barometric pressures…
I need help I’m trying to get some help the orthodontist wants me to go see an oral surgeon and a prosthodontist, I also have an appointment on Monday with my ENT ear nose and throat doctor to try to get some answers I’m just not sure what to do….
I’m so depressed this has caused me so much depression I’m crying everyday and I don’t want to do anything and functioning is very hard for me..
I’m looking for some advice some answers from you somebody who can help me this my dentist really screwed up my teeth my bite my jaw my nerves and my mental health all have been affected and it’s a living nightmare…
I feel like my teeth they are small on the bottom compared to how they used to be when I started brushing my teeth I was like what the hell where’s my teeth I’m used to having more structure when I brush and this was right after he did the procedure…..
And of course if you look at my teeth you might think they look fine you might not be able to tell but it’s an illusion…
And some of the dentist’s can tell but some are so stupid can’t tell and really good orthodontists can and have said things need to be fixed and yes structure has been altered and they have said it’s going to take a village to fix this that it’s not good and it’s going to cost you $25-$35,000 too fix this..
I’m crying……
All these things that just totally went wrong the flattening of the cusps area on my one molar on the bottom left and filing and buffing all way down to the gumline on the top molar on the left hand side this is just so bad and with the fact that he filed and did all the stuff to the front bottom teeth I’m pretty sure he touch 6 teeth on the backside and if not for sure 4 of them…
Because when I put my retainer in which fit completely my teeth were all in line with the top part of the retainer you can see where the structure was taken out you can see how much structure he took out and for somebody to say that he swears that he only filed one tooth it’s unbelievable what he did…
I live in Chicago, Ilinois I don’t know if you know anybody out here or what tests or procedures or anything that you can recommend for me too do or who to see…
I’m desperately looking for answers and a way too get this fixed to some extent..
I also read an article before reading yours about this lady who had an issue with her jaw and she has dental work done as well and she had something that affected her system because of the herpes virus being in her system and I mean cold sores not the other one, well something happened too her because of all this…
And for me at the end of the these procedures I wound up having a really bad cold sore which I haven’t had in years so if there’s a way that I can send you that article about this lady I would like to have you read it and get you feed back on what you think about that as well…
I want to be back to my free spirit loving fun outgoing person that I’ve always been I’m not somebody who stays home and locks themselves in their bedroom I’m not somebody who is homebound I’m a outgoing free spirit fun person and I love people I’m a very engaging person and this has been taken away from me due to all this…
This has been so horrible for me that I was actually in the hospital from New year’s Eve for like 8 days because of where this put me mentally…
Thank you so much for the time and listening and your feed back…
I want to give you my email address if you like to give me anything that will help or
even my mailing address…
Sincerely,
Christine Anderson
[email protected]
After reading your post I was reminded of what my mother went through before she was diagnosed with a pituitary tumor.She went through several retainers and had teeth pulled.The tumor was excreting growth hormone intended to add height in teenagers.But in an adult it causes cartilage to become thick.Her facial features including her jaw began to look horsey.Her hands and feet and hips were also affected.She was in a lot of mysterious pain.After she had the tumor removed her body and face returned to normal.Good Luck,Deb
I also wanted to add that I have issues with twitching in my left eye as well and vision disturbances at times low blood pressure clenching and biting down on the jaw more then I did before cuz I feel like the bite is not right more so with the front teeth placement and I think my jaw is misaligned..
I think I have a overbite / maybe open bite I’m not really sure because of the alterations on the teeth and everything going on with the jaw…
And because of things being not right muscles that are being strained pulled in different directions than they’re used too…
I think….
This is my observation of what I think has contributed to everything being really bad….
I’m also dealing with menopause I haven’t had my cycle for quite some time probably since August and this is something that’s been going on so once I pass August it’ll be 12 months and that means I’ll be in full-blown menopause so this has added to the stress and health..
And with the pain in my jaw I was taking Norco10 and Prednisone 5mg but the Norco starting to bother me so then I switch to Tramadol and now I’m not sure if I can take the Tramadol I was on Tramadol for quite a while at one time years ago but because of the SSRI and that started to give me some issues with my serotonin levels and it really screwed me up…
So I’m not sure if I can even take a Tramadol or if I might have issues with SSRI drugs I know I get more body twitching when I am on the Tramadol and I noticed that I get more but I also get it with a Norco too sometimes but I do notice that it’s more with the Tramadol and I’m getting more of hot flashes being on the Tramadol I really think it actually affects it…
I also went through breast cancer it’ll be
3 years in June..
I went through a lumpectomy surgery to take the lump out then I had a second surgery and I had 19 lymph nodes taken out and then I had 31 days of radiation…
And with what I have going on now with my jaw, my teeth I feel very off at times it’s not right..
And I will tell you this that mentally what this has done too me and physically that going through the breast cancer and everything that I went through has been 100 times easier than what I’m going through now and I know it may sound crazy but it has been…
I’m scared I just want my life back…
Thank you again
Christine..
Thanks for the comprehensive article. Anyway, I’ve been having odd sensations on my face mainly the jaw, nose and cheek area whereby I feel like bugs crawling, cobweb sensation, or like a hair strand on my face. Could that be caused by the neck? My cervical MRI states that I have a flat neck and mild bulging from C3-C7?
Do you have rosacea? I had rosacea and the crawling sensations were from Demodex mites. I used topical ivermectin for 4 months which solved the problem.
Thanks for the comprehensive article. Anyway, I’ve been having odd sensations on my face mainly the jaw, nose and cheek area whereby I feel like bugs crawling, cobweb sensation, or like a hair strand on my face. Could that be caused by the neck? My cervical MRI states that I have a flat neck and mild bulging from C3-C7?
Hi,
Do you do Skype consults?
Yes: https://mskneurology.com/booking
Hello,
This is a truly incredible article. I have been searching for info related to neck injuries specifically relating to the vagus nerve. My husband was trying to strengthen his neck with a lightweight band. The following day he woke up with his jaw pain and ear pain that gradually got so bad he went to the ER. They gave him muscles relaxers and those helped but still had ear and jaw pain if he didn’t take them. A week passed and he suddenly got intense symptoms while at work -where he looks down almost all day long. These symptoms got so bad-rapid heart beats, shaking, anxiety and pains in chest he was taking to the ER fearing a heart attack. Ekg was fine. All blood work normal but when we explained we were worried he hurt his kneck and this was the cause of these new symptoms they just insisted it is from stress. Now it’s been 2-3 weeks where he is having slight ear pain but intense “panick attacks” rapid heart rate, feeling like his out of control to the point of thinking he is dying etc so bad he wants to go back to the ER. I’m almost certain this has to do with his neck excersise he tried as he has never had this problem before. I think he hurt his vagus nerve due to my research and it’s correlation to fainting feelings, heart palpitations/ effects, anxiety, ear ringing, pain in ears and jaw etc. We saw chiropractor 1st time it happened when his jaw pain and ear pain were present and it almost instantly relieved all symptoms. Pain and emotional stress and anxiety all disappeared but then slowly returned. Now after reading this I am worried that chiropractic care is dangerous in this situation. What is the best way to get this diagnosed or at least looked into. No x-rays have been done or anything looked into relating to his neck pain. What would you recommend to ask for? I feel like something is compressing or triggering his vagus nerve but that really is only my best guess. If this is something you think you can help him with via a Skype call please let me know so I can schedule this with you asap, it seems no one is taking it seriously and he is unable to function normally. Thank you so very much.
I need to review his neck and head MRIs. Let’s discuss this in a skype session. Booking here: mskneurology.com
Hello,
This is a truly incredible article. I have been searching for info related to neck injuries specifically relating to the vagus nerve. My husband was trying to strengthen his neck with a lightweight band. The following day he woke up with his jaw pain and ear pain that gradually got so bad he went to the ER. They gave him muscles relaxers and those helped but still had ear and jaw pain if he didn’t take them. A week passed and he suddenly got intense symptoms while at work -where he looks down almost all day long. These symptoms got so bad-rapid heart beats, shaking, anxiety and pains in chest he was taking to the ER fearing a heart attack. Ekg was fine. All blood work normal but when we explained we were worried he hurt his kneck and this was the cause of these new symptoms they just insisted it is from stress. Now it’s been 2-3 weeks where he is having slight ear pain but intense “panick attacks” rapid heart rate, feeling like his out of control to the point of thinking he is dying etc so bad he wants to go back to the ER. I’m almost certain this has to do with his neck excersise he tried as he has never had this problem before. I think he hurt his vagus nerve due to my research and it’s correlation to fainting feelings, heart palpitations/ effects, anxiety, ear ringing, pain in ears and jaw etc. We saw chiropractor 1st time it happened when his jaw pain and ear pain were present and it almost instantly relieved all symptoms. Pain and emotional stress and anxiety all disappeared but then slowly returned. Now after reading this I am worried that chiropractic care is dangerous in this situation. What is the best way to get this diagnosed or at least looked into. No x-rays have been done or anything looked into relating to his neck pain. What would you recommend to ask for? I feel like something is compressing or triggering his vagus nerve but that really is only my best guess. If this is something you think you can help him with via a Skype call please let me know so I can schedule this with you asap, it seems no one is taking it seriously and he is unable to function normally. Thank you so very much.
Hi,
This was a really interesting article and as I have been suffering with a whole bunch of symptoms that no one has been able to identify the cause of yet, I do believe the culprit might be weak neck muscles and atlas misalignment.
I just wanted to ask how often do you recommend doing these exercises? How long will it take for my neck muscles to get stronger?
Thank you and best wishes from Manchester!
I am blown away by this article. I havent had any previous health issues or symptoms for 25 years until June 2019. I went to the dentist and had an impacted wisdom tooth removed on my left side and the dentist pushed down so hard on my jaw I cried out. A couple weeks later I woke up with the worst stiffness and pain in my neck and it hasnt been the same since. Constant cracking and grinding and pain and a non stop headache ever since for 8 months. I developed Visual Snow Syndrome in the end of June, a neurological syndrome related to aura migraine. No previous history of migraines. Tinnitus came on, then awful stomach burning and gurgling. Endoscopy and colonoscopy clear, tons of diets and things cut out with no changes it still persists every day. Jaw pain that wasn’t there before like my muscles are just sore all the time. Tensor tempani/roaring in head anytime I open my mouth wide enough or yawn, sometimes the fluttering in ears. Chronic dry sinuses. Chest pain with clear ekg and stress ultrasound cant find a reason. Then joint pain started in my knees and ankles, random burning sensations too. All my joints especially my shoulders have started to crack whenever I move(but no pain). Pain in my back began a few weeks ago. A chest xray revealed dextroscoliosis I had no idea of. I have tested negative for ana factor, rheumatoid arthritis, thyroid issues, lyme disease, celiac, been to the er 3 times, mri showed nothing abnormal. All tests normal. All of my doctors said they think its anxiety which is completely insane, I had to go out of my way to find a physical therapist because they wouldnt do it so I could finally get a neck xray done and it showed straightened neck and a misaligned atlas. I cant help but thinking that my atlas has caused all of this…could it be possible for it to have become misaligned from the harsh tooth extraction separating the tooth from the bone last year? So much pressure there was a crack? All of this began then. I have gotten to the point I am about to be diagnosed with fibromyalgia because the docs dont know what to do anymore. They cant explain it. I know there has to be an answer. The physical therapy I go to they just tell me to do exercises they printed out and correct my posture and it has been nearly two months and I feel I need something more. I feel no different. I do all I can to improve, my health means everything. My life is so different i am terrified to lose my job. Should I look into finding a place that does atlas orthogonal and see if i am a candidate? It is very hard to live like this. I spend every day researching and advocating for myself and so far I have found no relief. Your article is I feel the closest I have come to some answers so thank you for putting all of this out there. I know i have a lot of questions and am a complicated case, i dont expect you to have all the answers. Just wanted you to know i have been feeling hopeless for nearly a year and you have given me some hope.
Consider booking a session, I don’t have time to respond to long comments like this; my apologies.
I’m 26. For 4 years I have had extreme debilitating right upper neck pain and right shoulder pain( more trapezius area) started after working in ER as a scribe. Sometimes pain radiates down my right arm, also throbbing pain. I’ve had injections, RFAx2, physical therapy, acupuncture, chiropractor, 2 cervical ‘MRIs read normal except slight bulge c6-c7. The chiropractor I recently started going to found my atlas is rotated 10 degrees to the left. Along with many other findings. I’ve been getting adjustments 3x a week going into 4th week. No pain reductions. I am feeling hopeless and don’t know how much longer I can keep going on in this debilitating pain. Will this ever get better? Please help.
It sounds like thoracic outlet syndrome.
Don’t get “atlas adjustments”, they don’t work, and may be dangerous.
Hi my name is Kayla, I’m 26 years old. I have been suffering from extreme right sided neck pain and right shoulder/trapezius area pain x4 years. Initially starting after working in ER as a scribe. It’s debilitating and no one can figure it out. I’ve tried numerous things, with no avail. Physical therapy, chiropractor, medical doctors, trigger point, RFAx2, massage, acupuncture, Ect. MRI is normal, except slight bulge c6-c7 which they say isn’t enough to cause any pain. Recent Xrays show: atlas out of alignment, along with rounded shoulders, straight cervical spine, extreme back curve, one hip higher than the other, one leg shorter than the other. I have been going to new chiropractor 3x a week for 1 month now. Even he doesn’t know why I’m in so much pain and what to do. Suicidal ideation is creeping in every day. Do you think it’s possible to fix my pain? And what is the cause?! Please help.
X-ray doesn’t show atlas out of alignment. Don’t trust this. You need an MRI. However, unfortunately, due to your utterance of suicidal thoughts, I dare not advise you anything else than seeking out a psychiatrist. Take care.
Special X-RAYS taken for advanced atlas orthogonal do show atlas misalignment. Mine was shown to be off by 3 degrees.
These are not reliable whatsoever.
Thank you so much for this informative science-based article.
I had an unnecessary neck adjustment back in 2015 where a chiropractor forcefully rotated my neck to each side, and after that, I’ve been experiencing TMJD and many spinal misalignments. Over time, my jaw has become visibly misaligned and my face uneven.
I went to another chiropractor who did an atlas adjustment using a little device, and it momentarily felt better, but got excruciatingly worse. The x-ray he took showed that when my jaw is open, it is shaped like an uppercase L rather than a V. It’s extremely misaligned.
After the trauma from the bad adjustment, I have started to habitually clench my jaw, have been having headaches, have been having eye pain and vision disturbances on my right side (the side where my neck and jaw are the tightest). I’ve had muscle spasms in my suboccipital muscles and in my neck.
I went to a PT and he needled my suboccipital muscles (which I now know was not an effective treatment).
Most of the other articles I read when trying to find solutions to my atlas/axis/tmj problem point to NUCCA or other chiropractic therapies (which I don’t trust). Thank you for such a thorough, science-based article that I trust will be helpful and lead to change once I focus on changing my posture and committing to the exercises.
What would you recommend as the best approach to implement your solutions (would it be dangerous for me to attempt them alone)?
Thanks and stay safe and healthy.
Consider booking a session. My general recommendations are seen in this article.
As Mr. Larsen said, any chiropractic adjustment is a charade at best, but those with high-velocity thrust on the neck are extremely dangers, I got severe neck instability from those, its worse than playing with fire. This page raises awareness against chiropractic manipulations and have many patients testimonies: https://www.facebook.com/profile.php?id=100087855409011
6 months ago I have back pain, uneven hip, a higher ear.
i am from america center
Hi there, I’ve just looked into all of your videos and articles and find a lot of your work really fascinating. Doctors in Canada were very hesitant to diagnose me with TOS back in 2015, but here I am now having gone through many of the things that you advised against. For example, a lot of the physical therapists had me pulling my shoulder blade back and down during my back exercises and scapular strengthening. Stretching my right arm was almost impossible. The right arm already feels constantly over-stretched. Stretching my right pec hurt me the most. I eventually got an epidural in my C7 in Canada because they thought maybe my TOS pain in my right arm was coming from the neck, but it was not. Weeks after the epidural, I started experiencing a lot of head symptoms like headaches, tingling, occipital pain, ear pain, face burning, pressure behind eyes, etc.. basically felt like every cranial nerve had been affected. Thanks epidural! Years later, I still have some of these symptoms, which seem to come on whenever I bend down, squat, get stressed, exercise, valsalva maneuver, pretty much any exertion.
I tried a course of physical therapy for a dual diagnosis of neurogenic TOS and occipital neuralgia/cervicogenic headaches. They started me on neck strengthening such as chin tucks and some other isometric neck stuff. Then rows and scap strengthening. Just as your article stated, they were initially very hard to do, and would sometimes radiate nerve pain into my right arm which was odd to me considering I never thought I had any radiculopathy and all my neck MRIs were normal. But I imagine a combination of having TOS and now a neck flareup from the epidural could have affected the lower Cervical vertebrae too. Anyways, I continued physical therapy and I managed to become more capable of performing the cervical exercises, even the chin tucks which triggered the most flareups in the head. I would still get a lot of tingling in my left ear and sometimes headaches after the treatments, but they would have me go through some cervical traction, which would sometimes reduce the discomfort. Heat helped too. The main reason I started physical therapy was because as long as I would put on one of those manual cervical traction pumps you find on Amazon, I could pretty much get through any exercise without experiencing too much pain in my head. But wearing the cervical traction pump long term was not a solution. All the pump is doing is providing traction and not really addressing the main issue and likely further weakening my neck. So my attempt at physical therapy was to avoid needing the traction pump to push through exercises without experiencing head symptoms. I eventually over-did a chin tuck once and triggered my symptoms really badly.
Despite making some progress after 1.5 months, I eventually quit physical therapy as I was getting frustrated, and decided to see an atlas orthogonal chiropractor to check and see if maybe there were structural issues that strengthening would not correct. They found that my atlas was rotated by 3°, my C2 had some rotation, and my left clavicle had some issues. I’ve now gone through three weeks of advanced atlas orthogonal adjustments using sound waves. I’ve noticed some minor improvements in other parts of my body but not really in the head yet. Perhaps it’s too soon. My last visit after a week break, they had determined that my atlas was actually holding and so they didn’t adjust it. That was despite still having some head pain which was a little bit confusing to me. I just imagine patience is a virtue and I know all about retracing. I like my chiro, and she encouraged me to give it more time since I’ve been in a chronic state for over 3 years.
I’m really fascinated with your work and I am considering trying some of the exercises that you suggested but I want to make sure I give my body enough time to heal from the atlas adjustment. I’m also scared to start up physio again here in the states and run into some of the same misguided techniques you eloquently pointed out.
Thanks,
Shayan
PhD candidate
Very sorry, I don’t have enough time to read long messages. Consider booking a skype consult.
Thank you for the article! Life changing!
I was rear ended very hard and 8 months later I started having shoulder pain. Went to physical therapy when one day I couldn’t depress my shoulders. I think they figured thoracic outlet syndrome. They popped my top rib back down and over the next 2 weeks muscles between my neck and shoulder started to spasm and I would get them massaged out. Eventually the pain moved into my neck. PT didn’t help there, perhaps she didn’t have enough experience. I went from doctor to doctor. Got an MRI and found I had a bulging disk pushing into a nerve, I think at C5-C6.
Googling symptoms I found an article and it read like my life for the past year of trying to get to the bottom of my pain; 15 of22 symptoms matched up. I ended up at a NUCCA chiropractor. These guys do very gentle low velocity adjustments. However I do hear a sort of wet sandy crack, it sounds like it comes from the Chiro’s hands and not my neck, that makes me think a ligament is being abused.
I see that you don’t care for Chiropractic adjustments. I normally won’t go near a chiro; but pain will make you try things. I thought I’d tell you my story. I always feel something is off at a chiropractor
About 5 minutes after my first NUCCA adjustment my neck completely relaxed and it was like I was waking up from a dream. I believe that was the vertebrobasilar insufficiency. Colors seemed brighter and I could literally feel my thinking change. I had been incredibly worried about my memory; I thought I was getting some kind of alzheimers at 33.
So adjustments seemed to be a 3 steps forward and two steps back until the next adjustment. My neck felt great right away, but I had some episodes where all of a sudden I could not do simple tasks. I could not add 15 and 17 together, I just stared at them knowing I wanted to add them. I thought I could be having ischemic strokes. I ended up getting a neck and brain MRI to be safe.
My NUCCA Chiro says those episodes are common, but couldn’t give me a real answer; we both kind of arrived at the new increased bloodflow to my brain sort of rebooting it.
After 1 month of adjustments I found your article and started doing all the exercises, as well as adding in a 45 minute walk 4 times a week. While walking I externally rotating my shoulders and made sure to be “long in the neck.” It felt weird, but my posture adjusted to be comfortable quite quickly doing this. I think getting the blood moving was a huge factor. I started having back muscles feeling very fatigued, like some of them were finally loosening up. My spine is much happier now and the tired back muscles have gone away.
The nerve pain in my neck in nearly gone. My left shoulder is no longer raised, my head sits correctly on my neck. My suboccipitals have softened up. Headaches have gone away for 2 weeks today. Increased energy and confidence, depression is gone.
So I started some light 145lbs barbell squats and deadlifts. I go very slow, under control, neck straight. I don’t know if they help, but it feels really good to do some full body movements again. As well as rows and shoulder external extensions. I don’t do any movements over my head yet. I feel like I’m almost out of the hole.
Again thank you for the article. My recovery went into high gear after I began your exercises.
If you have any suggestions I’d appreciate them.
Hi Kjetil! so is Nucca dangerous for CCI? Do you have to have an upright MRI with flexion to be more precise? My Nucca chiropractor wants me to come back but after last session I had the worst occipital headache of my life and was vomiting! Ahh so confused!
Read the article. Regardless, you answered your own question.
Hey Kjetil,
I have a reversed neck curve, are those exercises ( particularly the deep neck flexors / subboccipitals exercises ) approriate for me ?
Yes
Three week ago I have been to chiropractor which manipulated with my neck and was correcting the atlas using some vibrating machine (atlas method). After that procedure I was very sleepy, started to have strong headaches especially on the right side along with my eye and ear. I could not tolerate high noises and photophobia. After some days the pressure around my throat came and pain in my occipital area and neck. She told me it is normal reaction and should dissapear in few days. It did not. Now she says it can take up 3-6 months. I am so devastated and cannot function at all. I feel pressure in my ears and head in general. I have been to ER, everything came back fine even CT of the brain, they gave me analgin through my vein and I have been good for about a week. Yesterday I had a major headache attack and nothing helps. I still have strong headaches. What should I do, please help me.
I have visual snow. I have a bad posture and posture.
which skype session should i choose?
Paypal is not used in our country (Turkey).
Are there any SWIFT or similar in payment methods?
No, sorry.
Which exams should I send you for visual snow? I want to skype with you after the hospital visit.
MRI head neck. Vascular scans also if you have them.
I have visual snow as well
Hi Kjetil! In your opinion, can “atypical face pain” (Dull ache in angle of jaw) be from atlas misalignment, cervical instability, or poor posture related?
It’s usually trigeminal. If not trigeminal, can be facial nerve or cervical plexus.
Could also be cervical disc compression of the trigeminal nerve nucleus in the spinal cord.
http://www.ajnr.org/content/ajnr/11/3/609.full.pdf
This is a cervical plexus-affecting hernia, most likely mainly greater auricular neuralgia, which was misinterpreted as trigeminal neuralgia. You do not get trigeminal symptoms from disc herniations as it is a cranial nerve.
I am an orthopedic surgeon and deeply impressed by your profound research and insight! I self-diagnosed with left c1 malpositioning 4 months ago and started treatment with chiro, massage and stretching. That lead to TOS, severe vagus impairment, sacroiliac joint and lower extremity muscle pain. I started with your exercises 1.5 weeks ago and already see a massive improvement. The only remnant is a tight iliotibial tract (maybe you’ll have there a good exercise as well). I just wanted to thank you and wish you the best for med school in 2021 and eagerly looking forward for any new articles/publications.
Kind regards,
Stephanie
That’s great, I’m happy for you. I appreciate your kind wishes!
The “ITB“ problem could be meralgia paresthetica, L5 radiculopathy or true ITBS. Based on your other lower body problems it’s probably MP which is just a subproblem of LPES. As a default strategy that’ll probably work, unless it’s L5, is strengthening of the TFL and Psoas. See my YouTube for exercises.
Thank you so much for writing this, Kjetil! I had double jaw surgery in Dec 2019 to fix class III malocclusion and an underdeveloped maxilla. I’ve been going to traditional chiros for years for headaches and neck pain, but my pain persists (headaches mostly gone, but neck pain isn’t). Post-surgery, the two sides of my face have been very different in healing: my left side (no neck pain) hardly lost any feeling, while I still have lots of numbness in my face and palate on the right side (where I have all my pain). My right eye is also slowly drifting out and up over the past few years, especially when I track down or to the left. Also have the scapular winging you mentioned. I’m starting to think these things are all related to an atlas subluxation. I’m seeking out a NUCCA chiro now to help me look at that area precisely, and your article is really guiding my questions for my first appointment with this new practitioner. I really hope he will pay special attention to my A-O joint, not just the A-A. Do you have any specific thoughts or advice for me going into this first appt?
If you read the article, you’ll see that I don’t recommend manipulation therapy at all.
Out of curiosity, if not a Chiro, who should one see to correct neck hinge or Other postural Issues which could be causing compression of IJV?
This is incredible work. Fantastic write up. Thank you very much. Not even doctors, much less chiropractors or physical therapists, have such a deep knowledge and understanding of this area of the spin.
You may not know this, but CCI & AAI have suddenly become a very interested & pursued topic in ME/CFS patients & community. I think your article will be very helpful. I think that applying some of your therapies may even help ME/CFS patients with MILD symptoms or instabilities.
Ah, just saw your ME/CFS article. I am glad you are aware. Thank you for writing about it and taking an interest!
Now after having read your ME/CFS article, it appears that your article predated the ME/CFS community interest in CCI/AAI in early 2019 due to Jen Brea’s & Jeff Wood’s public announcements of their diagnosis. So you actually may not know of ME/CFS’s community interest in CCI/AAI as it has occurred after the date of your article.
As of this Feburary (after 1 year of Jen & Jeff’s stories):
“121 people with ICC/CCC ME/CFS have been diagnosed with craniocervical instability, 48 with cervical stenosis, 25 with Chiari malformation (still a common, undiagnosed pathology in our patient population), and 12 with tethered cord syndrome. 25 have been given other structural diagnoses. (Many people are diagnosed with more than one problem, so these numbers are overlapping.)”
This is a shocking number of patients who had zero indication to look for CCI/AAI had it not been for Jen & Jeff’s stories.
I think the craniovascular component in ME is vastly more important than the instabilities that some of these patients suffer from. I think it is a mistake for the vast majority of these patients to pursue stabilizing surgery.
Hi Kjetil,
Could cervical instability be linked to difficulty breathing ( permanent upper abs tension ( at the solar plexus level )) ? TOS ? TMD ?
TOS is more probable
Thanks for the article! Should I be concerned about a misaligned atlas and overall health? If I can freely move into rotation.
If you’re healthy, I wouldn’t worry too much about it. This article is for patients with actual compatible symptoms.
Hello Kjetil, greetings from Bogotá. Colombia. I have an 8mm right rotation of my C2 which apparently is responsible for some of the symptoms I’ve endured during the last year (dizziness, blurry vision, difficulty swallowing), but an orthopedic manual physiotherapist will begin treating me next we through manual mobilizations and strengthening exercises. However, I feel tension in both of my temple muscles daily despite wearing a mouth guard to stop my clenching. My question is, ¿do atlantoaxial rotation could be generating myofascial trigger points? Thank you!
Sorry but it sounds like you’re not on the right track neither with regards to diagnosis nor treatment. Rotations are measured in degrees, not in mm, so this makes me suspicious of how reliable this measurement is. I recommend that you book a skype session and send me your images. I strongly discourage manipulation therapy.
Dear Kjetil
Thanks for this very illuminating article. I have IJV compression caused by C1 transverse process – I suffer from hearing loss, endolymphatic hydrops and tinnitus and recently I have been noticing a feeling of constriction/tightness around my throat at times. As if being slightly strangled. Could this be related? I would like to improve my posture, to help my condition, but with professional guidance so as not to exacerbate the situation. What type of practitioner would you recommend?
Yes, lump in the throat and feeling of strangulation is a common co-symptom in JOS
Hello, Khetil!
What are your thoughts on the thoracic extension stretches? Could they fix kyphosis, combined with thoracic extensors strengthening of course, or should one rather focus on the strengthening?
Keep up the good work!
Only good posture fixes bad posture. Exercises will not fix it.
Hello Kjetil!
I’ve been having these weird cervical instability symptoms for about 5 months now, and recently I’ve been having a click or like a pop when I swallow slightly on the left side of my throat and disappears when it wants, I also feel like my throat isn’t supported and about the fall off when I sleep on my side of the head (both sides) feeling the pressure of the pillow on my side head more.
Don’t know what the problem is and I’ve searched everywhere couldn’t find a hint
Thank you!
I would have to review your images. Book a skype session.
A few years back I was tilting my head and I heard what sounded like rushing fluid coming from inside my neck. Minutes later my neck was frozen and only loosened up after about a week of heat and ice. Ever since then my head has tilted to one side. Lately I have been having really bad neck and back pain as well as TMD pain and tightness but only on one side of my jaw (the side that my head is tilting towards). I’m wondering if maybe years back I could have injured my cervical spine and the symptoms are only now beginning to set in. I will be getting an x-ray soon because the pain and numbness has been very bad lately. Do you think these symptoms could be the cause of cervical/atlas problems? Regardless, I really appreciate all of the material that you’ve published – very informative and thoughtful.
Doesn’t sound particularly sinister
I’ve noticed my SCM muscle is a lot bigger on the right side, is that an indication of a weak muscle that requires strengthening?
Not unless there is compatible clinical exam and symptomology
Hi Kjetil,
My left eustachian tube is patulous (I hear myself breathing and speaking very loudly) + my jaw clicks at the left tmj,
I really feel like my atlas is slightly subluxated, what mri/xrays would you advise me to do ?
Hi, you’ll have to book a session if you want case-specific advice.
With regards to imaging, then brain and jaw MRI is a good start.
Hi my sons and I have Treacher Collins Syndrome. I was very interested to read how posture is connected to the jaw, teeth over crowding and mouth breathing all common in TCS. My oldest son has hypermobility in the atlas joint and as he gets older (35) is now getting back, head and neck pain. Medical investigations can find no cause! but reading your article I think I can see how his TC and poster etc could be causing this. I wonder if you have had any experience of anyone with Treacher Collins Syndrome?
Can your atlas be stuck on one side if you’r jaw is really uneven ?
No
Can you please let me know what mri can should I do before I book the Skype with you?
I have etd/stiff jaw/neck and shoulders tension and pain and sometimes headaches.
These are the available mri in my city:
Full spine contrast/Complete spine native/Cervical spine contrast/Cervical spine native/Dorsal spine contrast/Dorsal spine native/skull contrast/skull native/3D Angiography (skull) contrast/ 3D Angiography (skull) native/ 3D Angiography (limb) contrast MR
And if I need any vascular scans please tell me their names. Thanks in advance and hope to talk to you soon!
Hi — Head CT, neck MRI. Your symptoms don’t suggest a need for any vascular workups.
Hi. Thank you so much for this valuable information. I also have atlas bone misalignment. That’s why I have an asymmetrical nose and misaligned jaw. I have also forward head posture (I think this is the main cause of my atlas bone misalignment) and anterior pelvic tilt. My question is if I correct my forward head posture and APT is it enough to solve my misaligned atlas bone problem? I’m doing some exercises for my posture for a while, I’m trying to keep my head aligned and I feel some little changes but I don’t know if it is permanent.
And I noticed that when I move my jaw a little to the left, my head position slightly improves. But I don’t know if it’s okay to keep my chin like that. At least until I have enough money for jaw surgery.
I wouldn’t pay much attention to that if I were you.
Did you read the article? Of course that’s not enough.
Yes I’ve read your article. It takes time for me to understand compIetely because of my poor english. I have all the problems you have talked about in the article (forward head, pelvic tilt, hunchback posture and etc.). So I understood that I should correct my hunchback posture firstly. But in the sections about some muscles you indicate that some muscles can be tight because they are weak and they need to be strengthened (not stretched). My left scalene muscles are tighter than the opposite side (My head tilts to the left side too and my left eye is slightly higher). So should I strengthen both sides or what?
Always strengthen both sides
When I do suboccipital muscles strengthening exercises and try to keep my head aligned my left SCM muscle tightens and my neck tiltes to the right. Is this normal? What should I do for this?
And when I do chin tuck
Never do chin tucks
Hi doctor Kjetil. I finally managed to fix my forward head posture. My neck hump is gone. But my neck doesn’t look perfectly normal. My SCM muscles look a little bit different. What should I do now? (Atlas bone misalignment)
I’m trying to do your suboccibital muscles strengthening exercise. But I can’t feel very well. I think the upper part of my left SCM muscle is engaging.
I have the same. cant feel the the right deep neck muscles at all. possibly due to a subluxed atlas. since the muscles insert here they become inhibited due to an unstable insertion
I have a problem with hinging when watching TV, in a car or airplane seat. How do I maintain good posture
in those settings? My neck (straight with stenosis) is easily irritated when my left shoulder comes forward, I can feel the scapula protract and muscles (levator scapulae) yank down on the neck. Thanks, you have great content!
More effort
I just paid a good sum of money for an occlusal splint For neurosensory reprogramming of respiratory and postural patterns.
So I was googling and trying to understand what it means and now I’m confused and I hope I haven’t wasted a lot of money I’ll be going through postural therapy. The postural therapy is extra fees not cheap. !!
Plus an ALF For tongue retraining !
The dentist is saying my tongue should be touching the roof of my mouth and it does so I’m confused. I I’ve already spent several thousand dollars with two previous to the doctors the last several years I have lots of radiation pain The back of my head when laying down while I’m upright I don’t have it. It’s just when I flex my neck back.
I won’t lie to much more it’s too complicated.
But I think your article says that this occlusal device is not necessary !!
My impression based on your words here is that you might be misdiagnosed. Doesn’t sound like a TMD problem
Hi Dr. Kjetil. I am 29 y.o. 185cm and 60kg, all my life with very bad posture due to laptop/cellphone/stress and suffering IBS with intermittent migraines since child, and dental malocclusion. Neck always stiff and practicing self-pop, haven’t practiced sports since 17yo. January 2021 I had a severe vertigo attack, which resolved but left me dizzy and with chronic tinnitus. This summer intense back and neck pain have appeared along with more dizziness and a lot of spontaneous cracking and popping around thoracic-cervical spine. I started a regular chiropractic who practiced violent neck twisting, then I suffered brain fog, blurry vision, mores instability, etc. I have changed to an Upper Cervical chiropractor, who ordered x rays. It showed that my c spine is almost straight but hinging backwards at C1 and C7 where a discal protrusion was found in previous MRI. The upper chiropractor found atlas misalignment, and after getting 2 atlas knee-bench adjustments (last one with loud cracking) I feel a worsening of all symptoms (dizziness, tinnitus, TMJ, neck tension, blurry vision, instability). After learning from your articles, which are great, I think I might have some degree cervical instability, which chiros adjustments I think are making it worse. I now think about quitting the Upper Cervical Chiropractor and stating to implement your advice. Do you think is it a good idea? I don’t want myself to get hurt. Maybe by doing that I could save money and book you a call. Thank You so much in advance!
I strongly discourage any kind of neck manipulation approaches in general
Dear Dr Kjetil,
I was diagnosed with Chronic RA in the C1/C2 region some 16 years ago and have lived on Tramadol since.
2 years ago I got Cortisone injections from C1 to C7 and it stopped the pain. The I got an Ablation. The pain stopped for almost 2 years and it was good.
HOWEVER, I started getting serious headaches at night. These headaches originate from my neck ABOVE my RA. The pain radiates to my entire back of head and sometimes to my eyes. It is seriously crippling pain. [7 -9]
I can NEVER lie on the back of my head and must always lie on my side. This pain has now become regular at twice weekly.
While I am writing for an appointment with my Neurosurgeon I will ask a question.
I bought a cervical collar 2 nights ago and so far it seems to work as I woke without that ‘threatening tingle’ in my neck at C1 or C0.
What neck brace would you suggest?
Thanks from Australia
I don’t recommend a neck brace at all.
Marcel, my name is Sam. I too suffer with debilitating chronic migraines. Please drop me an email, [email protected]. It would be really helpful to have someone who is experiencing similar, and have gone through the same process, to talk to.
Hey man how are you doing now? What have you done sincr then?
My story is very similar to yours..
Have you ever seen a patient with extreme sensitivity to upuward/downward forces? Since an accident, my c1/c2 was injured and I must walk on my toes, as i can viscerally feel any sort of heel contact on a hard surface in my upper neck/head. This has caused me to walk with soft soled shoes and take on a lot of maladaptive movement patterns. I also have a slew of neuro issues. Feels like brainstem compression. Does any of this sound familiar? Looking into booking with you once my images are delivered to me.
Depends on what symptoms we are talking about, but either spine or CSF pressure are my first thoughts. Need a full imaging review and a better explanation of hstory and symptoms
I have severe occipital neuralgia. I’m in North Carolina mountains USA.
I WILL PAY AND FLY TO YOU FOR HELP!
I’m at the end of my rope here.
Come on down. I think a skype consult would be sufficient though, if you only have ON and nothing else.
Hi Kjetil,
I have had this strange postural issue for about the last decade, that I think might be due to atlas joint stability or something similar. I have seen multiple healthcare professionals but they don’t know what is wrong with me. However, I know the specific posture that caused the issue and some of the symptoms which may give you an idea of what could be the cause. I cannot express how much your help will mean to me as I have been trying for years to solve this issue with no luck. The issue started around 10 years ago when I first got an iPad. I would spend multiple hours per day lying in bed with this specific posture that I think caused the issue: I would lie down with the iPad on my chest, I would then rest my head against the backboard of the bed or armrest of the couch and look at my iPad on my chest. After many months of doing this daily I developed very strange symptoms. The most noticeable symptom was my eyes and jaw area. The upper eyelids above my eyes were far more noticeable, which make my eyes constantly look droopy/sleepy and my eyes looked like they were bulging out a bit. The hyoid muscles under my neck look visibly tight, and my side profile looked recessed almost. Another strange feature that popped up during this time was a bump the size of a grape right where the nuchal ligament inserts (i think this is because of bone remodelling due to increase stress on the ligament). I also started having issues sleeping with my eyes open. None of these issues were originally noticed by me so I know it wasn’t me imagining them suddenly. The aesthetic implications were so great that I have had cone beam scans on my skull and MRIs on my eye area. One specialist thought I had maxillary hypoplasia, but to his total surprise the bones of my skull are developed perfectly normal. An eye specialist thought I had proptosis of the eyes, but every test back came normal (MRI, blood tests, etc). The hertel measurements were also normal (distance eyes protrude from skill), but since it looked as if I had proptosis he diagnosed me with pseudo proptosis. There were minor things that came back from the 3d skull scan that I think are relevant to this issue. 1) Pansinusitis and 2) TMJ. When I go to the dentist, I have difficulty keeping my mouth open and have a burning pain after a few minutes in my TMJ area. When I tilt my head to the left I have noticeable tightness in my levator scapulae, to the point where it is clearly visible during the tilt. Also, when writing a test or doing a task where I am looking straight down, I get a burning feeling in my cervical extensor area after 10 minutes or so. When rotating my head I also feel tightness. Also, if I extend my neck I start to get tingling in my hands and fingers after about a minute or so. When I am standing up the scalene area of my neck is very tight, which I know is common for neck stability issues. However, here is the strange thing, if I lay down supine and place a book under my head (couple of inches) my eyes/jaw area look completely different (what they looked like before this issue) and there is no tightness in my neck. Please let me know if you have any idea what could be the issue, you have no idea how much it would mean to me.
Apologies, I don’t have time to read all this.
These people commenting on your article are all suffering severely (myself included), you could potentially be lifechanging to them. Make time!
What are you talking about? I wrote this article and it’s free, all my online material is for free — and I should also “make time” for free consults? I try to get back to most of you but I don’t have time to read super long comments; it is what it is! Get real and go elsewhere with your entitlement problem.
agreed, thanks Kjetil for the info – I might soon have figured out all my issues thanks to your free resources!
I just left a comment that I hope isn’t too long, sorry! I fully understand.
Thanks for sharing! Great article! Very insightful.
What do you think about prolotherapy injections to accelerate/help muscle restauration? also used to strengthen ligaments.
Could this be a good complement to muscle training/AA-CC stability?
The actual question was, would you use prolotherapy as a complement for a subluxated atlas that keeps being knocked out?
Prolotherapy can be helpful if there is pathological instability that is at the borderline for surgery. The atlas, contrary to popular belief, doesn’t “knock out”; it’s not a ball joint or socket. It is a gliding surface, and muscular integrity / pulling forces and postural integrity is mainly what holds it in place. There are some exceptions for this. In most cases, no, I don’t agree that this will help.
Thanks for this info. it makes great sense!
When you claim that the first step would be atlas correction (if viable, i.e if the patient is cleared to do so) what you actually mean?
You also said you are against any manual correction or manipulation. So i’m confused.
How would you correct the atlas in a safe way without recurring to any upper neck specialist?
The atlas correction is really something that I don’t use a lot, almost never. The notion that “atlas correction” is the main treatment for this problem should NOT be the take-away from this article. There are some few scenarios where I may attempt it, but the results will generally not last even if the “correction” is successful. I just removed it from the article (the article is 6 years old). The reality is that these horizontal misalignments that occur at the upper cervical spine are not really something that you can “pop back into place”, as many mistakenly believe. The gliding that occurs, it happens due to poor posture and weak neck muscles, and it happens over the course of years. The solution for this problem is to optimize neck posture and to aggressively improve strength and capacity of the longus capitis, levator scapula and suboccipital muscles.
“Atlas correction”, for all who are reading this, is largely a scam business.
And quite well functioning one as I’ve managed to grasp 🙂
Great article!!
You think Regenexx which you mention here – could help to speed up the recovery process with PRP/PICL injections while practicing good posture and doing the muscle exercises?
Or should this be used only to avoid surgery in severe CCI/AAI cases?
Is there any device/technique/practice out there you recommend to speed up the strengthen of muscles from “the trio of success”?
This is too individual to be able to give casual advice on it. I rarely refer someone for prolotherapy, mainly because I feel that some of these clinics have a poor understanding of what CCI really is, and they tend to overdiagnose it even to normal patients.
Now, if there are serious deviations found on imaging that is of non surgical degree, I may recommend prolo to avoid deterioration. It doesn’t really speed up any processes as far as I a concerned, as these processes are generally not dependent on the ligaments. Pathological CCI with neurovascular conflict will generally require surgery.
Hello Kjetil. I had a moderate occipital neuralgia but after chiro neck manipulations sessions, in a month I got bedbound from the headache/heavy head. Now I have severe muscle atrophy at c2/c3 as seen on MRI (suboccipitals maybe?). Do you think that the chiro neck cracking had damaged more my ligaments or muscles? I can stay upright around 3h a day and have severe loss in range of motion.
Ligaments, doubtful but possible. Muscle yes
This is the most comprehensive article I have ever found regarding ALL the issues that can go wrong in the neck.: Many of which I have had for two decades. Probably much more.
However, I have reached a level and age (68) in which I feel I need to know in more detail exactly what my damage is, some of which I know.
I had a cervical fusion, not an option, at age 50, at C5/6 which resulted in a serious nerve root injury (surgeons fault) and woke up in so much pain that my career (artist/designer) was immediately over, as well as my ability to exercise.
I have been treating this and continuing disintegration of all cervical areas, as well as cervical instability and damaged cranial nerves for many years although I have not been treated by anyone other than my prolotherapist.
He is the top in his field and has kept me somewhat stable but I do have to go three times a year. Especially in the past two years, as he learned ultrasound guided hydro dissection of the C1 and C2, which has afforded stability of the head, and regular prolotherapy for issues with my mid and lower back, which at age 68, I do not consider to be my primary concern.
I have been so afraid to exercise up until now. My neck was feeling really good until a recent bout with Covid fried all the nerves, so to speak, and everything came back overbite and am dealing with this now. Very disheartening.
I am alarmed by all this information, especially since , after a 10 hour dental procedure in 2019, got what I am certain is Cranial Instability, which I never had before. I could not even walk for 2 years because my head felt utterly unstable and my neck muscles were choking me. I am very grateful that the prolo and the hydro dissection helped.
However, he does not use any imagery other than ultrasound and the patients pain report.
I live in So. California and wanted to know what kind of doctor do you feel is most appropriate to evaluate my disabling condition with either MRI, CT, and or ultrasound. Many doctors say if you don’t want surgery, you don’t need imaging. But, how do I know I don’t have something t serious, or bordering on serious, as my cranial nerves are causing issues as well. Can ultrasound see tumors, or other concerning elements in the brain? I don’t think so. The pressure and pain is immense at times, and I have had to rely on pain medications as well for may years.
Additionally, and probably very important : I have a soft tissue disorder caused by an extremely adverse reaction to fluoroquinolone antibiotics: Cipro and Levaquin, rendering me housebound mostly for over 5 years. Although I had taken it before, as many others have, but did not know anything about them.
These drugs have played a part in the condition of my soft tissue deterioration, including a large spontaneous ankle rupture from the same drug in 2010, which I had no idea what it was from.
I am starting to add some cranial and other exercises, slowly, to see how these help. My posture needs support and I am focusing on that now but would appreciate any advice as to what kind of MD could evaluate this area to make sure I don’t have anything more serious. MD image referral is the only kind medicare will pay for, and I am far too afraid to go to a chiropractor, or PT, as I have such a multitude of issues, and without imagery might hurt myself further, which I cannot afford!
I want to be stronger and mobile, and fully appreciate all the information you have imparted here and will study it very closely.
I will also send this article, or your website, to my prolotherapist.
Thank you.
Hopefully I might find someone as knowledgeable as you.
I have an orthopedic doctor for bilateral achilles tendonosis( thank you Levaquin in 2017 while travellng for a simple UTI, walked 15 miles in Rome, came home, and the next day couldn’t walk. for a year and a half and still can only walk for 15 min…. among many other disabling symptoms), and this orthopedic doctor does not use imagery either.
So it’s a challenge to find an MD who will fully evaluate me with imagery. Medicare will only pay for it if it is an MD. Neurologist, or?
Do you know about Fluoroquinolone damage to soft tissue?
Again thanks for everything. You are brilliant! I think with solid imagery, I could get better safely.
Deborah Goodman
Sorry for the too long comments. I just want to know what kind of imagery I need and what kind of doctor would order it. I would Skype you afterwards.
Sorry I don’t have time to review this amount of backstory outside of session
I’ve been reading through your article and have found it to be a real eye opener. I’ve been suffering on and off with symptoms from a severe concussion back in 2014. While I’ve done many things for my recovery I’ve never felt 100% due to, what I believe have been issues with my neck. Now, this past year after having a lot of new symptoms appear out of nowhere, I have been seeing a Chiropractor who has been using a sound device to gently push my atlas back into position. The alignment seemed to be taking after several sessions, but then I hit my head again unfortunately and now it’s been even harder to maintain the alignment after a session. I seems that you don’t believe in this method from what you said above and I’m interested in strengthening the muscles and ligaments as you suggest. I’m a little overwhelmed at what to do and a little scared of just doing the exercises myself. Is there a way that I could book a Skype session with you sometime soon?
You’ve saved my life!! It’s an amazing article. I really appreciate your elaborate and insightful research work. I have got a really complex and pour alignment from cranial bone to feet after having orthodontics with four molar extraction, though I have a lot of asymmetric bones with my birth.(scoliosis, pronating feet, bone length asymmetry on saggital plane, deviating TMJ and A-O joint subluxation after each chewing) So I have difficulty to get back my tensegrity after each chewing, though I try to correct it using some corrective techniques. Your insight shed light on my practice routines for it and help me get it back more comfortably and safely. Thank you so much. I hope you don’t forget your elaborate efforts save so many lives. Many blessings to you!!
I’ve got a strong feeling that my maloclussion (bite hangs out to the left when I bite) was the beginning of my bad posture and atlas instability.
Are the pterygoid muscles the most important in this? How to balance those muscles out? I dont feel like massaging those is enough, so what would you say about orthodontics to center the bite?
So, I’ve got 3 of your YouTube excercises for the neck muscles. Are those 3 the ones I should do? My C1 is twisted to the left so the right side is forwarded. Should I do the excersice levator scapulae only on the right side?
https://youtu.be/zH7O-7sfHTY
https://youtu.be/yRMCI6xnxAw
https://youtu.be/Q43oMCJfFN0
Do you believe in scoliosis treatment using muscles as leverage? E.g unilateral strengthening of psoas for lumbar scoliosis, or rhomboid for thoracic scoliosis?
I doubt it’ll work but I guess it has some theoretical plausibility. There are various theories regarding the origin of scoliosis
Oh okkk, do you think (or have seen in your patients) that pulling atlas in correct position can make spine “unwind” and go to correct position, if for example scoliosis came from craniofacial/malocclusion problems (if of course this is really origin of scoliosis)?
Dear Mr Larsen,
I love your articles. I had endless off the charts migraines after a whiplash about 15 years ago. I do not totally agree with you that( conservative )atlas adjustments do not work. They gave me immediate relief. However i do agree that endless adjustments are not the answer long term. I do believe you are right about posture & strengthening the muscles that are trying to compensate for the now lax ligaments damaged in the whiplash. Sometimes now when my atlas is out it self adjusts but sometimes it just will not without the adjustment. I also wear a neck brace to bed because though i only sleep on my back it seems i can not trust what my neck is doing while i sleep & so i was previously waking up early with a migraine every morning. The muscles never felt like they got to relax during sleep because they were trying to control what my neck was doing all night. The neck brace gives my neck a chance to relax at night.
Kejtil, what do you think of curve correction therapy through CBP (chiropractic biophysics tools), they use a daneroll device under neck, neck weights and some other machine.
Hi Kejtil,i have sth to consult u,it makes me being suicidal.And idk whether your business includes ETD or not,so i want to post a long comment here,if u do have some clues to help me,pls let me know,i will be very very grateful~Off course,i will book an appointment with u,i will pay no matter how much it would cost.
Let me explain mewing briefly and firstly:
Mew can basically be understood as placing the tongue behind the upper teeth for a long time and pushing the palate forward and upward. Soft mew should not apply any force, but sometimes i overdo it and apply extra force. I doubt it squeezed my Eustachian tube and the muscles surrounding it.
I started mewing since 2020 late,for i used to breathe with my mouth sometimes,after seeing mewing videos i wanted to adjust my tongue posture.Sometimes i even do hard mew(applying pressure to my soft and hard palate and swallowing only with my tongue forcefully. )
Since the summer of 2022,i realized that sometimes when i swallowed or even spoke,i could hear a rattling/clicking sounds,a bit like the sound of bones rubbing together.And it didnt sound loud,for me it’s acceptable.But coincidentally,there was one time during that time when i couldn’t open my mouth suddenly which never happened to me before.Within a few days,i was struggle to open my mouth when i had my meal.But fortunately the mouth problem went away after few weeks.
But the cracking sounds after swallowing and speaking never went away.They just occur less frequent after i wake up.
Last month,i found that sometimes after swallow,apart from cracking sounds,now i could hear a sort of popping sounds as well(though i had it before,but it sounds more louder than usual and they were more frequent).Its the sound that you can hear when you take a flight(altitude changes),and i just realized i got tinnitus.(a bit like the sound of electricity flowing).I went to see a ENT Dr but it seemed he didn’t have any ways to fix it.He just prescribed me some medicines then send me home.
Well I know the popping sounds are normal in science,but as i said it did sound louder than before.It’s very annoying that they showed up when i used earphone.(Forget to mention,i used headphones quite often in the past few months and slept late,and i had some anxiety.)
I quit headphones very soon.
After the first Dr,i visited a new ENT Dr who arranged a TMM check for me(To check whether your eustachian tube is normal or not).And he found mine did have problems for Both ears.(R≤1 means the tube open normally,R>1means the opening is delayed,0 means open activity wasn’t detected).The report showed my both ears basically were 0.Again,he prescribed some medicines,and nasal spray this time.
I have taken those medicines up till now,i wont say it doesn’t effect at all,but generally the improvement are extremely slow,i still have ear fullness sometimes,and popping sounds after swallow.(Sometimes it still hurt a bit).Sometimes my ears popping of its own accord when i didn’t do anything,the sudden airflow impact hits me really,it could be scary and painful).
Off course,the rattling sounds after speak never went away,i could also initiate them by moving tongue.This is another sound, not that sort caused by the Eustachian tube. I guess it is a muscle spasm near the Eustachian tube, or something went wrong after being squeezed. In fact, the sound source seems to be in the direction of the neck.
Now what i wonder is that are there any ways to reverse hard mewing effect?I saw a post,
https://wholebodybreathing.com/community/main-forum/tinnitus-from-mewing/#post-38250
It said people can pull the palate downwards by tongue which is opposite to mewing(Well my understanding for mewing is about pushing your palate upwards and forward.It does sound reasonable but i have no idea whether it will bring more troubles to me,i cant take it anymore,these 3 mouths are hell. I got intense popping even when i drink,i can only alleviate the frequency by using a straw.
I have lost a lot of weight in the past 3 months because eating is no longer a purely enjoyable thing for me.Because I am afraid of swallowing, I have to bring a cup when I go out and spit it in when I want to swallow, but avoiding swallow for a long time will aggravate my ear fullness.
I have lost a lot of fun in life. I am only 27 years old now. It is hard for me to imagine that I have to live like this for the rest of my life. My guess is that mewing messed up the muscles or tissues near my Eustachian tube and may have squeezed my Eustachian tube. , I don’t even know if these effects will be permanent or if there is any way to fix them.
I went for an MRI and there was nothing wrong with my TMJ joint.
I went for a spinal checkup and there was something wrong with my spine, the hole between my spine was narrowed, the doctor said my spine was not good and prescribed some medicine,also suggested me to keep a good body posture.But I thought I’ve had this spinal problem for a long time (Although diagnosed for the first time), it may have been several years, but i dont think it caused my ear problems.
Best wishes for you,Kejtil.
Hello Roger,
I am neither a medical professional nor a patient of Kejtil (I might be in the future). I don’t think I have any helpful information to give you but I too caused problems for myself with forceful mewing. I thought my dental misalignment would need extra effort for me to see any change since I am older so I tried to add extra pressure on my palate. Thank you for writing this post. I think it makes it more probable for me to have caused my issues with mewing and not anything else. Unfortunately, my problem might have reached a stage that is way more advanced than yours. I have a crackling sound and salty water in my mouth and I think I may have caused a cranial CSF leak that is not healing on its own. I don’t mean to scare you as our problems could be different. CSF leaks are difficult to diagnose, (even with the most accurate and risky imaging techniques) and they cause many problems. If I may suggest something, perhaps you should do a thin sliced CT of the skull. There is something called the Stealth Protocol, which I believe is a generalised CT scan of the head that might reveal certain things. You would need to find a good specialist to read such a scan and know what to look for. A skull-base ENT surgeon who is trained in spotting CSF leaks. Again, I do not mean to scare you or misguide you, take anything I say with caution. I am still trying to find what is wrong myself as the country I live in does not have anyone skilled enough to spot CSF leaks. They are a rare breed of doctors worldwide. I’ve also done MRIs of the brain and cervical spine and found nothing of significance. According to my CSF leak support group, doctors are generally not trained to spot leaks. Both specialists and leaks are difficult to find.
I am not sure what you meant by saying that the hole between your spine has narrowed. Could you possibly clarify?
I hope you are feeling better or at least have not worsened for you since you posted. Take care.
Hello sir I have this weird feeling of lump in throat and tightness in neck. Also this leads to lack of concentration in my studies. This feeling is often when my neck is in stable upright position. So can these exercises help me. My neck x-ray is normal..
Hi I was wondering if an elevated first rib can cause atlas issues or vice versa? Also can it pull on temporal bones and if so what would be a good fix? I did a self adjustment of first rib and feel relief and look different as well. Just wanted to see if there was any correlation that youre aware of? Thanks you
Kjetil are you a chek practitioner?
BR
Bruno
Hi Bruno. No.
I have pain in my neck, pain in my face, pain around my eye, a sore throat, and a feeling that something is stuck in my throat
Could my tireóide cartilage ( I have a prominent Addams apple) press on nearby muscles or tissues, especially when swallowing or moving my neck?
Or I have muscle tension, meaning my neck muscles are overworking to compensate for local sensitivity.
It could either be thoracic outlet syndrome, or impingement of the vagal or glossopharyngeal nerves at the upper neck. IF it is truly an MSK issue, that is.