The presence of non-discogenic lumbar plexus neuralgia, also known as lumbar plexus compression syndrome (LPCS) is a virtually unknown and thus relatively unmentioned cause of thoracolumbar, lumbopelvic, and femoral pain. It is sometimes also referred to as Maigne’s syndrome, posterior rami syndrome and thoracolumbar junction syndrome. To some degree, this may also be true for similar lower extremity entrapment syndromes. They may often appear, falsely, to be a simple groin, hamstring or quadriceps injury of muscular origin, and thus end up getting treated inappropriately. This article will attempt to shed light on its signs and symptoms, and my approach of identification as well as treatment.
Nerve entrapment syndromes of the lumbar plexus are a rare but important etiology that should be considered when evaluating athletes. – Rassner, 2011
Entrapment of the lumbosacral plexus is an under-recognized cause of lower extremity, pelvic, low back, and abdominal pain; because of the wide variety of entrapments, there can be a wide variety of potentially confusing clinical presentations. The clinician needs to have a high index of suspicion to diagnose and therefore treat psoas entrapment of the lumbosacral plexus. – Anderson-Jones et al., 2016 – Lumbar Plexus Entrapment: Lower Extremity
The patient was diagnosed with thoracolumbar junction syndrome and treated with conservative methods. Thoracolumbar junction syndrome is a pathology that should be considered in the differential diagnosis in elderly patients with low back, hip and groin pain. – Aktas et al., 2014
Thoracolumbar junction syndrome is characterized by referred pain which may originate at the thoracolumbar junction, which extends from 12th thoracic vertebra to 2nd lumbar vertebra, due to functional abnormalities. Clinical manifestations include back pain, pseudo-visceral pain and pseudo-pain on the posterior iliac crest, as well as irritable bowel symptoms. – Kim et al., 2013
This case report describes a 46-year-old female who experienced symptoms of low back pain with pain radiating into the right gluteal area. The thoracolumbar junction is described as a predominant contributor to the symptomatology. Its complementary role to the lumbosacral junction is enumerated. – Sebastian, 2006
A frequently overlooked cause of testicular and buttock pain is irritation of the T10-L1 sensory nerve roots, the genitofemoral nerve, and the ilioinguinal nerve. – Doubleday et al., 2003
The thoracolumbar syndrome is a potential cause of back pain in athletes whose sport involves prolonged posturing with the hips flexed and the head extended upward. This syndrome may be overlooked and athletes are sometimes inappropriately treated for an incidental finding in the lower lumbar spine disclosed on conventional imaging studies. The clinical presentation involves point tenderness over the affected motion segment (T12 through L3) with pain radiating along a segmental nerve distribution (anterior or posterior rami divisions) of thoracolumbar origin. – Fortin, 2003
The author describes the clinical findings of the posterior rami of the spinal nerve syndrome (R. Maigne) which innervates the skin from the vertex down to the coccyx. Moreover, he reports the cutaneous trophic changes which occur during the suffering of the anterior rami of the spinal nerve. He gives, for example, the sufferings of the T12 rami which are at the origin of the major diagnosis errors. – Rageot, 1982
Fig. 1

Myofascial compression of the lumbar plexus can cause many diffuse symptoms, due to its innervation spreading from the stomach (and I hypothesize; even into the abdominal autonomic plexuses) and all the way down into the calf. To understand the reason why this may occur, you will have to understand the course of the lumbar plexus nerves, as well as its surrounding myofascial anatomy. Solving LPCS requires a holistic approach to posture, breathing, and of course muscular assessment, function and correctives. But first, let us talk about what I consider the cause of myofascial nerve entrapment.
DISCLAIMER: This article is written for educational purposes only
The cause of myofascial nerve entrapment (MFNE)
Nerve entrapment syndromes have become quite controversial. Many claim that nerve entrapments are very rare, and almost never the cause of the patients’ pain syndromes, but rather that psychological factors are causing the patient’s diffuse pain. Others acknowledge its existence and do not doubt its common frequency, but because no concrete diagnostic nor treatment criteria exists, differential diagnoses will almost always be investigated and pursued instead.
Here is a relatively small quote-collection. A tremendous amount of papers have noted the controversy regarding nerve entrapment syndromes.
Pudendal neuralgia does seem to exist as a clinical syndrome rather than a specific diagnosis. It is important to note that it does not have definite etiological implications, and there is no evidence to support equating the presence of this syndrome with a diagnosis of pudendal nerve entrapment although that may be 1 etiological condition. – Stav et al., 2009
Piriformis syndrome, sciatica caused by compression of the sciatic nerve by the piriformis muscle, has been described for over 70 years; yet, it remains controversial. It could be argued that there is no value in making a diagnosis where there is no proven treatment. – Hopayian et al., 2010
However, little agreement exists on which muscles need strengthening and which ones need lengthening. – Vanti et al., 2007 Conservative treatment of thoracic outlet syndrome
This article is concerned with thoracic outlet compression syndrome (TOCS), one of the most controversial subjects in medicine. It may also be the most underrated, overlooked, misdiagnosed, and probably the most important and difficult to manage peripheral nerve compression in the upper extremity. – Atasoy, 1996
The diagnosis of saphenous nerve entrapment is a difficult one to make and is met with controversy within the literature. Due to the rarity of saphenous nerve entrapments, little is known on the prognosis or natural history for these patients. – Porr et a., 2013
The diagnosis of piriformis syndrome is challenging, as the symptoms are often nonspecific and electrodiagnostic tests are difficult to perform due to the deep location of the nerve. Imaging diagnosis of piriformis syndrome is similarly problematic. – Petchprapa et al., 2010
There is no significant disagreement about the major common entrapment neuropathies, such as carpal tunnel syndrome (CTS), ulnar neuropathy at the elbow, and peroneal neuropathy at the knee. In contrast, there is a group of entrapment syndromes about which there is major disagreement, including whether or not they even exist. There are other entrapment syndromes about which clinical questions arise on a regular basis, and which are the subject of this discussion. These include thoracic outlet syndrome, radial tunnel syndrome, ulnar nerve entrapment at the arcade of Struthers, piriformis syndrome, and tarsal tunnel syndrome. – Campbell et al., 2008
Tarsal tunnel syndrome is an entrapment neuropathy of the posterior tibial nerve or its terminal branches within its fibro-osseous tunnel beneath the flexor retinaculum on the medial side of the ankle. The condition is frequently underdiagnosed leading to controversies regarding its epidemiology and to an intense debate in the literature. However, management of this entrapment neuropathy remains challenging because of many intervention strategies but limited robust evidence. Uncertainties still exist about the best conservative treatment, timing of surgical intervention, and best surgical approach. – Doneddu et al., 2017
Obturator neuropathy is a difficult clinical problem to evaluate. – Tipton, 2008
In sports medicine, chronic hip, groin and buttock pain is a common diagnostic problem. Because of the complex anatomy of this region and the many potential neurological causes for pain, few sports clinicians have a detailed understanding of this problem. – McCrory & Bell, 2012
The clinical differentiation of ilioinguinal, iliohypogastric and genitofemoral neuralgia is difficult, frequently resulting in misdiagnosis and inappropriate treatment[29,30]. – Hakeem & Shanmugam, 2011
Now, if nerve entrapment is, identified and diagnosed, which is somewhat rare, at least in my country, another great obstacle presents itself; there is no known treatment for these issues. Even relatively simple aetiologies such as piriformis syndrome is considered very controversial and also difficult to treat. Surgery may be attempted in order to resolve various nerve entrapment issues, but has very unsteady success rates. The reason for this, is that the region of the symptoms may not always be the region of entrapment, as you’ll learn more about throughout this article.
My own experience working with myofascial nerve entrapment syndromes have left one point very clear; the muscles that are entrapping the nerves and causing the neuralgic responses, are almost always severely weak. I strongly consider this fundamental factor to be the main reason why nerve entrapment syndromes are considered so difficult to treat. It took me some time to realize this, mostly because I was greatly influenced by the therapeutic consensus, which creates a strong desire to perform myofascial release on just about anything, and especially when it comes to nerve compression issues. After I was introduced to manual muscle testing (MMT), I gradually started to see am undeniable pattern of inhibition, which means neurological inactivity (i.e. muscle does not respond reflexively to loading), as well as pure weakness of the muscles surrounding the affected nerves.
Fig. 2

I kept performing myofascialrelase for a while, but my patients with various MFNE were improving just marginally (temporarily), or not at all. As an experiment of sorts I tried to strengthen those muscles (scalenes on a TOS patient), but the patient became significantly worse (also temporarily) and I got cold feet, and therefore discontinued the strengthening work. After some back and forth I speculated that the extremely low work capacity of the respective muscles causing the compression, could be something that had to be corrected gradually, and that temporary increase of symptoms was a necessary and unavoidable part of the rehabilitation process. I told that patient that we were going to retry the strengthening, but this time very gradually to control the symptoms. The patient agreed.
After a few months of gradual strengthening work, and of course as well as postural, breathing-corrective procedures, the pain resolved permanently. After this, it became increasingly quite clear to me that severely inhibited muscles indeed become very tight and abrasive, greatly increasing their potential for myofascial nerve entrapment. After this incident, the above was confirmed again and again in my clinical practice.
Garrick and Webb in their excellent book, Sports Injuries: Diagnosis and Management, state that a weak muscle is a tight muscle. Whenever a weak muscle is forced to work beyond its capacity, it will tighten and, therefore, be more subject to stress and strain. – Warren Hammer, 1990
I am now, after treating hundreds of these patients, left with no doubt that it is a huge misconception that myofascial nerve entrapment is caused by “over-active” muscles, and that these require myofascial release to let go of the nearby nerves.
For further anecdotal proof to these claims, you may also look into the evidence of TOS, which is very similar to LPCS; there is no known cure, nor any consensus with regards to treatment protocol, as mentioned above! Secondly, try to find a single person that has permanently cured their chronic myofascial nerve entrapment by stretching, massaging or any type of isolated release work. It virtually never occurs. Another good and similar example, which I also briefly touched upon above, is the infamous piriformis syndrome, where the sciatic nerve gets entrapped between the piriformis and obturator internus. I have never seen a single patient with this problem that had a strong, functional piriformis muscle upon MMT. Their desperate efforts had just been making the issue gradually worse, by straining the weak and unhealthy hip rotators with excessive myofascial release protocols.
In reality, the weaker a muscle becomes, usually due to an underlying postural or movement-related dysfunctions, the less amount of work it is able to handle. When such a muscle, for example the psoas major is exposed to a situation where it’s forced to work like running uphill or bicycling (or similar stress, like continuous myofascial release), it can not cope with that load, and may eventually enter a state of chronic inflammation. This will of course affect all of the nerves that pass through it, such as the lumbar plexus, as they will get stuck within the tight and restricted muscle’s fibers and fascia.
Some may argue that if the muscle is weak, shouldn’t it get stronger when it’s being used? The answer is; it depends. Once a muscle enters a severe state of inhibition and weakness, it’s tough to rehab it. It must be done by very light work loads, to gradually increase its work capacity without overloading it. Frequent overloading will cause regression and exacerbate the weakness, causing a negative spiral.
An important study in the fascial world by Langevin et al., 2009 proposed that people with chronic and recurrent low back pain had 25 percent greater fascial thickness than a low back pain-free group. Another study in Skeletal Radiology, 2005 (Richards et al) found that pathological Achilles tendons showed increased thickness and 89 percent were painful. Furthermore, there was found a correlation between the intensity of the pain and the thickness of the fascia compared to the control patients. The dense-collagen type I fibers remained the same, while the loose connective tissue demonstrated increased GAGs and hyaluronic acid. (Stecco, 2012)
Fig. x
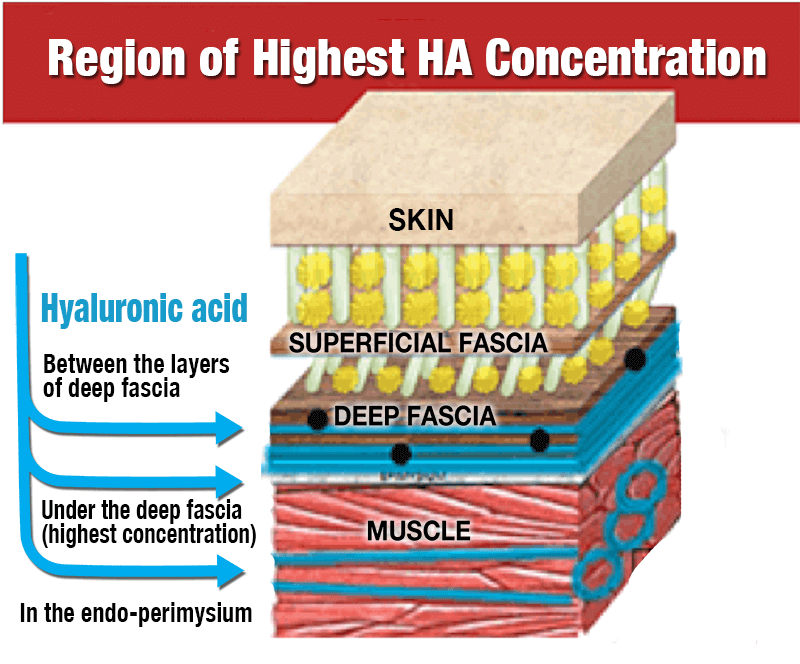
Based on the above studies, and of course my own experiences, I believe that lack of fascial glidning (i.e entrapment, and not true mechanical compression) is the pimary cause of common nerve entrapment issues, and that the fascial buildup occurs as a compensation when the muscle is overloaded, i.e has an inadequate work capacity and can not cope with the load imposed upon it, whatever it may be. Once the muscles are strengthened and their work capacity is adequate compared to imposed loading patterns, the fascial hyper-rigidity will cease and proper structural gliding is restored. The nerve entrapment and accompanying pain will be gone. Stecco et al uses massage to reduce the hyaluronic acid build up that restricts fascial gliding, but personally I do not find this to provide lasting results. Strengthening and restoring muscular health, however, can and will give lasting results. I have seen it time and time again.
A small summary must be done from this subheading, as my protocol is based on these principles:
- A severely weak muscle usually is a very tight and unhealthy muscle
- Inhibited muscles are almost always responsible for myofascial nerve entrapment, not strong and “over-active” ones
- A severely inhibited muscle must be strengthened gradually, starting with a very light load
- Performing myofascial release on an inhibited muscle will make it worse
Imaging and neurographies
It is known that signs of periphreral entrapment is difficult to visualize on MRI. A systematic review by Kwee et al. (2014) states that MR Neurography for detection and diagnosis of nerve entrapment neuropathies has a low sensitivity and specificity, and that its use in clinical decision making should be used with great care.
Further, with regards to diagnosis of plexopathy and/or peripheral nerve entrapment neuropathies, it has been shown that EMG, NCV and SEP studies are not reliable diagnostic criteria (Tolson 2004, Passero 1994, Veilleux 1988, Aminoff 1988, Rousseff 2005) There have also been reports of EMGs only being positive when the patient is in certain positions (Fishman 2002), and reports that motor nerve NCVs have been negative while sensory segments positive (Machanic 2008). Said et al. 2018 found that only 55% of patients diagnosed with piriformis syndrome had positive NCV tests, however these numbers may be grossly overestimated, as the very same patient group underwent surgery, suggesting that the symptoms were both severe and conspicuous in nature. I have seen several patients with severe pain upon pressure to the interscalene triangle, positive myotome tests etc., who still did not have any findings upon EMG. The sensitivity of these tests are simply inadequate and should not be used to exclude pathology. They may be used to quantify the problem, once already implicated, however.
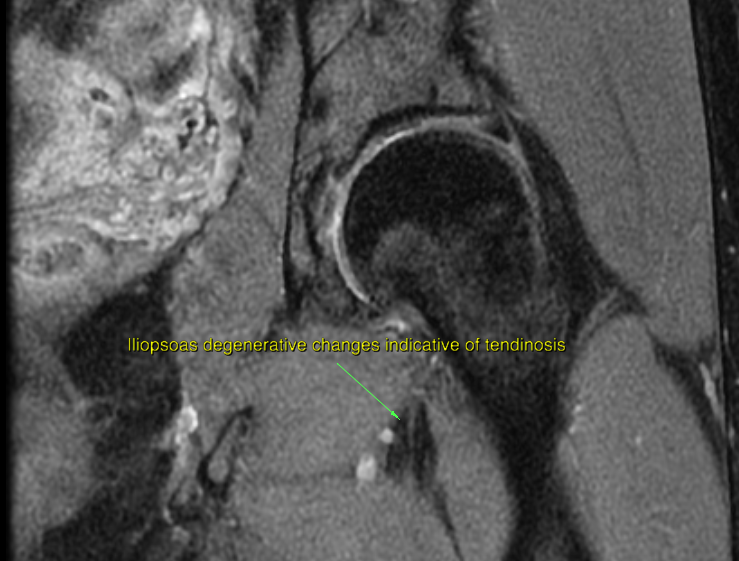
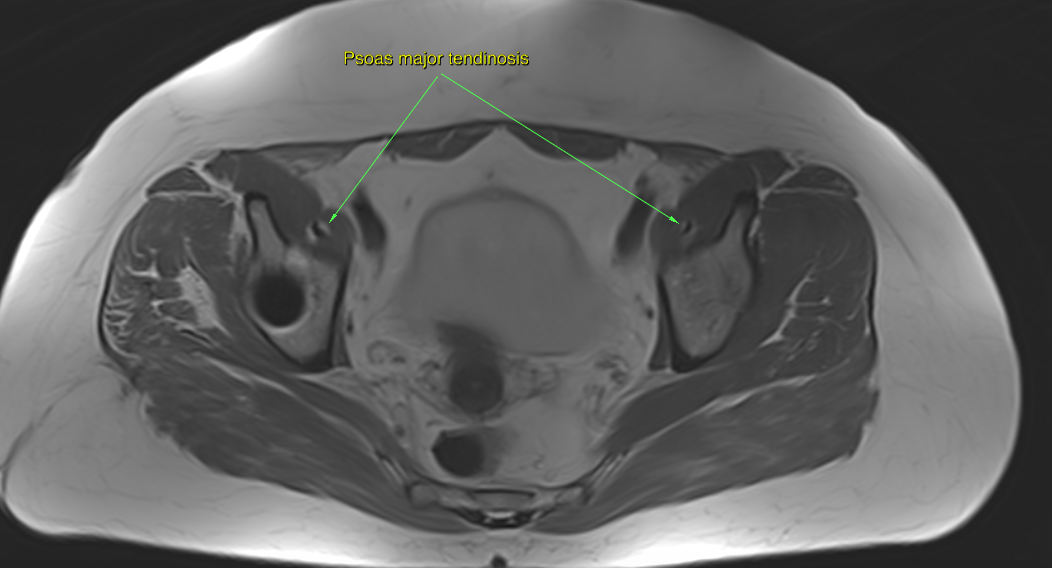
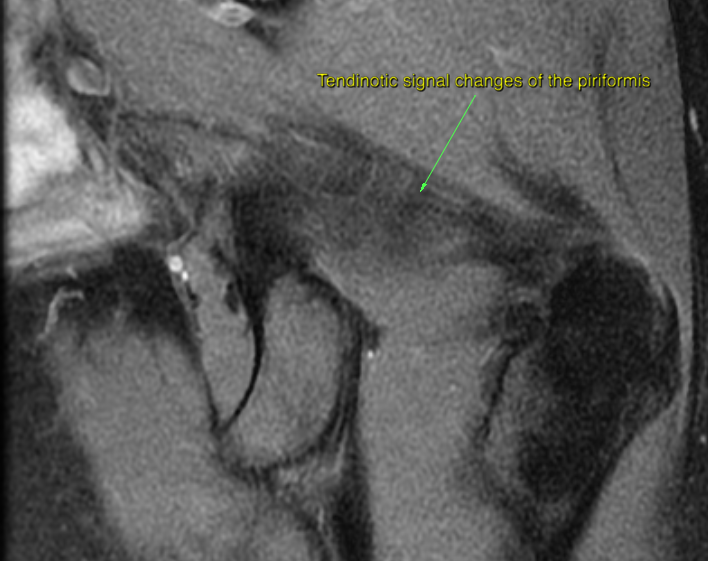
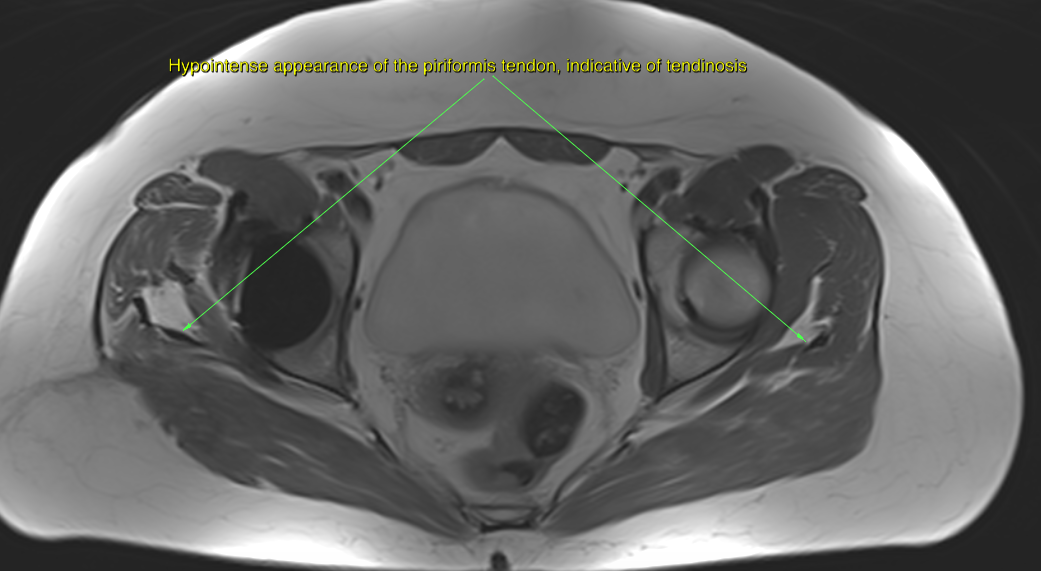
However, I have found that although one may seldom be able to visualize neuropathic lesions (thickening) of the sciatic nerve or the lumbar plexus upon MRI in patients with obvious nerve entrapment symptoms, tendinous degenerative changes which are indicative of tendinosis may be seen in the muscles of tight compartments, such as the piriformis, obturator internus and iliopsoas. Generally, STIR and T2 sequences are used for myotendinous evaluation, as they are sensitive to fluids, however tendinosis is a degenerative condition and not an inflammation, and thus fluid is not what one wants to look for. Hypointense tendinous signal changes are well visualized on PD and T1 sequences, especially in the axial plane.
NCV can be prolonged by injury or simple extrinsic pressure against a nerve.41 NCV prolongation is especially seen in patients with long-standing NTOS that results in muscle atrophy.42 However, other articles have reported that NCV is often normal in patients with symptoms of NTOS.42,43
Somatosensory evoked potentials studies have been found useful in some reports.46,47 However, somatosensory evoked potential has also been criticized as nonspecific, nonlocalizing, and rarely abnormal.43,44,48
Findings showed denervation activity, increased mean action potential amplitude, and/or duration and reduced recruitment at maximum effort. However, there is still some question as to whether EMG is adequately sensitive to detect changes in NTOS patients with milder symptoms.42,45 – Sanders et al., 2008
Somatosensory evoked potentials (SEPs) are used in the diagnosis of thoracic outlet syndrome (TOS), even as an indication for surgery. The purpose of this study was to evaluate the use of SEPs in the diagnosis of TOS. Twenty-one patients (mean age, 37 years) with TOS and 23 control subjects (mean age, 34 years) were included. Somatosensory evoked potentials of median and ulnar nerves were measured bilaterally in patients in both a relaxed and arms-elevated provocative position. A three-way analysis of variance showed no significant difference between the interpeak latencies of the TOS and control groups (p = .352). Significant differences were found in testing positions (p = .0014) and nerve tested (p = .001) in both groups. Therefore, this study suggests that SEPs are not helpful in the diagnosis of TOS. – Komanetsky et al., 1996
The regional anatomy of the lumbar plexus
Fig. 3
The lumbar plexus was situated within the psoas major muscle in 61 of 63 cases. In 2 of 63 cases the entire plexus was localized posterior to the psoas major muscle. In the 61 of 63 cases in which the lumbar plexus was situated within the psoas major muscle, emergence of the individual nerves most often occurred on the posterior or posterolateral surface. – Kirchmair et al., 2008
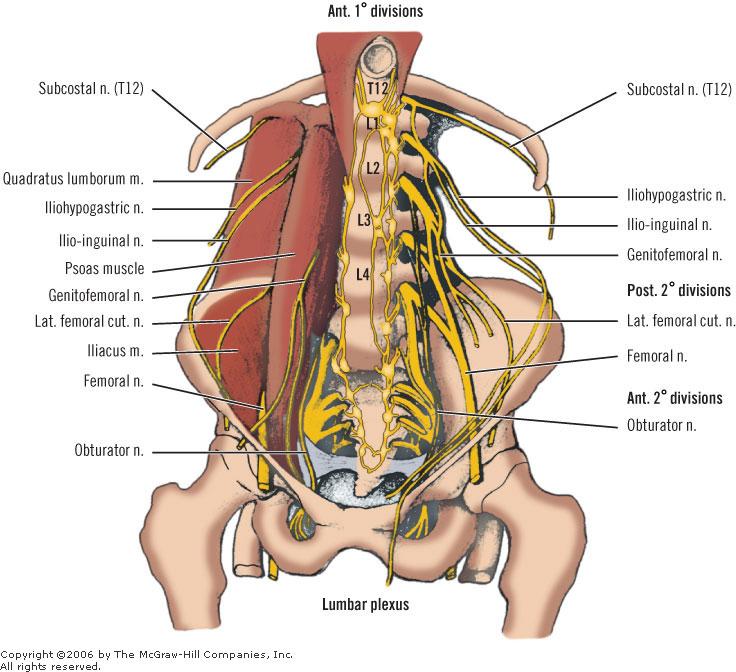
The lumbar plexus is a complex neural network formed by the lower thoracic and lumbar ventral nerve roots (T12 to L5) which supplies motor and sensory innervation to the lower limb and pelvic girdle. Formed within the substance of the psoas major muscle, anterior to the lumbar transverse processes. – Hacking et al., (Radiopaedia)
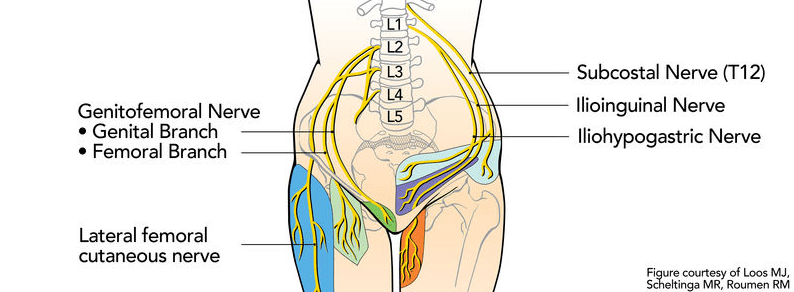
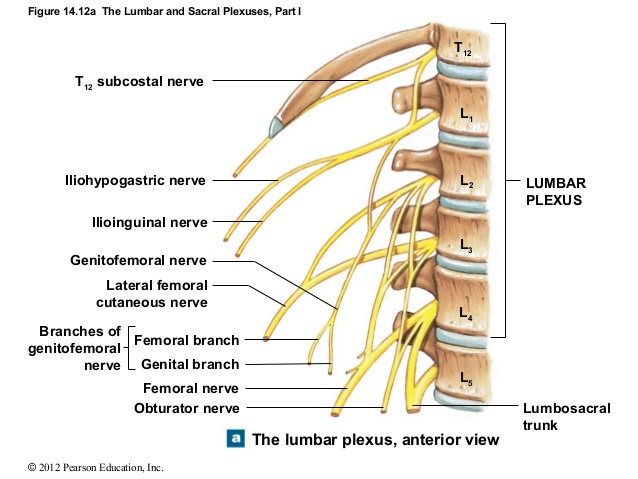
The lumbar plexus consists of the nerve roots between the T12 and L5 vertebrae. Important: All of the lumbar plexus’ nerve roots pass through the psoas major muscle in most individuals. Here’s a general overview of its branches; the …
- Subcostal nerve originates from the T12 nerve root, and passes between the psoas major, quadratus lumborum, and through the transversus abdominus and internal oblique muscles. It innervates the skin and muscle of posterolateral abdominal wall, such as the transversus abdominus.
- The subcostal nerve is an uncommon cause of lower thoracic horizontally distributed (lower costal) nerve pain.
Fig. 4
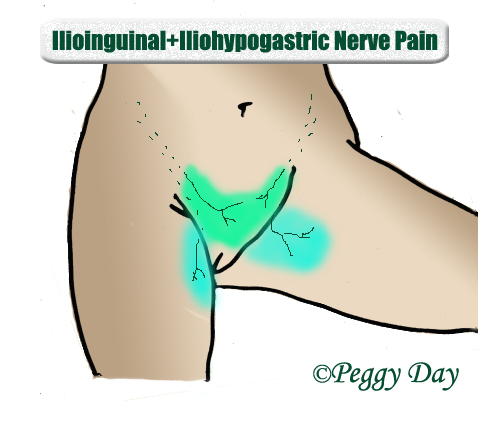
- Iliohypogastric nerve originates from the L1 nerve root. It passes between the psoas major and quadratus lumborum muscles, and innervates the skin and muscles in the lower part of the anterior abdominal wall, such as the transversus abdominus and internal oblique muscles.
- The iliohypogastric nerve is a relatively uncommon cause of lower abdominal nerve pain.
- Ilioinguinal nerve originates from the L1 nerve root. It passes between the psoas major and quadratus lumborum. It provides cutaneous (skin) innervation to the superior medial thigh, and; in men, it also supplies the skin over the anterior one-third of the scrotum and the root of the penis. In women, it also supplies the skin over the anterior one-third of the labium majus and the root of the clitoris.
- The ilioinguinal nerve is a somewhat common cause of nerve pain in the groin and genitalia.
Fig. 5
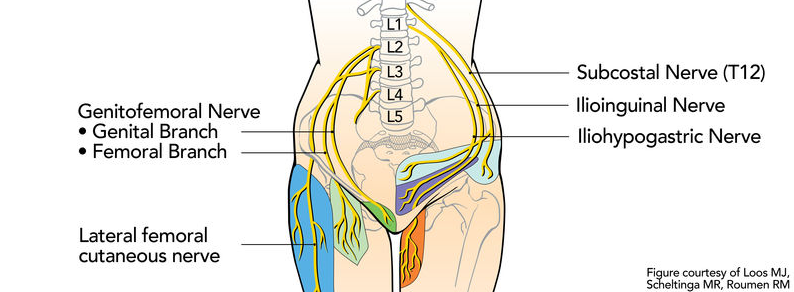
- Genitofemoral nerve originates from the L1-L2 nerve roots. It passes though the psoas major, and innervates the skin around the femoral triangle (groin) through the femoral branch. The genital branch, supplies the spermatic cord, testicles and scrotal skin in men, and the mons pubis and labia majoria in women.
- The genitofemoral nerve is a common cause of groin and genital-regional nerve pain.
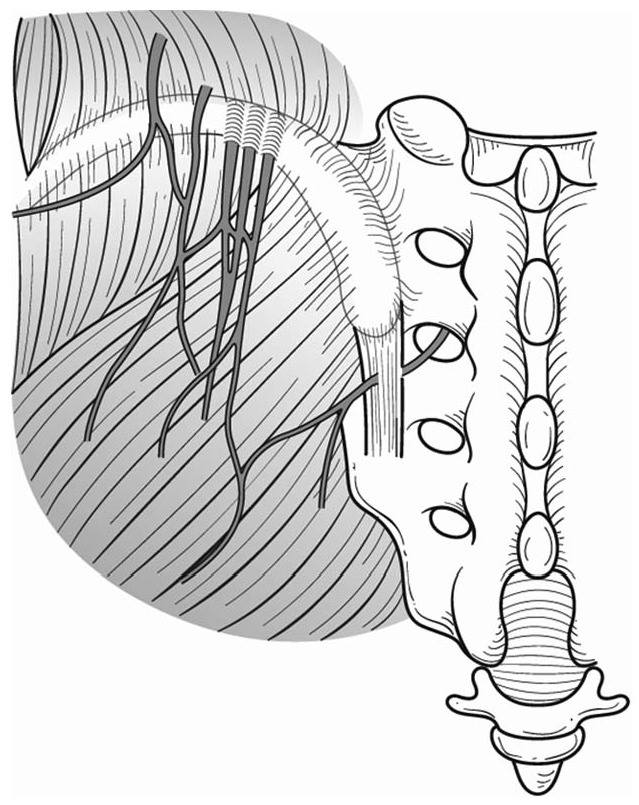
- Superior cluneal nerves originate from the dorsal ramus of the spinal nerves, from the L1-3 nerve roots. It passes through the psoas major, quadratus lumborum and finally into the gluteus medius. It innervates the skin of the upper lateral gluteal region.
- The superior cluneal nerve is a common cause of proximal posterolateral buttocks pain.
Fig. 6
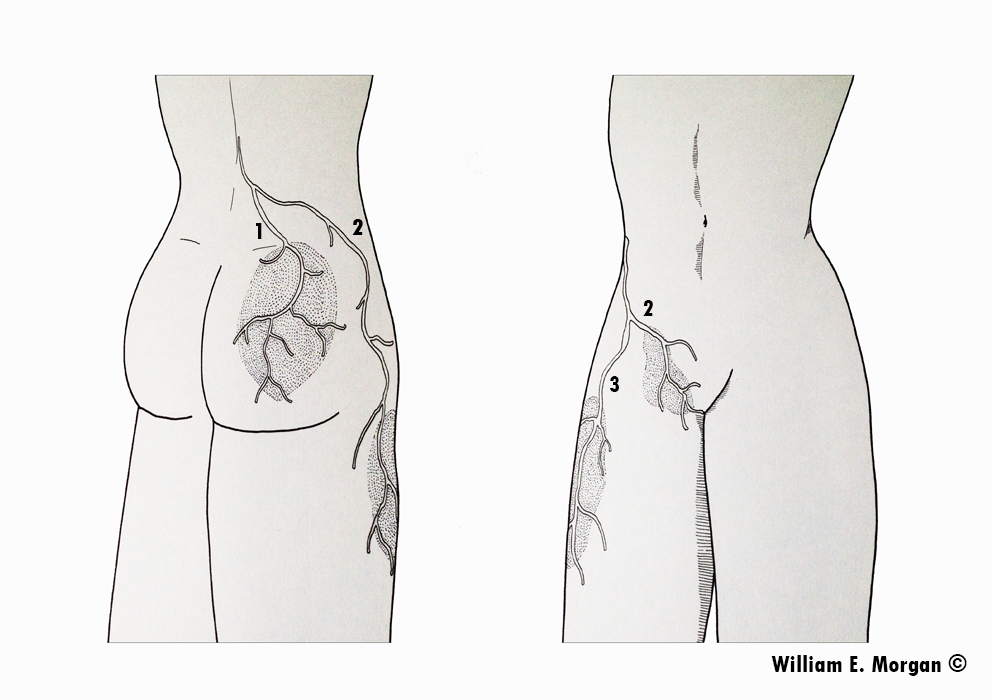
- Lateral femoral cutaneous nerve originates from the L2-L3 nerve roots. It passes between the psoas and quadratus lumborum muscles, through the iliac fascia and then between the iliacus, inguinal ligament and sartorius. Occasionally it perforates the inguinal ligament. it innervates the lateral part of the thigh’s skin, between the lateral pelvis and the upper patellar region.
- The lateral femoral cutaneous nerve is a relatively common cause of lateral leg pain, and may spread down toward the knee.
- Femoral nerve originates from the L2-4 nerve roots. It passes between the psoas major and iliacus, then between the iliopsoas tendon and inguinal ligament. It innervates the iliacus, pectineus, sartorius, quadriceps and articularis genu muscles, as well as the middle and medial skin of the leg.
- The femoral nerve is a relatively common cause of anterior leg pain.
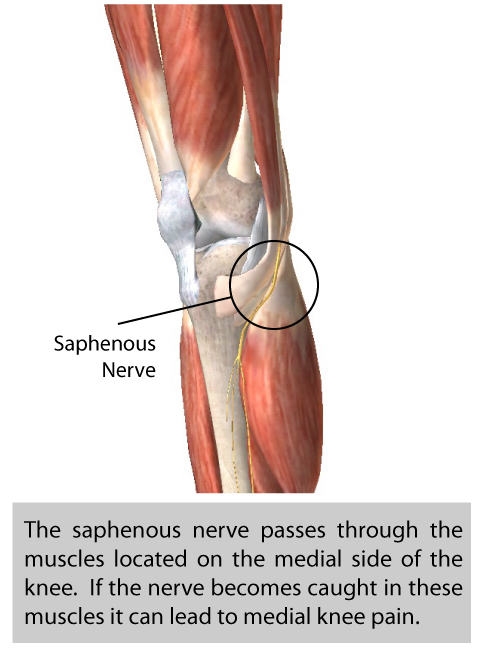
- Saphenous nerve eminates from the femoral nerve. It passes between the distal semitendinosus and sartorius muscles, then between tibia and flexor digitorum longus muscles. It provides cutaneous (skin sensory) innervation to the medial thigh, knee, calf and foot.
- The saphenous nerve is a relatively common cause of medial thigh, knee and calf-regional nerve pain.
Fig. 7
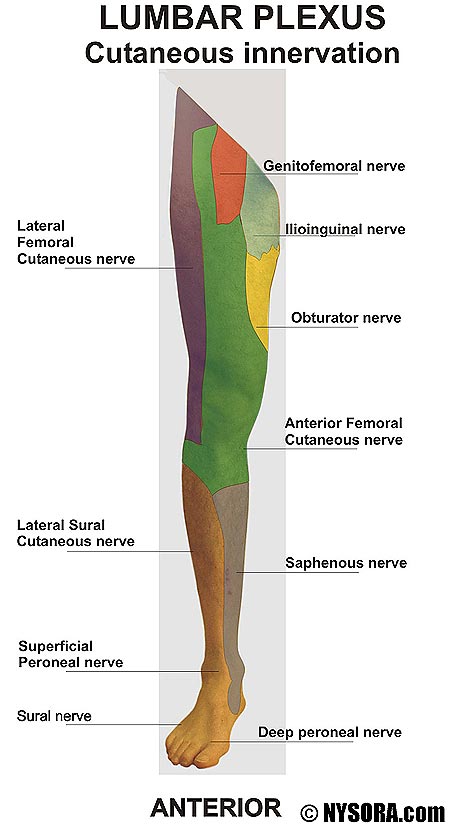
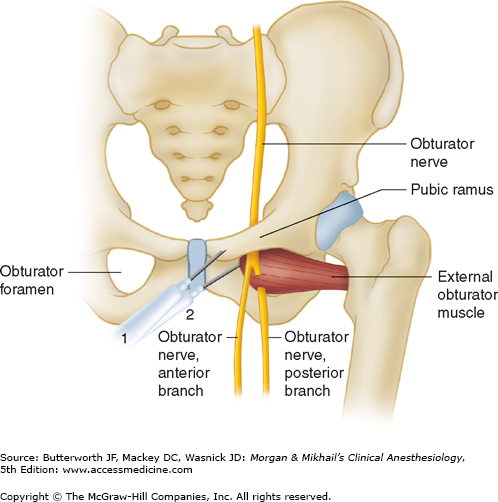
- Obturator nerve originates from the L2-4 nerve roots. It passes through the psoas major and obturator externus muscles, as well as between the obturator externus and adductor magnus (posterior branch), and the pectineus and adductor brevis (anterior branch). It innervates the obturator externus and the adductors.
- The obturator nerve is a relatively common cause of medial lower buttocks and groin pain.
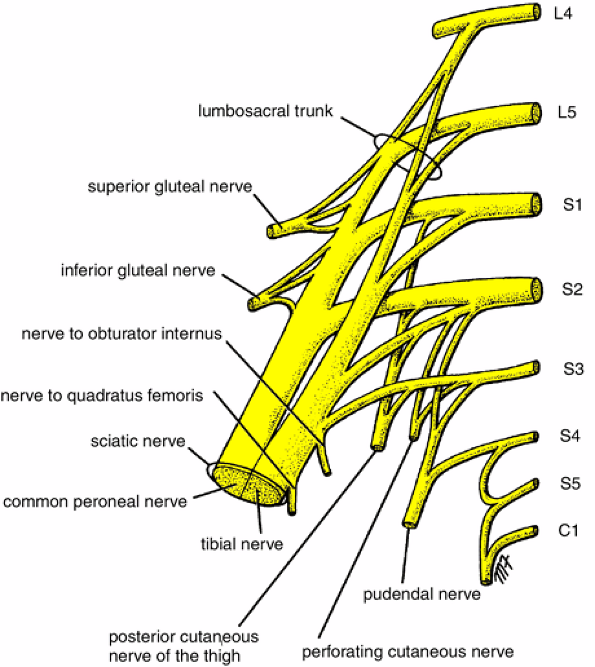
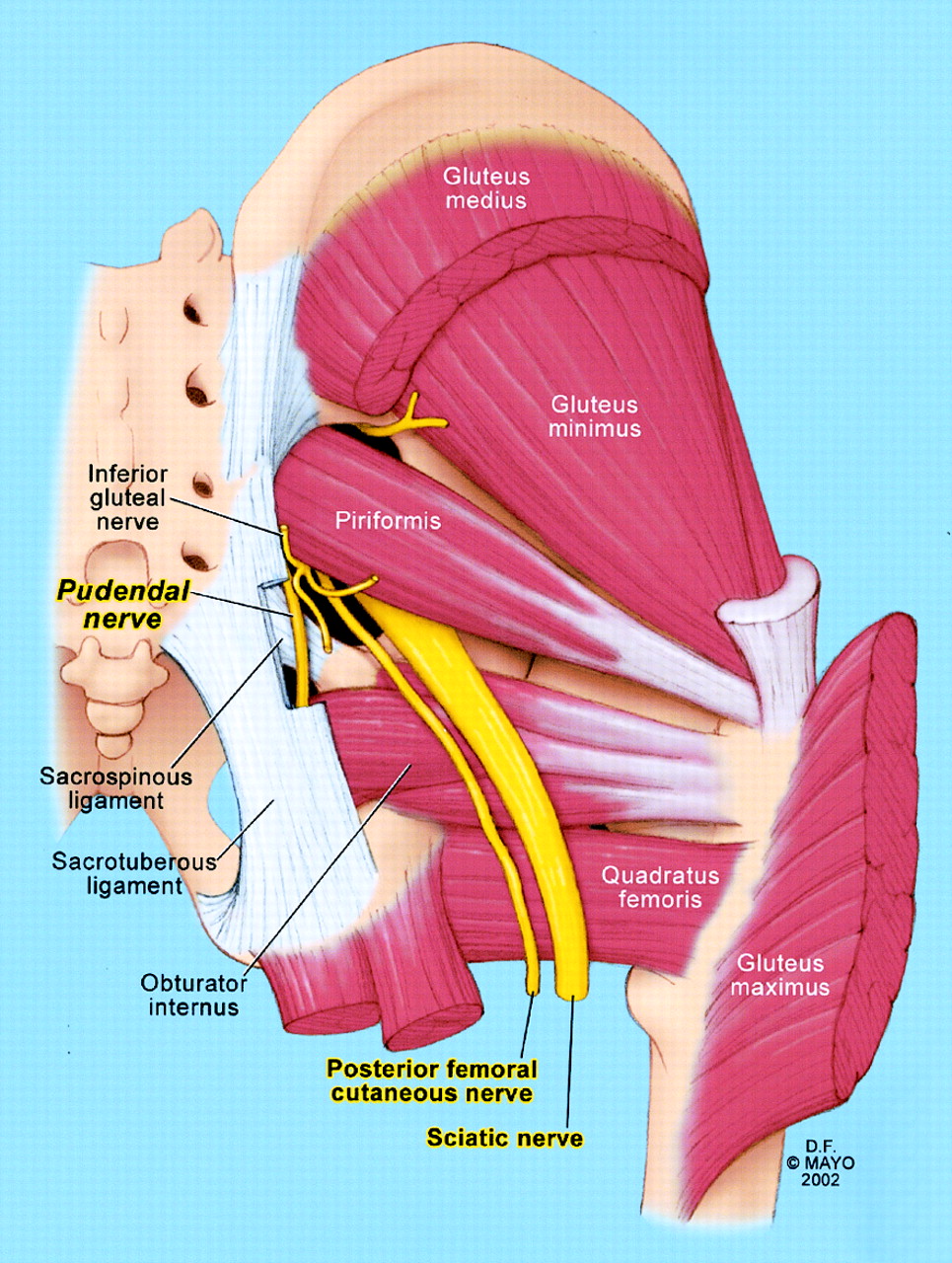
- Lumbosacral trunk originates from the L4-5 nerve roots and passes through the psoas major. It contributes to form the sacral and pudendal plexus, and amongst it, the; sciatic nerve, pudendal, superior gluteal nerve and inferior gluteal nerves. Amongst these, it also contributes to the innervation of the deep six hip rotators, especially the quadratus femoris, gemelli, and obturator internus.
- The lumbosacral trunk’s involvement in sacral plexus neuralgia is hard to evaluate due to the many possible entrapment zones, but it may be a cause of gluteal and pudendal-regional nerve pain.
Fig. 8
Entrapment sites
As the reader may have expected, the main compression site of the lumbar plexus is within the psoas major muscle. This is, of course, because all of the lumbar plexus’ nerve roots pass through it. Secondary common compression sites have briefly been mentioned already, but are as following:
Fig. 9
- The subcostal, iliohypogastric, ilioinguinal and superior cluneal nerves between the quadratus lumborum and psoas major.
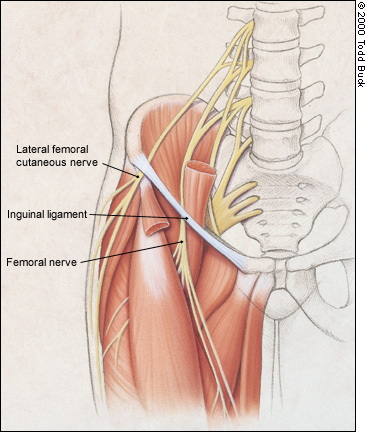
- The lateral femoral cutaneous nerve between the iliacus, sartorius and inguinal ligament
- The femoral nerve between the iliopsoas tendon and inguinal ligament. The femoral nerve may also become positionally compressed between the inguinal ligament and pectineus during hip flexion, which causes femoral neuralgia and anterior thigh numbness in seated posture, especially when leaning forward.
- The saphenous nerve between the sartorius and semitendinosus, as well as between the medial tibia bone and flexor digitorum longus muscle
- The obturator nerve within the adductors and obturator externus muscle
Non lumbar plexus entrapment sites:
I’ll list a few more important entrapment zones that may not be typically considered as related to the lumbar plexus. There is, though, some direct lumbar plexus interconnection to the sacral plexus through the lumbosacral trunk.
- Sciatic nerve compression between the piriformis and obturator internus, as well as beneath the biceps femoris
- Tibial nerve compression between the popliteus and gastrocnemius, as well as between the tibialis posterior and soleus muscles.
- Peroneal nerve compression between the fibula and peroneus longus as well as the tibialis anterior muscles
- Pudendal nerve compression between the falciform process of the sacrotuberous ligament and the obturator internus, as well as beneath the piriformis muscle.
Fig. 10

By knowing the potential symptoms and tight passages of the nerves in question, it’s relatively easy to find the culprit(s) by using provocative testing on these areas. In fact, specific pain provocation is the key to solving myofascial neuralgic syndromes, as it not only reveals which nerve is affected but also by which structures it is compressed. I’ll describe this process soon, but first let us look at some information regarding potential ANS affection of myofascial origin.
A potential for autonomic entrapment / affection
I have noticed that the potential for autonomic nervous system (ANS) dysfunction due to psoas major compression is plausible. This all started with seeing how someone close to me always had severe menstrual pain (during her period), when standing up (hip extension). She was always fine as long as she was sitting down, indicating that something mechanical could be the cause of her persistent pain. I pondered on this, as the ovaries and uterus shouldn’t be that affected by hip extension.
Especially one day, after working out her psoas to rehabilitate a cluneal nerve issue, she started having non-period related menstrual type pain. When I compressed the psoas with MPPT, this also reproduced the same pain that has been felt during the period for years. It occurred to me that the psoas major must also have some effect on the ANS. This makes sense, as the somatic and autonomic nervous systems are interconnected through the ramus communicans, as illustrated below.
Fig. 11

My hypothesis is that LPCS causes irritation that spreads to the organs through the prevertebral ganglia, such as the hypogastric, celiac and mesenteric plexuses, which innervate the abdominal viscera. It’s very well known that somatic compression spreads through its nervous fibers, often to distal ends (i.e disc herniation with nerve root compression, sending lightning bolts down to the calf), and some studies also show that nerve root compression can affect the ANS. Similar ANS affection of myofascial origin will of course cause much milder symptoms, if any at all, in comparison with something like a central disc herniation at the upper lumbar levels.
In addition to sympathetic symptoms being caused by lumbar plexus compression within the psoas major, both the sympathetic and parasympathetic divisions of the ANS pass through the diapraghm. This may be why we see all kinds of strange symptoms appear when people are in stressful situations, as the diaphragm tightens due to increased bodily tension and thus potentially squeeze around the esophagus (and the vagus nerve that surrounds it) as well as sympathetic chains around the spinal column. Further more, many also hold their breaths and create IAP (valsalva) when they get stressed. If the stress isn’t being properly managed, I’ve seen this cause significant tightening of the diapraghm, even to the degree of causing hiatal hernias and chronic acid reflux.
Fig. 12

Laboratory evaluation of autonomic nervous system (ANS) in patients with cervical compressive myelopathy (CCM). Patients with CCM have definite ANS dysfunction as compared to healthy age- and sex-matched controls. There is significant improvement in 30:15 ratio after surgery. – Srihari et al., 2011
On the basis of investigations involving 134 patients operated on at the National Institute of Neurosurgery, Budapest, the authors point out that herniations of the intervertebral discs at L 1/2, L 2/3, L 3/4 levels are characterized by more severe neurological changes. Paresis and autonomic disorders occur much more frequently than in lower lumbar disc herniations: paresis was found in 67 cases (50%) and bilaterally in 44 cases (32.8%), with inability to walk in 21 cases (15.7%); autonomic disturbances were noted in 36 patients (26.9%). With clear symptoms of a lumbar disc herniation a raised protein content in the CSF, more than 100 mg%, makes one suspicious of an upper lumbar lesion. In most of the cases the level of the lesion could not be exactly determined on the basis of sensory symptoms alone. The more severe neurological changes are attributed to a medial situation of many disc hernias as found at operation, and also to unduly prolonged conservative treatment. The early postoperative results are analysed, most of which show permanent further improvement. – Pásztor et al., 1981
Cauda equina syndrome (CES) is a rare condition with a disproportionately high medico-legal profile. It occurs most frequently following a large central lumbar disc herniation, prolapse or sequestration. Review of the literature indicates that around 50–70% of patients have urinary retention (CES-R) on presentation with 30–50% having an incomplete syndrome (CES-I). – Gardner et al., 2011
Neural network for erectile functioning has been well documented over the last decade. Lumbosacral roots merging to form the pudendal nerves plays major role in the erection mechanism. Root compression leading to radicular pain theoretically may also impair the parasympathetic nerves that regulate the production of nerve mediated nitric oxide release and thus debilitate the erection process. – Kulaksizoglu & Kaptan, 2011
Fig. 13 – The sympathetic division of the ANS. Click for full size.
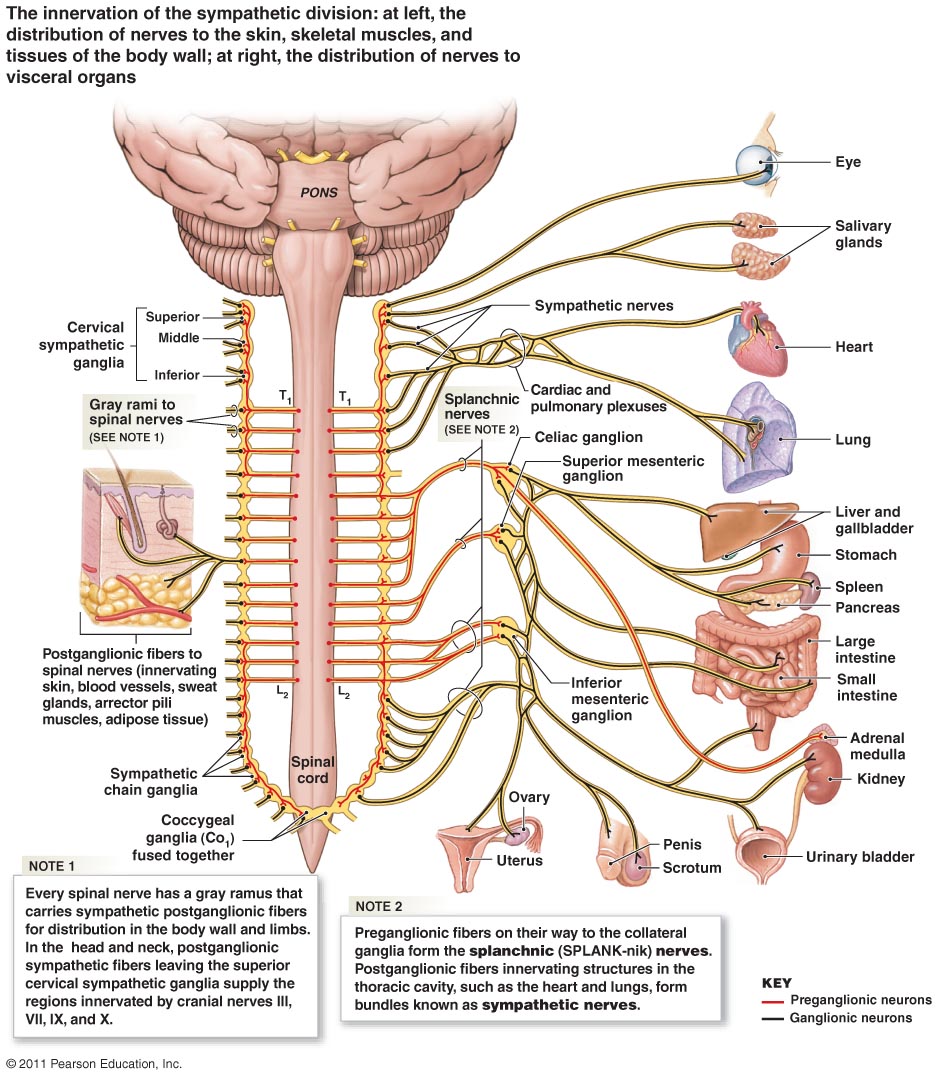
I’ve both had and heard of cases where menstrual pain (as mentioned), bedwetting, premature ejaculation, erectile dysfunction, hiatal hernias, both bradycardia & tachycardia, acid reflux and similar issues have been linked to autonomic compression within the psoas major and/or diapraghm.
Sadly, I haven’t been able to follow up all of these cases, and some of them are still in treatment at my clinic (which is why this is still just a hypothesis), but it’s an interesting and also plausible aspect of the potential causes of ANS dysfunction that I think is worth sharing. I hope to have more clinical anecdotal “proof” soon, and when that happens I’ll update this article.
NEWS per august ’17: I have somewhat confirmed this theory, both with regards to more evidence emerging on the subject, as well as seeing very direct correlations in clinic.
The main autonomic compression sites that I am aware of, are as following:
- Trigeminal nerve (CN 5) behind the mandibular ramus and within the lateral pterygoid muscle
- More information about this in my TMD-article.
- Vagal compression between the clavicular head of the SCM, and anterior scalene. Also, in the esophageal passage through the diaphragm. I’ve also seen it theorized that posterior occipital glide on the C1 or significant atlanto-occipital rotation may cause the vagus nerve to crash into the C1’s transverse processes, jamming it between the TVP and jugular foramen. I haven’t seen this myself, but I consider it plausible.
- More information in my TOS-article and atlas-article
- Sympathetic chain compression within the diaphragm and psoas major.
Naturally, I don’t have all the answers as to what array of symptoms irritation of the ANS may produce, but you can use this chart of ANS mechanisms (link), which may considered as a reference for potential symptoms of ANS dysfunction.
Fig. 14 – The parasympathetic division of the ANS. Click for full size

Identification by provocative testing
Back to the main topic: In order to assess the various nervous branches for affection, manual pressure provocation tests (MPPT), manual muscle tests (MMT), or specific strengthening exercises (SSE) can be utilized to see whether they reproduce the symptoms that the patient is experiencing. To learn MMTs, I recommend David Weinstock’s book “NeuroKinetic Therapy”. As mentioned, it is absolutely critical to find the specific structures involved in the pain pattern in order to remove the guess-work, and to be able to identify the true pattern of dysfunction, so that an effective corrective strategy can be initiated. If you don’t know exactly which nerve is entrapped, nor where it is entrapped, you are indeed shooting in the dark.
Most of the time, manual provocation by pushing into the nerve at its entrapment points (MPPT) will give a relatively accurate answer with regards to whether there is nervous tissue irritation in that area or not. To use this method, you need to know the regional anatomy, the suspected nerve’s entrapment sites, and of course have decent palpative skills.
Let’s say you have nervy groin pain that appears every time you or your patient walk up hills (hip flexion with a bent knee). This could be indicative of entrapment of the the obturator, genitofemoral and/or ilioinguinal nerves, which are all affected by the psoas and innervate that area. Push firmly into the proximal psoas major at L1-L3 (always ask your client if they are bloated or have abdominal pain first) and see if this reproduces the symptoms in the groin. I always ask “Does it radiate, or is it local?” (radiative or shooting type of pain is positive for neuralgia). If it does, the nerves are being compressed by the psoas major and you’ll know that it requires strengthening. Furthermore, if the psoas major is positive for nerve compression, it’s a good idea to MPPT other secondary compression sites as well, such as the obturator externus (for this scenario). Which secondary sites to check, of course depends on the complaints of the client.
A simpler example could be that your patient has gluteal neuralgia, and has of course taken an MRI to rule out disc herniations. Simply compress the sciatic nerve by pushing firmly into the middle part of the piriformis muscle. If the pain reproduces, you know that the piriformis is causing irritation to the sciatic nerve, and that it needs strengthening. Also here, a check of secondary compression sites could prove worthwhile, such as beneath the biceps femoris and between the popliteus and tricep surae muscles, as mentioned in the reference list earlier.
Reproduction of the sciatica upon deep palpation, either by gluteal or rectal route, was diagnostic. – Durrani & Winnie, 1991, Piriformis muscle syndrome: an under diagnosed cause of sciatica
Fig. 15

If the MPPT did not reproduce (or produce) any nerve pain, this could simply mean that the nerve is not affected, or that you’re either not at the right spot, not pushing hard enough, or that it’s “one of those” clients who don’t respond to MPPT (more on that below). Make sure to move around a little before giving up, to make sure that the right spot – directly onto the nerve’s course – is being compressed.
If all the symptoms fit the respective nerve you’re suspecting, for example the genitofemoral nerve in the scenario with the psoas major compression above, but the MPPT is definitely negative, there are more methods to check for potential nerve irritation. You can use a manual muscle test (MMT) to see if contraction of the muscle reproduces the pain, or you can use a specific exercise to target the muscle in question with a task that requires higher work capacity. If MPPT didn’t reproduce the pain, and you decide to try MMT and SSEs, the pain may not appear until the day after.
I’ve also written about these assessment approaches in my thoracic outlet article (linked further up), which revolves around the same principles of finding and correcting the entrapment sites, rather than wasting your time on random stretching and nerve flossing protocols that are not specific nor lead to lasting results (more on this later).
When performing the MMT and SSEs, details matter. If someone has nerve-pain due to muscular compression, that muscle is usually extremely weak (NOT overactive), as mentioned earlier. It’s important to understand that this weakness combined with pain may make MMTs and exercises less specific, because the patient will often brace the body (usually subconsciously) to avoid getting hurt. Their nervous system already knows that this movement or method of provocation that you’re exposing them to, is a bad idea. The result is what I call “clenching”, where all the muscles in a region is clenched (bracing), rather than normal muscle-activation. In such cases it is important to identify the clenching and teach the client to be relaxed while performing the tasks in question.
A slight disgression, but if an area is very painful, the patient will often brace the whole complex (i.e all of the respective muscle’s synergists) in order to protect the body from the pain that occurs when the dysfunctional muscle is being loaded, i.e tested with MMT. This is a strategy that masques the muscle as strong, often misleading the therapist performing the tests. This “cheat” will of course have to be identified and cued away by the therapist, in order to perform the MMT properly and consequently reveal the muscle’s true status; weakness. Some cues that I like to use are “don’t clench your whole body”, “meet my pressure naturally”, or even have them initiate the movement rather than resisting my pressure. In my experience, the harder a person braces the body when being tested with MMT, the higher is the likelihood of significant dysfunction. Some people, especially those who suffer from chronic pain, sometimes execute this brace very calmly. So be observant, and don’t trust your first MMT when dealing with myofascial nerve entrapment issues.
Compression vs. entrapment
This part has been added some time after writing this article, and comes with some important distinctive information. The words ‘compression’ and ‘entrapment’ are used somewhat interchangeably in this article. They are also used in similar fashion in much medical literature. After writing this article, however, I’ve come to realize that these two phenomena are two quite different things, especially with regards to provocative testing of the nerves and detection of pathology. Therefore I need to describe these differences here in this subheading.
Nerve entrapment occurs when a nerve is not able to adequately glide through myofascial structures. Entrapments can vary in severity, and when extremely severe, they may mimic a true compression, but I’ve only seen a couple of patients who had this latter issue. In virtually all circumstances, nerves that are entrapped will produce pain when compressed manually (provocative testing).
Nerve compressions occur when there is direct mechanical compression to the nerve(s) involved. For example, the clavicle can compress the brachial plexus within the costoclavicular passage. A tight pectineus can compress the femoral nerve into the inguinal nerve upon hip flexion. A disc herniation can cause true compression, and so on. Truly compressed nerves will usually not produce pain when tested with provocation, and may therefore cause false negative interpretation of the tests. They may however, sometimes do so if compressed manually for longer periods, approx. 30 seconds, but not always.
Furthermore, we must distinguish between intermittent compression and constant compression. A disc herniation will usually cause a whole dermatome to seem negative when tested with MPPT. Intermittent compression, however, such as at the costoclavicular space or inguinal ligament, will often cause MPPT to seem negative at the area of compression, but distal branches will produce pain when manually compressed. This is not a rule written in stone, but seems to be a relatively reliable guideline.
If the patient has obvious femoral neuralgia, but MPPT is negative, try to compress the saphenous nerve. If the saphenous nerve produces pain, it may be intermittent compression at the inguinal ligament. If none of the nerve’s or its branches’ provocative test points are negative, you may be dealing with a disc herniation. If the inguinal MPPT is negative but saphenous and clunial nerves for example are positive, you may be dealing with both LPCS and femoral nerve compression by the inguinal ligament and pectineus.
Thus, if there are symptoms similar to nervous affection, but the pressure tests are negative, consider true nerve compression. The therapist needs to discern and interpret the results to some degree if there is probability of true mechanical compression, and if so, whether it’s intermittent or constant, to explain the most likely aetiology of the patient’s symptoms. In 85-90% of these cases, though, I’d say that the typical manual provocative testing will produce pain and therefore easily reveal the problem.
Regions and expectations for MPPT
Evaluation of the psoas major
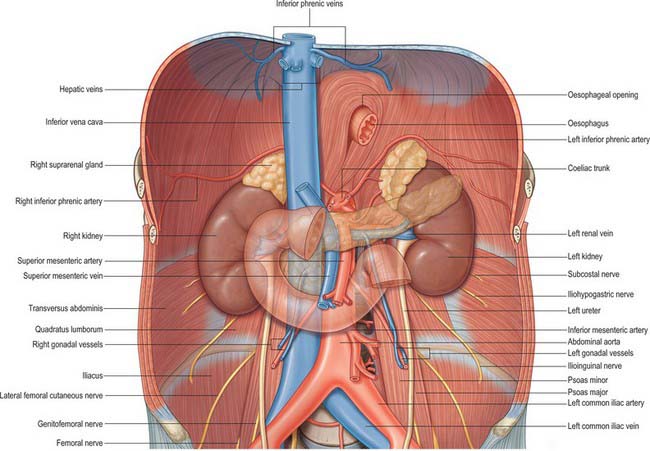
As mentioned numerous times now, the main compression site for the lumbar plexus, is within the psoas major. The psoas is almost always weak, but most people are still stretching it relentlessly. Big mistake. The psoas maintains lumbosacral lordosis and stabilizes the lower back, contributes to sacroiliac joint nutation and force closure, helps with anterior hip impingement and general iliofemoral stability by providing anterior stability to the femoral head, and is a tunnel for the lumbar plexus. To say it’s a pretty important muscle, would be an understatement.
If your client shows signs of lumbar plexus entrapment, and you know it’s not caused by a disc herniation, check the psoas first. Even if the pain is at the medial knee (saphenous nerve); it almost always starts with the psoas. To MPPT the psoas major, you need to go anterior to posterior through the abdomen, obliquely toward the lateral side of the spine (this should only be performed by trained health personell). Once again, make sure to ask the patient if they have abdominal pain, such as bloating or similar, before going in. If they do, use MMT or SSE for provocation assessment instead.
When you MPPT the psoas, make absolutely sure that you’re palpating the psoas and not an organ before you increase the pressure. When you attempt to MPPT the proximal part, it’s a good idea to use a superiorly oblique direction of pressure to avoid the kidneys. Likewise, avoid going too far medially toward the spine, so that you don’t end up compressing the aorta or vena cava. If you feel a pulse, go lateral. It should be a muscular feeling, and the patient should confirm that it feels like a muscle. If it does, compress it, and see whether the nerve pain reproduces.
- Proximal part: Subcostal (also assess QL), superior cluneal, iliohypogastric, and ilioinguinal nerves
- Middle part: Genitofemoral and lateral femoral cutaneous nerves
- Distal part: Femoral and obturator nerves, lumbosacral trunk
By pushing into the psoas, any type of neuralgia as a response is considered a positive test. If your patient has genital pain, but the test reveals abdominal (iliohypogastric) neuralgia, that’s still a confirmation of severe myofascial dysfunction, and means that the psoas needs rehabilitation. It doesn’t matter if the exact same pain is reproduced or not when all the nerves pass through the same muscle. It does matter, however, if they don’t. More on this soon.
Fig. 16
I’ll also include the manual muscle test for the psoas major, as it is the prime suspect of LPCS.
MMT walkthrough: The patient’s lower back is significantly arched, and femur is laterally rotated. The therapist stabilizes the contralateral pelvis, and pushes the leg down and out (posterolaterally), i.e opposite direction of its fibre orientation. Patient attempts to resist without clenching the full body nor holding his or her breath. Common cheats are to round the lower back, flexing the knee, holding their breath or clenching their abdominals (or full body).
Fig. 17

If the MMT doesn’t reproduce the pain either, you could leave the patient in the test-position as static hold for 30 seconds. If this also does not reproduce the pain, the psoas may not be the cause of the neuralgia, or the patient’s pain is not sufficiently pre-triggered to reveal itself on command. Sometimes the pain doesn’t appear until the day after the strenuous activity. Honestly, the psoas is almost always dysfunctional, just strengthen it and see what happens. The static hold as I just described is a good way to do so (SSE), because the video I’ll show later may prove to be too progressed for individuals with significant weakness, which will just result in cheating and thus also lack of progress.
Pain patterns from MPPT to the psoas major, generally spread out into the groin (obturator, genitofemoral), medial butt (obturator) or abdominal (ilioinguinal, iliohypogastric) region. For more distal neuralgia such as the saphenous nerve at the medial knee, consider a double or even “triple crush”-effect, where the tissues are pre-compressed within the psoas, and the “last drop” is provided by other tissues down the line, as mentioned above in the reference lists.
The inguinal ligament
The femoral nerve and lateral femoral cutaneous nerves both pass beneath the inguinal ligament. They may be compressed between the iliopsoas tendons and the ligament itself. Compression to the inguinal ligament is usually quite effective, revealing potential entrapment immediately when done correctly.
To assess the lateral femoral cutaneous nerve, push down and in (inferior posterior) on the lateral part of the inguinal ligament. For the femoral nerve, apply the same pressure to the middle part of the ligament. The pain patterns should either spread into the lateral (lateral cutaneous nerve), intermediate (femoral nerve) or medial (saphenous nerve) quadriceps. If the tests are positive, then the iliopsoas and sometimes sartorius muscles will need strengthening.
Fig. 18
The obturator externus
The obturator nerve pierces the obturator externus muscle before entering into the medial compartment of the thigh. It’s hard to MPPT the obturator externus, as it is located on the posterior side of the ischial tuberosity. I will use an MMT, or strengthening exercise (SSE) to assess this muscle. If the pain reproduces with MMT (immediately), or with SSE (pain usually felt the day after), this once again means that the muscle need significant strengthening. The neuralgic pattern for obturator nerve pain, is usually into the medial buttocks, or into the medial thigh. Because the obturator nerve first passes through the psoas major, it is of course important to assess this muscle as well, even if the pain just appears in the gluteal or medial thigh regions.
You can find exercises for the obturator externus muscle (link) in my video library.
Fig. 19
Cluneal nerve entrapment
The cluneal nerve has a little different route than the other nerves, somewhat similar to the subcostal nerve. It is the terminal branch of the dorsal lumbar nerves, which first pass through the psoas major and quadratus lumborum, before it enters into the gluteus medius. The cluneal nerve can cause severe pain in the posterior gluteal region.
Within its course, the SCN pierces the psoas major muscle and paraspinal muscles, runs posterior to the quadratus lumborum muscle and pierces the thoracolumbar fascia as it crosses over the posterior part of the iliac crest. – Loubser et al., 2015
When affected, the superior fibers of the gluteus medius will be very sensitive to palpation, and it may feel like a swollen trigger point. Go slightly caudal from the iliac crest, down onto the posterior portion of the proximal gluteus medius fibers. Abnormally high pain in this portion is a positive test. Remember, it’ll feel like a trigger point, and the patient often complains of “back pain” when pointing to this same region. Gentle pressure to this area will often reproduce the symptoms (I always give it a moderate to rough push, it is a provocation test after all), but it doesn’t always spread out.
To resolve this dysfunction, both the psoas major, quadratus lumborum and gluteus medius’ (posterior fibers) will need to be addressed with SSEs.
Fig. 20
The distal hamstring (pes anserinus)
The saphenous nerve, which is a branch of the femoral nerve, can be compressed at the medial knee between the sartorius and semitendinosus muscles. It’s an uncommon cause of medial knee pain, often triggered when the hamstrings are loaded, such as when leaned forward or using high heels. Its pain pattern may be referred neuralgic pain into the medial knee and medial calf, or even foot.
To MPPT the saphenous nerve at this compression site, push firmly into the distal semitendinosus (oblique pressure, posterolateral to anteromedial). If the test is positive, the hamstrings (rarely sartorius) need specific strengthening, by performing knee flexion with the tibia internally rotated to target the semitendinosus. It’s important to remember that the saphenous nerve is a branch, and that it may be predisposed and sensitized due to pre-compression further up the chain, like in the psoas and beneath the inguinal ligament. When distal branches are affected, always assess the whole chain.
Fig. 21
The pudendal canal
For the pudendal nerve it is similar to the obturator externus; it’s difficult to MPPT. Its main compression site is between the falciform process of the sacrotuberous ligament and the obturator internus muscle. The pain can usually be reproduced by MMT of the obturator internus, though. If not, try SSE and see if that reproduces the pain (may come the day after). It probably will, which indicates that significant strengthening of the obturator internus is necessary. The piriformis muscle also lies close to the pudendal nerve and may potentially compress it. For the piriformis, use the same approach as for the sciatic nerve with regards to assessment; try to compress it and see if the pain is reproduced. If it is, strengthen it.
Pudendal neuralgia is recognized by radiative or shooting pain in the genital area, raying into the anus, perineum and genitalia.
Fig. 22
Most of the time, the pudendal nerve will be “double crushed”; first by the piriformis, and then between the falciform process of the STL and the obturator internus.
It may also happen, though rare in my experience, that it also gets caught between the sacrotuberous and sacrospinous ligaments. I know that some people have attempted to “release” the ligaments in order to relieve pudendal neuralgia, but I don’t think this is possible nor viable, because these ligaments are extremely strong. What I consider a better option, is to encourage increased sacral nutation. This will increase the distance between the SS and ST ligaments, thus freeing the nerve. The psoas is the main contributor to sacral nutation, but proper pelvic posture is also very important (more on this later). With MPPT, push posterior to anteriorly into the proximal STL. As always, a positive test is reproduction of the respective symptoms.
Fig. 23

It may also be compressed by the pelvic floor, but personally I have not found the pelvic floor to be a significant player in this dysfunction. The connection, though, is that the psoas, obturators and pelvic floor share fascial bonds (Anatomy trains, Deep front line). We know that 30-40% of muscular tension travels through the fascia (Huijing et al., 2003; Stecco et al.,), and a strong and functional pelvic floor will thus contribute to proper function of the deep six and psoas major.
Some evidence also suggests that affection of the lumbosacral trunk may carry over to the pundendal nerve (Kulaksizoglu & Kaptan, 2011), in which the psoas major (or a potential disc herniation) will need to be addressed to relieve the irritation caused to the lumbosacral trunk.
Sciatic, tibial and peroneal compartments
Slightly related to the lumbar plexus (through the lumbosacral trunk), are the sciatic, tibial and peroneal nerves.
The sciatic nerve parts into two main branches; the tibial, and common peroneal nerves. As seen earlier in the reference list, the sciatic nerve can be entrapped between the piriformis and obturator internus, as well as beneath the biceps femoris. Furthermore, the tibial nerve can become compress between the popliteus, soleus and gastrocnemius. Compressing these structures by applying a solid posterior to anterior pressure, should reproduce the symptoms if there is nervous entrapment at that level. Sometimes the MPPT is positive at the popliteal fossa, other times only at the mid tibial level, into the soleus; it’s important to squeeze the tibial nerve at both regions. If MPPT to the piriformis and proximal soleus invokes neuralgia, but biceps femoris does not (which is a very common pattern of compression), this just means that the biceps femoris is not irritating the nerves. Common signs of affection is a radiative or shooting type of pain down the posterior leg and plantar side of the foot.
If the nerve is extremely irritated from top to bottom, it’s likely a disc herniation. Always rule out disc herniations first, using whatever methods you’re trained with. Straight leg sciatic tension test, swelling in the lower back, extreme sensitivity of the nerve’s path and so on, are all signs of potential disc herniations (read my lower back article (link)) to learn my approach on solving lower back pain).
Fig. 24

The common peroneal nerve splits into two main branches; the deep and superficial peroneal nerves. When affected, they are almost always compressed by the peroneus longus, in my experience. Find the proximal fibula bone, and compress the upper part of the peroneus longus muscle firmly (lateral to medial). If you’re at the right spot, and the patient has peroneal nerve compression of myofsacial origin, he will immediately feel shooting pain down into the lateral calf and dorsal foot if the nerve is irritated.
Fig. 25

Corrective strategy
Posture
As mentioned several times by now, one of the keys to solving myofascial nerve entrapment syndromes such as lumbar plexus compression syndrome, is to both find and properly rehabilitate the structures that are causing nervous tissue compression. It is however also important to ask the question “Why did these weaknesses occur in the first place?”, in order to find and resolve the initial and underlying cause of dysfunction.
Sometimes trauma, surgeries or similar may trigger muscular atrophy or motor pattern changes which may lead to potential nerve entrapment down the line. Most of the time, though, poor postural-, breathing and movement strategies are the main underlying causes of myofascial imbalances (a cliché term, I know). The point is that the responsible motor dysfunction must (should) be identified and corrected in order to properly rehabilitate and cure the secondary nervous entrapment.
As mentioned, the psoas major is a hip flexor, lateral femoral rotator, sacral nutator and lumbosacral extensor. It also contributes to lumbopelvic rotation in gait, as well as maintaining proper lumbosacral alignment when bending (fig. 26) and loading the spine. We need to ensure that our motor patterns do not continuously oppose the psoas major’s functions, in order for it to rehabilitate successfully and long lastingly. The most common cause of functional opposition, is swayback posture with posterior pelvic tilt, walking uphill too rarely, and having a deficit of lumbopelvic rotation in gait. Excessive medial femoral rotation in posture is also an extremely important factor that may need to be addressed, especially for women. If these four habits can be changed, the psoas major will likely remain healthy after its initial, thorough strengthening process.
In the image below a typical gait pattern for ‘these kinds of patients’ is seen. Lateral rotation and abduction should occur as the loaded femur moves into extension. However, we here see medial rotation and adduction. This will often also lead to hip impingement, which is a common co-problem in patients with LPCS. When treating the femoral rotation, minute changes should be made in posture. The patient must be helped to avoid adduction and medial rotation during hip extension by ever-so-slightly laterally rotating their femur in posture and gait. Very small changes must be performed, as transverse plane motion is easily over-corrected.
Fig. x

The psoas also maintains lumbar lordosis and stability when bending; a much lost ability in the westernized society. In figure 26 you can see how it looks like when a person properly bends using the psoas. Surely, no one taught this woman how to hip hinge! It is an innate ability. Luckily, this motor function can be relearned by arching the lower back and pulling the femur toward the abdomen as you bend forward. It may take a few tries until you get it right, but this is how you should bend and it is absolutely worth practicing.
Fig. 26 – Bending with the psoas

I’ve written several articles about postural alignment and its effects on the body, for example in my hip article and lower back article (already linked earlier). Generally you’ll want a slight anterior tilt of the pelvis, enough of a tilt to get the lumbosacral part of the spinal erectors to remain active in posture. The thorax and shoulders should not be hanging back posterior to the butt, but should be slightly in front of it. The butt should point slightly up, and never down, as the latter indicates posterior pelvic tilt.
I’ve written about this several times; forget the notion that exercises can fix your posture. They can’t. Only altered habits, i.e your actual focus and efforts on changing your posture, can resolve poor posture. It is a continuous process. Strengthening work can supplement the habitual changes and make the transition smoother, but at the end of the day you’ll need to work hard to change your structural habits. Get into position, and stay there!
Fig. 27

The psoas and its fascial connections
I touched upon this already, a little earlier. The psoas major is the link between the diapraghm, the pelvic floor and the deep six rotators. Because 30-40% of muscle tension transfer through these fascial bonds, it’s very important to address the system and not just the muscle, if you want to get long lasting results. The diapraghm and pelvic floor makes up the main pressure system in the body, and thus its ability to create and maintain intraabdominal pressure (IAP). If this system is compromised, for example due to inhibited synergistic structures like the psoas, faulty posture or or breathing, it will often cause a negative chain effect to its synergistic muscle chains.
Therefore, in addition to addressing posture, movement, and the dysfunctional muscle itself, I also recommend to address its most relevant fascial and functional cooperators. For the psoas, it is as mentioned the diaphragm, pelvic floor and deep six hip rotators. You could also add the quadratus lumborum, scalenes and transversus abdominus to that list, if you want to be very thorough. All of these muscles have a role in either respiration or IAP. The exercises can once again be found in my video library (link).
Breathing must be well balanced, both with regards to horizontal, downward and upward expansion. In other words, both the belly and chest should expand equally to properly stimulate the muscles of the intrinsic core system (Deep front line, Myers). “3D breathing” is the cliché term. Additionally, these muscles can and should be strengthened simultaneously.
Fig. 28

Specific strengthening exercises
A muscle that is responsible for nerve entrapment, is generally a severely weak muscle. Often atrophied, but not always. Paradoxically, also thick and seemingly tense muscles may be severely weak. This is why it’s so important to have more tools in your belt than just palpation, in order to assess muscular function. Palpation is very subjective, and can be misleading. It takes time and experience doing the right things, to get good at palpation and muscular evaluation. Utilization of MMT and SSE is a good way to further evaluate muscular function; if the exercises and muscle tests are performed correctly (without cheating/clenching), it will often reveal the status quite decently, taking away the guessing.
My recommendation is to always strengthen structures that have shown either by MPPT or SSE to reproduce neuralgic symptoms. The exceptions to this norm are very, very few, in my experience.
Pregnant women with pregnancy-related low back and pelvic pain (PLBP) developed significantly higher muscle activity in the rectus femoris, psoas major and external oblique during the ASLR test than pregnant women with no PLBP (de Groot et al. 2008). Despite this increase in muscle activity, women with PLBP produced significantly less muscle force than non-PLBP women during the ASLR test.
On the symptomatic side the gluteus maximus was far more active compared with the healthy subjects. Despite the increased activation of gluteus maximus, patients with SIJ dysfunction demonstrate significant weakness in the muscle (Massoud Arab et al. 2011). – Vleeming et al., 2012
IMPORTANT: When assigning SSEs for homework (not when using it as a provocation assessment, obviously), you’ll want to start out lightly if the muscle in question has been proven to be involved in nerve compression. Going too hard may greatly increase your symptoms (“SSE aftermath”), so be careful. The symptoms usually do not appear until the day after, if you’ve gone too hard.
As a general rule I recommend my clients to start with 5-10 repetitions for one set, or 30 seconds static hold for one set. See how it feels the day after; are the symptoms significantly worse? If so, consider doing even less. If not, increase a little and see how it feels the day after. Never increase load or volume unless the exercises are done 100% correctly nor if the current regime is increasing the pain significantly.
SSE for the psoas major
This exercise is the most important one in this article. The psoas has relations to almost all of the nerves in question. Generally this muscle is extremely weak, and should be exercised lightly in the beginning. For most patients, especially those with LPCS, it may be beneficial to start out with a static hold variant of this exercise, as the dynamic one will be hard to perform without significant cheating. This is something I have learned after trial and error, so don’t waste your time doing the same.
I’ve touched on it already, but to perform the exercise properly, the lower back must be fully arched, as the psoas arches the lower back. Failure to arch indicates that you’re not getting contact with the psoas. The abdominal muscles must be relaxed in order to fully target the psoas, as clenching them significant load off it. Further, importantly, maximal femoral lateral rotation must be maintained during the exercise. Here is the newest exercise that I have found very effective for strengthening the psoas major.
SSE for the deep six hip rotators
The deep six are sometimes not as extremely atrophied and/or weak as the psoas, because they are forced to contribute somewhat when the hip is loaded, i.e in gait, unless there is excessive medial femoral rotation. Thus case dependent. SSE aftermath symptoms are usually mild/moderate and manageable as long as the muscles aren’t being trained very very hard.
The exception is for pudendal nerve pain; you’ll want to start very easily and gradually build up the strength of the obturator internus, to avoid increased pain in this very sensitive area.
I have developed a new exercise that targets the piriformis to a greater degree. The above exercise will target the quadratus femoris and obturator externus to a greater degree.
SSE for the quadratus lumborum
There are many ways to strengthen the quadratus lumborum, but I generally recommend to start easy. Hiking the pelvis, side planks etc, are good alternatives. To connect with the QL, the lower back must be arched, and the thorax must slightly contralaterally rotate. If ipsilateral thoracic rotation occurs during the hip hike or similar exercise, it will (unpurposely) target the obliques rather QL.
Strengthening the quadratus lumborum may lead to severe back pain initially, as it is often very weak. I once again recommend to start out with light and low volume loads, gradually increasing the the intensity as the muscle becomes stronger and healthier.
See other QL variations here (link).
Other muscles
I won’t include all the potential SSEs in this article, as the possibilities are many. Resolving the deep six and psoas weakness will cure most of the lumbar plexus compression cases, as long as the postural, breathing and movement improvements are simultaneously worked on and corrected.
You’ll find exercises for the adductors, abductors, iliacus and peroneus longus muscles in my video library, that was linked earlier, or on my youtube channel. For the gastrocnemius and soleus, simply perform seated or standing calf raises (make sure that the toes are relaxed during execution).
Summary
Myofsacial entrapment syndromes such as lumbar plexus compression syndrome are very rarely identified. Even more renowned diagnoses such as thoracic outlet syndrome, which has a very cause, has no diagnostic nor treatment protocol consensus. I am therefore proud to say that the method detailed in this article really works, and have cured many patients with so-called “idiopathic” or diffuse pain patterns.
To identify the muscles that are responsible for the neuralgia, you need to know the anatomy and have decent palpatory skills. Use the reference list provided in this article, to find the spots that are causing the nerve compression.
Rehabilitating the muscles that are causing the neural entrapment must be done both by specific strengthening exercises, and by addressing the underlying postural, breathing and/or movement based dysfunction. The most common ones being swayback posture, lack of lumbopelvic rotation in gait, and breathing dysfunctions.
You will need to be patient, as rehabilitating severely weak muscles may turn out to be a lengthy business. The results will however be favourable, if the assessment and correctives were implemented properly.
Hello,
Can you please re-upload the two missing videos on psoas major exercises. Thank you very much for a most informative article!
Hello,
Can you please re-upload the two missing videos on psoas major exercises. Thank you very much for a most informative article!
Nothing is missing, the old video was deliberately removed. Use the videos which are embedded.
Exhaustive explanations on a “driving crazy”, dulling pain! Great work!
Thanks doc
Exhaustive explanations on a “driving crazy”, dulling pain! Great work!
I have exactly this happening. Extremely weak psoas which I’m working on. The autonomic symptoms are very interesting. Is it reasonable to think that panic attacks could occur as a result?
No. Rather, patients with anxiety tend to develop entrapment disorders such as LPCS. The nerve problem is secondary, and anxiety primary. Not always, but usually.
I have exactly this happening. Extremely weak psoas which I’m working on. The autonomic symptoms are very interesting. Is it reasonable to think that panic attacks could occur as a result?
Thank you very much for this informative article! I may have overlooked this in the reading but is common to have LPCS bilaterally? I had bilateral hip labral repairs with FAI (both side repaired surgically), yet I still suffer from a lot of the symptoms noted in your article. My left side is worse than the right, but my activity is still significantly impared due to post-activity flare-ups. I’m just wondering how often bilateral cases are seen or if they are ever seen. Thank you!!
Very often
Good to know. Thanks so much! Ive been doing the exercises suggested by you, as Ive had muscle testing from an NKT, and so far so good. I’m really hoping this is the answer for me!! Your website and videos are amazing! Thanks again!
Many thanks!
I believe I have an entrapped LFCN. I am having an MRI today. The thought is that if they can’t find it on MRI, they can still locate it via ultrasound and give me a localized injection based on my symptoms. Thoughts? Or just focus on PT? I have had burning in my outer thigh for a month which then progressed to a tight calf and then a cold foot (physically colder).
Imaging is useless for this problem. Injection can relieve symptoms to some degree, but is usually done with diagnostic purposes. LCFN will not cause a cold foot, so there’s definitely more going on here.
Mr. Larsen, I have been searching 40 years for an explanation for my mysterious condition that’s plagued me from head to toe. Recently, I began to be able to isolate and identify my trouble area(S) and in searching, your research came up. Thank you for being easy to find. My medical Drs don’t understand my complaints, the cause of my pain, or how to help me; their pharmaceutical remedies, Chiropractic’s, and ‘physical therapy’ helped little. One Dr wants to take out 4 vertebrae and put in rods, plates, and screws from my neck without examining the rest of my spine (having difficulty walking). I’ve felt trapped in a semi-crippled somewhat numb body, challenged in life by 5 separate semi-traumatic assaults to my musculoskeletal (tiny) frame before the age of 12. At 60, I now have a better level of mobility (better than I can ever remember)… because for the past 10 years (since Chemo&Rad-that and stress possibly exacerbated sx’s) .. I’ve fought past the pain of shortened entrapped twisted-stuck muscles raking over nerves and ligaments rearranging (it feels like), to gain a new level of alignment and flexibility. In the past 5 months, working with a personal trainer, who also had to Rehab himself….along with your research applied, my recovery has sped at the speed of light compared to the last 10 years. I’m encouraged, but my hard work continues as I fight degeneration and notable incorrect spinal curves. Your research has allowed me to understand what I am dealing with…it fits! And your teaching pictures and videos are priceless. A number of your articles have shed light for me. Thank you! Thank you! Thank you!..for helping me toward a better quality of life. JL
Bonjour,
je suis française et je ne trouve pas d’équivalent à votre approche thérapeutique. Pourriez vous m’indiquer des professionnels qui utilisent votre méthode en france ?
merci
Cordialement
No, sorry.
Excellent article. I’ve had scans on my gall bladder, liver, right ovary, bladder (constantly feeling like I had UTI) and hospitalised for suspected appendicitis and all clear. I know my Psoas is the issue, I have nerve pains in the genital area and upper thigh, buttock. I read before the nerves pass through the Psoas major and we can hold a lot of emotions there too, I am peri menopausal and muscles can lose lubrication and get stiff from low Oestrogen, plus hormonal anxiety can make everything tense.
Thanks for this I am going to gently rehab. My physio I go to does provide temporary relief, and she says I need to be doing strength training and work on correct posture. Also as an aside, heavy handbags pulling on our bodies can cause so many issues too. My neck was so stiff and sore, very limited ROM but by doing your neck SCM and Occipital strengthening this has helped so much. Thank you.
Could extra fluid in the psoas bursae cause lumbar plexus impingement the starts after the psoas is under load for 30 minutes? I have an elite cyclist that gets pain in the upper glut and then ant post thigh. Vascular completely ruled out. Mr not impressive except fluid in the bursae. NCS L5 issues? Worth shrinking the bursae with steroids
The psoas bursa is most likely distended due to pectineus tightness. It is known as the iliopectineal bursa. The pectineus crushed this bursa in hip flexion, and iliopsoas in hip extension. Because your patient is a cyclist, it’s more likely to be a pectineus problem.
HOWEVER, the symptoms you’re describing sounds like a typical Maigne’s syndrome (I presume u mean ant lateral thigh, not anterior posterior thigh) which is caused by psoas weakness. Radiculopathy should be ruled out through MRI of the lower back.
The pectineus can also crush the lateral femoral cutaneous nerve and cause neuralgia in the anterolateral aspect of the thigh. If he has a simultaneous L5 root compression, these two could be a potential explanation.
As you see, I need more background information. You’d have to book a session and send me the images etc. I won’t go back on forth on this case here in the comments section.
Thank you for this informative article! Are there any specific exercises for pudendal nerve pain? All the best!
This is answered in the article
Pudendal neuralgia started postpartum, T11/12 central disc protusion, weak hip flexion, hyper lordotic posture. Would you still look at strengthening Psoas?
The treatment for pudendal neuralgia is stated in the article.
Hi Dr Kjetil, Great content. I have a doubt. You wrote that “if the nerve is extremely irritated from top to bottom, it’s likely a disc herniation”, but..before this you wrote that.. “A disc herniation will usually cause a whole dermatome to seem negative when tested with MPPT”. How do you know that it is irritated if the MPPT is negative? Thank you!
Radiculopathy worsens with spinal loading, usually has a positive nerve traction test (eg. lasegue’s). Big hernia will usually cause myotomal weakness which is in consistency with pain level; this isn’t seen in LPES (except quadriceps). MRI correlation is always important.
This is such a great article! I appreciate your wisdome!
1. Can you explain more about anxiety and your statement that, “patients with anxiety tend to develop entrapment disorders such as LPCS. The nerve problem is secondary, and anxiety primary. Not always, but usually.”
Is this because of the postural habits someone with anxiety often has – ribs thrusted forward, anterior pelvic tilt and chest breathing?
2. Are you using much gluteal muscles in the QL exercise?
3. I can’t find the alternate supine QL exercise you mention. Has that been deleted?
Thank you so much!!
1. Read my muscle clencher article
2. Nothing
3. Do the standing one, it is the best. See my youtube channel
Amazing wisdom and experience! These facts you share are valuable intell for dr and patient. Side note: wish you wrote NEWS story’s. No seriously! Thank you so much for your understanding these complex body nerve attributes.
Thank you for the insights! Is it possible LPCS may present itself mostly in the feet and occasionally in the leg? For example in my case: intermittent bi-lateral pins and needles on the soles of the feet that only goes away overnight, and, numbness in the feet and toes when sat with feet up on a footrest, that occasionally extends to the whole leg? I can confirm psoas major and piriformis when provoked by physio are painful to the touch.
Yes
I have to say your article seemed as though it has been specifically written for me. I suffer from several of the examples given. I have and am still having trying times with day to day living. I’ve sought relief in many different ways massage, medicine chiropractics only to have symptoms subside for a little while. If there is something I might be missing I would love to be directed. I’m supposed to be in the prime of my life but it doesn’t seem that way. I’m what they refer to as an old soul that’s been battling illness for most of my time. Any thoughts and or suggestions would be appreciated. Thanks
Sincerely,
Eileen Fiallo
Hi. My thoughts and recommendations are listed in this article. You can schedule a consultation if you want an assessment.
Going around in circles after a kidney nephrectomy on my left hand side and living donor transplant on the right 14 years ago and it appears to be increasingly a degenerative condition. The pain I have migrates on the left and right side psoas in the abdominals up to the lower rib cage where the scar tissue is located on both sides, from the upper hip down to the groin, and causes the piriformis/trocanter in the buttocks and sciatica pain in the thigh. I am guess it is gentiofemoral and ilioinguinal in nature. It often can extend into the knee and all the way down the left side of my leg to the knee and even further down the leg to the foot ending between the big toe and second toe. Ice and heat help but the pain is transitory in the greater region. I can’t take anti-inflamitory meds due to the possible effects on the kidney over time. I have tried stretching and hip strengthening PT for months, exercises to strengthen the hips and lumbar region, but it fixes nothing and can cause more symptomatic pain. Also read that immune suppression meds may compromise and deteriorate the nerve sheath over time? Compression and massage helps, but exercise seems to make it worse especially cycling, as does walking and swimming. I have been diagnosed with mild osteo-arthritis with some boney spurs located in the hip socket and osetoporosis according to MRIs with no disc damage. I am 6’2 inches tall about 212 lbs. Hip replacement has been ruled out because the surgeon believes it is nerve entrapment more than worn cartilage. I am wondering if you have any recommendations? Thank you Doctor for your comprehensive and innovative approach!
“A severely weak muscle usually is a very tight and unhealthy muscle”
Does it mean when the psoas is chronically tight it can bring the posture into hyperlordotic and the only way to calm down this muscle is by strenghtening, is that right?
Tight yes, hyperlordotic no.
Can low back chronic tightness comes from weakness in psoas muscle?
Usually pelvic pain (superior cluneal nerves) or the dorsal rami nerves that affect the paraspinal areas. But frank spine pain, I’d say not directly.
Is bloated stomach one of the symptoms of weakness / atrophy in psoas?
I have resolved a few “IBS” cases from this. Ie., patients whose “IBS” clearly worsened after psoas training (ie. intestinal dysfunction due to neuropathic dysautonomia) and then ultimately imrpoved with time. But I can’t say that this is the most common cause of IBS, I doubt that. But it is a possible differential diagnosis in some patients.
What if stretching the hip flexors helps with low back tightness but increasing pain in front of the hip but on the other hand strenghtening psoas helps so much to calm down that pain in front of the hip but increasing tightness in low back? Is that tightness gonna go away over time once hip fully healed?
No stretching of weak muscles. Even though it often causes temporary releif, it gradually worsens.
42yo female. 5’3″ 145 lbs (but previously 170 lbs and sedentary) The radiologist said mild gluteal tendonopathy. The ortho said greater trochanteric bursitis and IT Band syndrome. PT said everything is tight including my glutes and hip flexors. MRI showed disc desiccation and mild diffuse disc space narrowing. (I also have scoliosis). Spinal doc mentioned meralgia parasthetica and referred me to pain mgmt. Diagnostic block of bipuvicaine was done without imaging guidance and I felt temporary relief. He recommends steroid injection but feels it would be odd to have multiple nerve entrapments at multiple levels due to calf pain so feels maybe an epidural injection at L5-S1 would be good too because it could be the cause of both the radiating thigh pain and the calf pain.
I did the psoas excercise. How many reps and what frequency per day do you advise? Do you perform on both sides?
I have also had negative vascular and vein studies, ruled out DVT, autoimmune, vitamin deficiencies via blood and urine tests, etc. I’ve gone on medical leave and devoted the last 8 weeks to getting answers. The steroid in the GT bursa wasn’t effective, nor is heat, ice, PT, topical creams, various magnesium and potassium vitamins, etc. MP is an elusive diagnosis. We seemed to have ruled everything out and are left with only the idea of nerve entrapment. My inguinal ligament feels squished. LFCN appears to be the cause of the thigh pain but I’m not clear on the pathway and which nerve is causing the calf pain. If you don’t know which nerve is causing the pain it is hard to address the muscle imbalances. I used the directory to find an NKT provider near me but none seem anywhere near as skilled as you (North Dallas, TX).
Do you think I would be a good candidate to consult with you via Skype to determine what my issues are and how to best address them with the correct strengthening exercises?
Super interesting thoughts on how nerve compression can affect autonomic function, thanks.
Between lumbar/psoas/piriformis compression, or neck/thoracic outlet compression, which do you feel has more impact on digestive system/IBS/idiopathic reflux symptoms?
lumbar plexus
I found your article very interesting and an excellent lesson in anatomy, nerve innervation, and solutions. I’ve passed it along to my physical therapist. I’ve had genital pain, burning, tenderness along with inner posterior thigh and lower inner buttock burning 24/7 for almost a year. It started before I had a T10-12 laminectomy (to correct a spinal myelopathy), laminectomy of L2-L5 and L4-L5 fusion 7 months ago for severe spinal stenosis. The back pain and balance has improved but I still have the neuropathy pain that I had before surgery. My neurosurgeon and pain management physician think it is coming from dysfunction in the lumbar or lumbar/sacral plexus. I’m scheduled for a second EMG, but according to your article that is unlikely to diagnose the problem. I’m also getting an injection in the ganglion of impar to try to calm some of the sympathetic nerves. I hope my PT has read your article and can work with me to strengthen my psoas muscle, which we have determined is tight (and therefore weak?). Do you have any further thoughts of diagnostic avenues for injection to pursue in addition to further PT work?
Can LPCS lead to a person being unable to walk because of pain?