Temporomandibular dysfunction or TMD for short, is a condition that may lead to excruciating pain in the jaw joint area. Further more, related symptoms such as such as TMJ clicking, painful jaw muscles, facial neuralgia (trigeminal neuralgia), tinnitus, headaches, migraines are a few worth mentioning (D’Urso et al., 2016; Attanasio et al., 2015; Romero-Reyes & Uyanik, 2014; Franco et al., 2010).
It has been estimated that up to 33% of the population is affected with some kind of TMJ disorder, and between 3-7% are in so much pain that they require treatment. Sadly, there’s no real consensus with regards to the cause nor treatment protocols for temporomandibular dysfunction. In this article, however, I will detail what I consider to be the true cause and cure for TMD, a protocol that I use myself in my clinic on all TMD patients, with overwhelming results.
Approximately 33% of the population has at least one TMD symptom and 3.6% to 7% of the population has TMD with sufficient severity to cause them to seek treatment. – Edward & North, 2009
Patients with chronic TMD frequently report symptoms of depression, poor sleep quality, and low energy. Furthermore, chronic TMD has been found to interfere with normal social activity and interpersonal relationships and to negatively affect the ability to maintain employment. – Morris et al., 1997
Evidence for the effect of electrophysical modalities and surgery is insufficient, and occlusal adjustment seems to have no effect. One limitation of most of the reviewed systematic reviews was that the considerable variation in methodology between the primary studies made definitive conclusions impossible. – List & Axelsson, 2010
The true cause of TMD
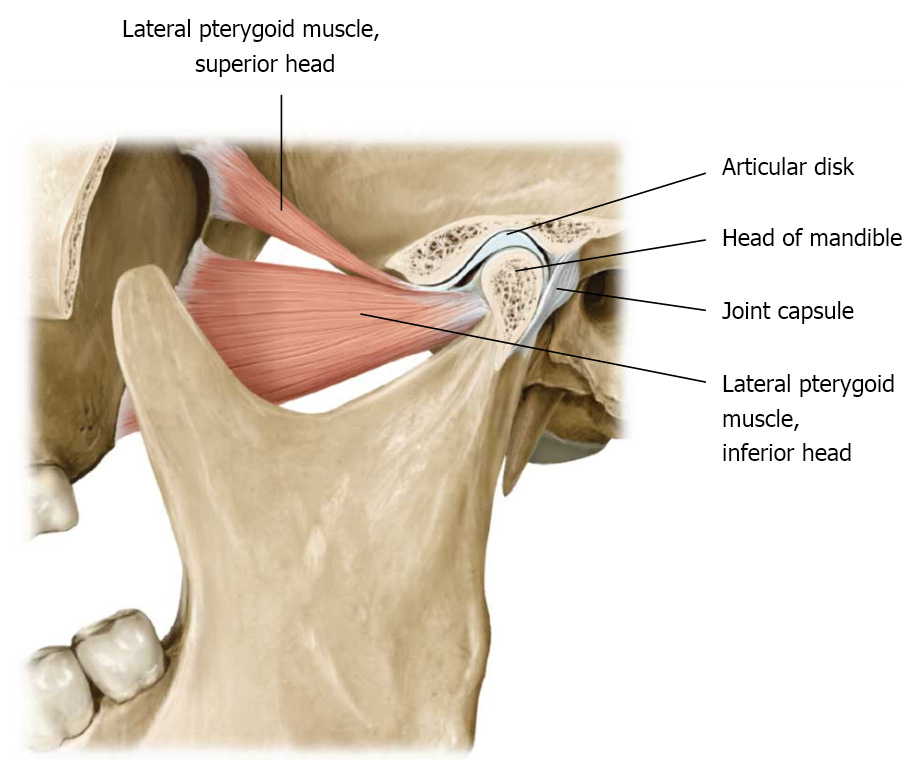
Fig. 1

The true cause of temporomandibular dysfunction, is habitual retraction of the mandible, jamming the glenoid fossa (joint socket). Underdevelopment of the maxilla bone (upper jaw), improper tongue posture, mouth breathing habits and similar will establish an excessively posterior tooth occlusion, and thus encourage posterior translation of the mandible, ultimately jamming it into the joint socket, causing deterioration over time.
This video does illustrate the cause of TMD well. It does not, however, mention the causes of horizontal underdevelopment of the maxilla; improper tongue posture. Pacifiers, thumb sucking and chewing overly soft foods in our youth, inhibits horizontal growth of the maxilla, leading to a more posteriorly established dental occlusion. The mandible (lower jaw) keeps growing into its full potential, even when the maxilla did not. The result of this is a mandible that is proportionally longer than the maxilla, which often lead to TMJ compression and TMD if postural occlusion is to be maintained. The more underdeveloped the maxilla is, the more compressed the TMJ joint socket will become, as the differential of length ratio between the two parts increase.
From a postural perspective, a whole different approach seems logical and almost too simple. When they bite together, the joint [when dysfunctional] is not centric, so is not balanced; it’s over-closed, with the head of the jaw joint set in the top back of the joint often squeezing the disk out of the way, possibly causing great damage. – Dr. Mike Mew
When the maxilla and mandible do not achieve their genetic potential in length, width, or vertical position, the effects are seen in mal-relationships and dysfunctions in the patient’s tissues, bones, muscles, and nerves. The temporomandibular joint (TMJ) relationship may then become compromised when this occurs, as it compensates for the discrepancies in normal growth and development. Normal spacing between the roof of the glenoid fossa of the temporal bone and the condyle of the mandible should be approximately three mm to support the disk between them. The retrodiskal tissues originate from the distal portion of the glenoid fossa and are inserted into the posterior portion of the disk. This tissue contains a matrix of blood vessels and nerves, particularly fibers of the auriculotemporal nerve, cranial nerve V, an afferent branch of the trigeminal nerve. If this space is insufficient or reduced or restricted and the condylar head grows posterosuperiorly or is iatrogenically repositioned posteriorly or posterosuperiorly, the condyle will pinch this tissue and usually the result will be pain. – Sims & Stack, 2007
Adults with clicking joints had a saggitally shorter maxilla and mandibular diagnonal, whereas adults with crepitating joints had, in addition, a shorter anterior and posterior cranial base and pharynx. This sagittal “shortness” could already be demonstrated for many of the reported dimensions at the corresponding cephalograms taken about the age of 12.5 years, and did not appear to have changed much over time. It is concluded that the reported TMD signs in adults were associated with a sagittal shorter midface. – Dibbets & Weele, 1996
Fig. 2
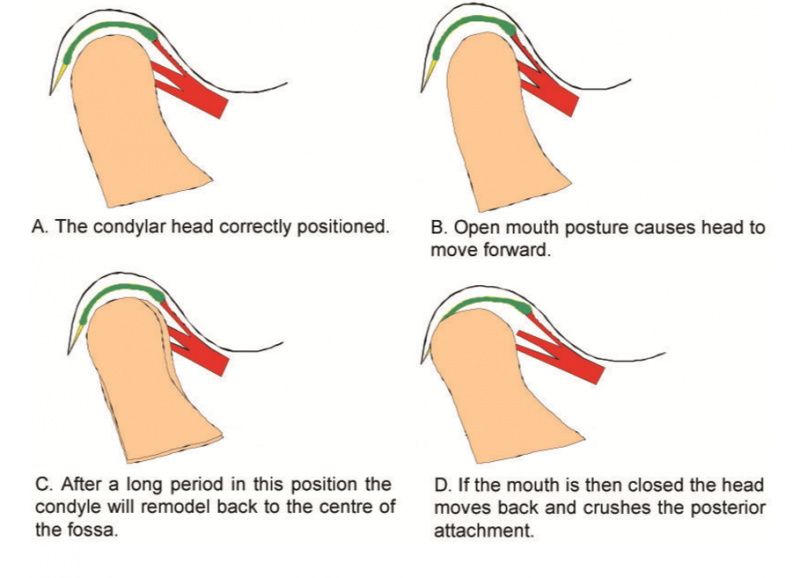
It is very important to understand that the TMJ is not a hinge joint. Most dentists, and even so called “TMD specialists” believe that the mandibular condyle should rest in the posterior position of the joint socket. This is absolutely wrong. The TMJ is an elliptical joint, allowing movement in all directions, from center. It is absolutely critical to understand that a centrated TMJ is equivalent to slight protraction of the mandible, and not maximal retraction; it should rest a minimum 2-4 millimeters more anterior than complete retraction, preferably more.
Fig. 3
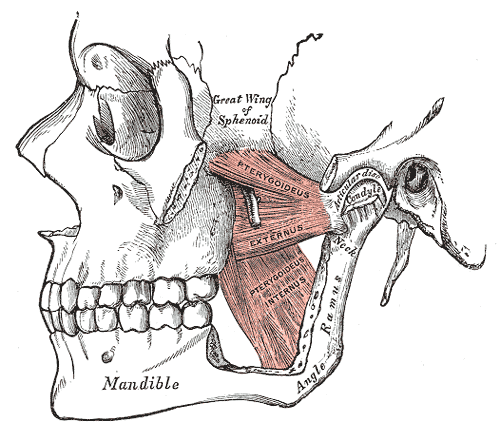
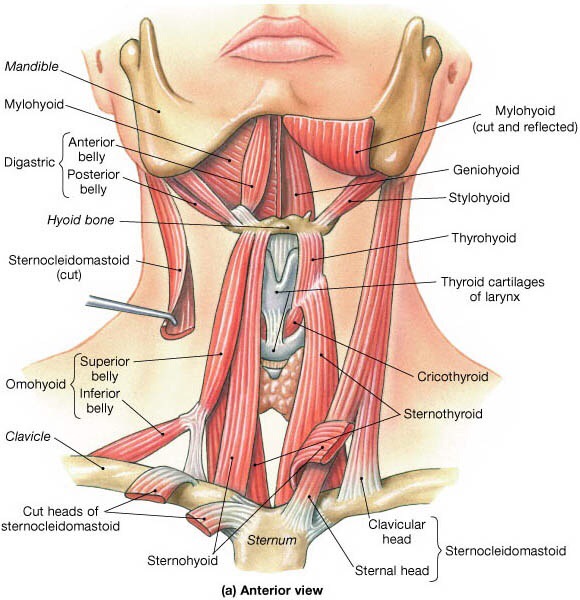
When the mandibular condyle rests too far back in the glenoid fossa (socket), this may lead to an array of issues, as mentioned earlier. We will speak more about the causes of this, but one important reason is that the pterygoid muscles will inhibit (become inactive). The pterygoid muscles are have very important functions, as they pull the mandible forward (anteriorly). Anterior translation of the mandible = unjammed / decompressed TMJ, right? Yes, indeed.
The lateral pterygoid controls protraction (forward translation) of the mandible during opening of the mouth. Ipsilaterally, it also rotates the jaw toward the other side (longitudinal axis). It has two heads; a superior and inferior portion. The medial pterygoid on the other hand, controls protraction during closing of the mouth. It also shifts the mandible contralaterally. Because these muscles protract the jaw, they become inhibited when the jaw is habitually retracted in posture.
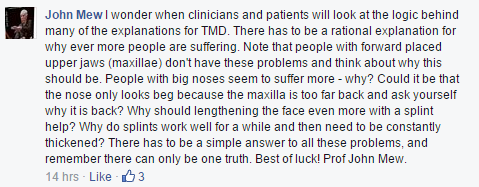
Fig. 4 – Professor and TMJ-surgeon, Dr. John Mew
The studies below show that there are no official beneficial diagnostic or treatment protocols with regards to TMD. It is therefore not very surprising that the researchers also do not find any significant difference between psychological treatment and physical treatment, when they didn’t know the cause in the first place.
This review aims at presenting a current view on the most frequent factors involved in the mechanisms causing temporomandibular disorders (TMD). The etiology of TMD is multidimensional: biomechanical, neuromuscular, bio-psychosocial and biological factors may contribute to the disorder. Occlusal overloading and parafunctions (bruxism) are frequently involved as biomechanical factors; increased levels of estrogen hormones are considered biological factors affecting the temporo–mandibular-joint. Among bio-psychosocial factors, stress, anxiety or depression, were frequently encountered. The etiopathogenesis of this condition is poorly understood, therefore TMDs are difficult to diagnose and manage. – Chisnoiu et al., 2015
No evidence was found to distinguish the clinical effectiveness between «usual treatment» and psychosocial interventions for myofascial TMD pain. – Roldán-Barraza et al., 2014
There are some studies showing significant improvement by utilizing some methods, although lacking consensus. It is however important to note that they are talking about symptom relief, and that they are not aware of the cause of TMD, in similar fashion to the above-mentioned studies. At the very least, postural correctives are portrayed as something positive – which they absolutely are, when done correctly.
This systematic review concluded that “active and passive oral exercises and exercises to improve posture are effective interventions to reduce symptoms associated with TMD. – McNeely et al., 2006
This systematic review analyzed studies examining the effectiveness of various physical therapy interventions for temporomandibular disorder. Active exercises and manual mobilizations may be effective. programs involving relaxation techniques and biofeedback, electromyography training, and proprioceptive re-education (bevegelseskorrigering) may be more effective than placebo treatment or occlusal splints. A combinations of active exercises, manual therapy, postural correction, and relaxation techniques may be effective. – Medlicott et al., 2006
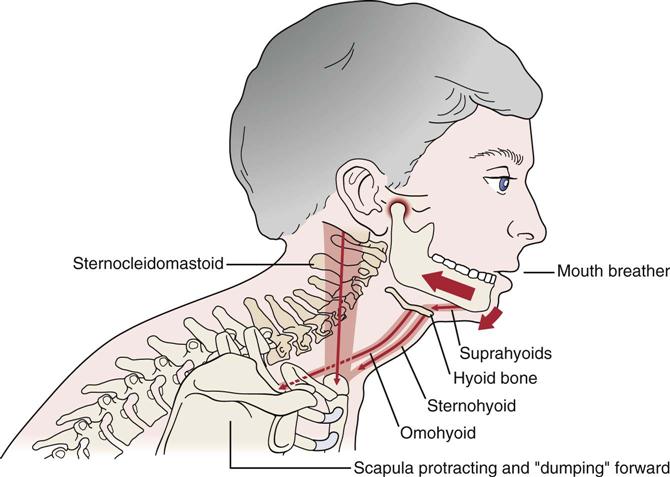
Why forward head posture encourages TMD
There is a high correlation between foward head posture (FHP) and temporomandibular dysfunction. The reason is because the mandible is attached to the sternum through the hyoid musculature. The further forward the head translates, the higher the tension of posterior mandibular pull through the hyoid structures will become. The added posterior retractive forces on the mandible will exacerbate the existing dysfunction, which is caused by underdevelopment of the maxilla, leading to a double compression force to the temporomandibular joint. This especially applies for mouth breathers and people with open-mouth postures, as the hyoidal posterior mandibular pull will not have great effect if occlusion is intact.
Special emphasis has been put on the influence of forward head posture on the craniofacial growth as it can determine a morphoskeletal and neuromuscular pattern leading to a dysfunctional condition. A correlation is established between Class II Occlusion, forward head posture, and craniomandibular dysfunction. The concept of craniocervical postural position is defined, as well as its close relation to the mandibular postural position. – Gonzales & Manns, 1996
It is possible to treat TMD without dealing with the craniocervical position, but it makes it harder to maintain proper mandibular resting position due to the retractive forces imposed by the infra- and suprahyoid stretching that occur when the head is forward. Let us have a closer look at common postural myths, and how to really correct FHP.
Fig. 5
To correct forward head posture, one must also address general postural sway. If the point of gravity is too far back, as with the utmost common swayback posture, the head and shoulders will naturally come forward in order to maintain equilibrium. No amount of cervical corrective procedures will ever be able to correct this! The point of gravity must be altered in order to be able to change and promote proper craniocervical resting position.
I must emphasize that no amount of exercising can ever fix postural anomalies. It’s a complete myth. The only way to permanently alter posture, is by altering habits. In other words, you need to get into proper position, and get used to staying there. Sure, exercises can help with making this process easier, but habits (posture) and exercises must both encourage proper function. The simplest way is by making sure of the following:
- The chest must be in line with, or anterior to the hip. The shoulders should never be posterior to the hip.
- The shoulder smust be raised slightly (half an inch), to avoid clavicular depression, if they are indeed depressed.
Swayback posture and clavicular depression both contribute to forward head posture. By maintaining proper thoracopelvic and clavicular alignment, this will lay the foundation for proper craniocervical posture, making it easier to maintain good structural habits. In practice, all you need to do is get your hip slightly backward, chest slightly forward, and shoulders slightly upward. Then stay there. You’ll get used to it within 4-8 weeks. For more information on thoracopelvic correctives, look into my lower back article.
Fig. 6

The TMJ’s relation to body posture
I’ve written a long article about the TMJ and its relation to body posture in my atlas-article (link – coming soon). The point is, though, that imbalanced occlusion and open-jaw postures will encourage both forward head posture due to loss of tensegrity of the hyoid musculature that pull the head into flexion when the mouth is closed, and encourages rotation of the atlas, most likely due to the occlusive state’s effect on the sphenoid bone that the optic nerves (CN2), as well as CN3, CN4 and CN6 pass through. The relation between occlusion and sphenoidal alignment, is formed by the temporalis and pterygoid muscles that attach to it.
It is however important to note, that even if you have a very crooked occlusion, you are not doomed to live with horrible posture. Our consciousness and habits may override the body’s automatic postural “baseline”, meaning that we can get out of forward head posture or pelvic imbalances by simply being aware of it and avoid letting it happen. You will most likely need to be taught how to do that, but it’s definitely possible and is something I teach my clients daily in clinic.
Fig. 7
A clear pattern of associations between crowding and craniocervical posture was found. – Solow et al., 1998
According to the literature reviewed, we believe that there are real correlations between posture and the SS (stomatognathic system). In this way, an increase in postural swaying may indicate a general malaise caused by problems in the SS. – Cuccia et al., 2009
The individual’s postural position can suffer biomechanical alterations due to stomatognathic alterations, causing clinically visible changes in dysfunctional individuals and affecting the performance of the involved structures. – Strini et al., 2009
Significant correlations could be obtained with respect to the facial axis and the lordotic angle, the facial axis and the pelvic inclination, the inner gonial angle and the lordotic angle, the inner gonial angle and the pelvic inclination, the mandibular plane angle and the lordotic angle, the mandibular plane angle and the pelvic inclination, as well as the facial depth and the pelvic inclination. – Lippold et al., 2006
Five animals received no alteration on their bite. Bite was increased on 10 animals and molar teeth were extracted on 10 other animals. Frontal and lateral radiographs were taken on days 0, 7, 14 and 21. Distances from landmarks to a true vertical line were measured on both radiographs. Results: Repeated measures analysis showed statistically significant differences between the amount of the curvature at the cervical and thoracic spines on frontal and lateral radiographs over time Ramirez-Yanez et al 2014
The data that is available points to the existence of a correlation between posture and occlusion and also asserts the prevalence of associations between cranio-facial anomalies and idiopathic scoliosis in adolescents. – Amat et al., 2009
The data confirmed a beneficial effect of balancing the occlusion with an acrylic wafer on the following paired postural muscles: sternocleidomostoid, erector spinae, and soleus. – bergamini et al., 2008
Based on these findings, it was concluded that changing mandibular position affected body posture. Conversely, changing body posture affected mandibular position. – Sakaguchi et al., 2007
Identification of dysfunction
Identifying TMD itself is not difficult. Reduced horizontal maxillary growth is indicated by an unproportionally bigger and more protruding nose than the cheeks, and reduction of the naso-maxillary line. This is, however, something that dentists and people with special orofacial interests may pay more attention to. It’s really not that important, in order to deal with TMD itself. Check out dentists Mike and John Mew’s youtube channel for more information on this.
Fig. 8

First off we have the symptoms, also mentioned earlier: jaw pain, myofascial pain in the chewing muscles such as temporalis, masseter and pterygoids, headaches, tinnitus, trigeminal neuralgia, etc. There may of course also be more symptoms, but they are not as common as the ones mentioned.
The ultimate TMD assessment technique, is measuring the distance between resting mandibular position and maximal retraction. Its resting position is usually maximally retracted already, crushing the TMJ socket for each day that passes. Additionally, the jaw will most of the time be unable to protract when opened, causing further posterior shearing forces into the joint socket and TMJ articulate disc.
Here’s what you do:
- Close your jaw with full occlusion (molar contact).
- Relax the jaw without moving it.
- Try to retract (pull back) the mandible.
If it moves minimally, or not at all, that means the mandibular resting position is causing the condyle to jam into the TMJ, often leading to pain, disc injuries, arthritis and so on over time. In other words, the occlusive state is causing chronic joint deterioration and must be altered, either by posturally moving the jaw forward, or expanding the maxilla horizontally. As a myoskeletal therapists, the first mentioned is my approach. A dentist who really knows how to deal with TMD, will probably choose the latter. There are also some splint therapies, such as Starecta, that supports mandibular protraction.
Fig. 9

The next step is to assess its movement. It is important to teach a dysfunctional jaw how to move properly, especially with regards to protraction, as this movement is often (always) inhibited. To identify improper opening and closing of the jaw, watch yourself in the mirror (or your patient) and look for mandibular retraction as the mouth opens. This is an unnatural way for the mandible to articulate within the joint socket, and will often lead to laxity of the TMJ capsular ligaments over time, causing anterior displacement of the mandibular condyle. If present, it will reveal itself as a bulge appearing anterior to the jaw joint, as illustrated in the picture below when the mouth opens to a certain degree. The bulge is the mandibular condyle subluxing anteriorly.
Once again, the mandible should protract (come forward) when the mouth opens, and not reflexively retract. The latter is what I almost always identify in people with temporomandibular dysfunction. You can also watch for left or right deviation as the mouth opens. The direction it deviates to indicates higher TMJ compression on that side, although many experience TMD bilaterally.
Fig. 10 – Red arrow=subluxing condyle, black arrow=mandibular retraction

Sadly, many therapists teach their patients to force greater mandibular depression (mouth opening) as an exercise, if mouth opening is restricted. This is highly detrimental and must not be done! The cause of reduced mandibular depression is improper TMJ articulation (lack of protraction) and not a simple “tight muscle”-problem. Patients who are exposed to these quacky protocols will end up getting worse and not better, as the TMJ is crushed due to lack of mandibular protraction! The TMJ restrictions are infact the body’s way to try to hinder further damage and excessive compression to the joint socket.
On the other hand, this is how optimal TMJ kinematics should look like, in the picture below. The mouth opens by encouraging downward and forward translation of the mandible, by utilizing the hyoid and pterygoid muscles. Also note the lack of bulging of the mandibular condyle, which does not displace when the TMJ is healthy and used normally.
Fig. 11

Here’s a video walkthrough of proper and improper TMJ mechanics.
Common sideeffects of TMD
Habitual excessive retraction of the mandible will often cause many secondary effects. I will address the most common ones here below.
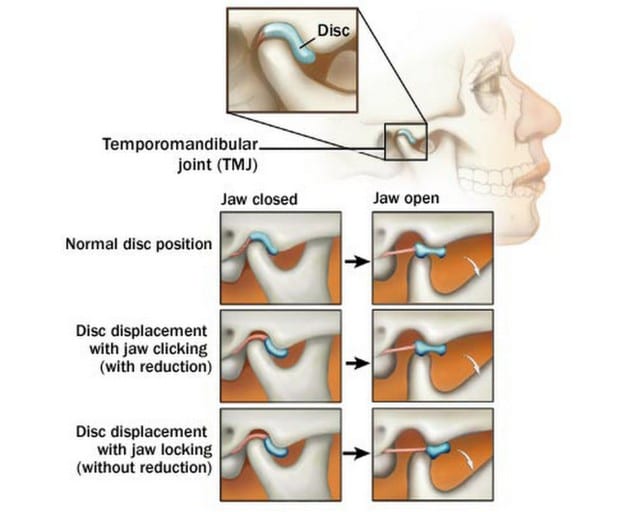
Articular disc displacement
A common sideeffect of TMD, is articular disc displacement. The articular disc is a structure that lies between the mandibular condyle and temporal bone (joint socket). Its function is to glide forward and backward in symmetry with the condyle’s movement, covering the condyle from grinding bone into bone. When the TMJ is compressed by an excessively posterior position of the mandibular condyle, the ligament (the retrodiscal tissue) that’s holding the disc may gradually degenerate, eventually causing the disc to slip forward in front of the condyle.
There are two main types of displacement: with, and without reduction (WOR). “With reduction” means that the mandibular condyle is able to pop back onto the disc, causing the infamous “pop” as the jaw opens. If the disc is severely displaced, it may be unable to slide back into position between the temporal bone and mandibular condyle as the mouth opens, and this scenario is referred to as “without reduction”, which sometimes cause the joint to lock up or greatly restrict in mobility.
Should we worry about disc displacements? Well, first of all it has been shown that patients with displacement WOR usually (~70%) resolve on their own, within a certain period of time. Surgery, rehab (of course, rehab without consensus), medication and psychological treatment were all found to be equally effective (or should I say ineffective) for treating TMD and disc displacement, indicating that the actual displacement is an unlikely cause of the pain by itself. Reports also note that the retrodiscal tissue may harden and create a ‘pseudodisc’ function. Additionally, scientists have conducted experiments where they purposely injured the retrodiscal tissue in goats, finding it to be reformed a month later. Why? In my view, because the goat doesn’t have the predisposing factor of TMD; TMJ compression due to continuous retraction of the mandible, and of course because the retrodiscal tissue has a decent vascular supply. Sure, the tissues were weaker (scar tissue), but this doesn’t really matter. The point is that the disc heals if there’s no continuous irritation to the joint, and the same applies, of course, to humans. Once the continuous injuring effect cease, the disc can heal.
If there has occurred retrodiscal tissue perforation, meaning that the tissue is completely torn, then this requires surgery.
Fig. 12
Clinical evidence and previous experimental animal work suggest that mandibular condylar cartilage shows the capacity for repair, after trauma or degeneration, that can reconstitute a functional articular surface; a facility not shared by other synovial joints. This study aims to test the regenerative capability of condylar cartilage in the repair of standardised full-thickness articular defects, and thereby to test the hypothesis that the healed wounds comprise tissues identical in form and composition to those of similar, but uninjured areas. The results showed reconstitution of all tissue elements of condylar cartilage within 6 months of injury. – Robinson, 1993
MRI of a 30-year-old woman 1 year after discectomy showed a residual disc-like tissue. The observation was initially confusing, but a close comparison of pre- and post-operative images suggested that the inferior wall of the anterior joint capsule had migrated superiorly after the removal of the disc and mimicked a residual disc on the follow-up MR images. – Petersson et al., 2005
The result of this prospective cohort study indicated that approximately 40% of patients with symptomatic disc displacement without reduction will be free of symptoms within 2.5 years, one-third will improve, whereas one-quarter will continue to be symptomatic. This knowledge should be valuable for the treatment planning and evaluation of prognosis of patients with non-reducing symptomatic disc displacement. – Kurita et al., 1998
This result demonstrates that therapeutic exercise brings earlier recovery of jaw function compared with splints. – Haketa et al., 2010
These results suggest that ADDwor subjects will improve with only minimal treatment intervention, and no significant difference was evident for the treatments tested and the control condition. – Minakuchi et al., 2001
MR images depicted anterior disc position in 32% of the asymptomatic joints (8/24 males, 5/18 females). Anterior disc position in asymptomatic subjects may be a predisposing factor to TMJ dysfunction or simply an anatomic variant whose prevalence must be considered when evaluating TMJ dysfunction. – Kircos et al., 1987
For individuals with temporomandibular joint (TMJ) disc displacement without reduction with limited mouth opening (closed lock), interventions vary from minimal treatment to surgery. In a single-blind trial, 106 individuals with TMJ closed lock were randomized among medical management, rehabilitation, arthroscopic surgery with post-operative rehabilitation, or arthroplasty with post-operative rehabilitation. Using an intention-to-treat analysis, we observed no between-group difference at any follow-up for CMI (p > or = 0.33) or SSI (p > or = 0.08). Both outcomes showed within-group improvement (p < 0.0001) for all groups. – Schiffman et al., 2007
Retrodiscal tissue of female goats received trauma or sham trauma. Following a healing period of 30 days, the tissues were pulled to failure on an extensometer. Thirty days after surgical section of retrodiscal tissues, the tissue had reformed, but the composition and biomechanics were substantially changed. Healed tissue manifested less than half the strength of normal tissue. – Cooper et al., 1999
The purpose of this study was to evaluate histologically the healing potential of surgical incisions placed in various areas of the TMJ disc and retrodiscal tissue. Eight weeks after surgery, it was found that incisions completely within retrodiscal tissue had healed and had a normal appearance. Incisions at the junction of the disc and retrodiscal tissue also had healed, but at a slower rate and with more random orientation of the collagen fibers. Defects within the disc had not healed, however, and degenerative changes had developed in the hard and soft tissues. – Wallace et al., 2010
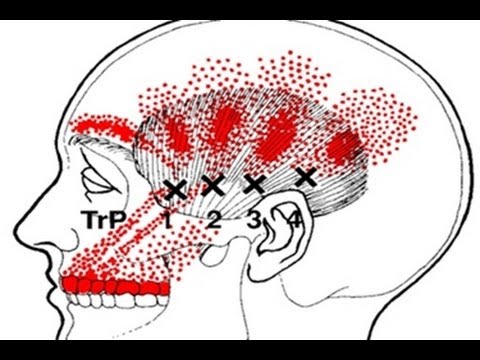
Headaches
The most common cause of TMD-related headaches are caused by the temporalis muscle, in my experience. Continuous retraction of the mandible will cause great imbalances between the muscles of mastication, often leaving the very strong masseter (a muscle that protracts the jaw) underused, overburdening the temporalis muscle (that pulls the mandible back / retraction). In addition to further the compressive forces in the TMJ, it will often cause trigger points in the temporalis muscles that cause headaches.
Although it may be beneficial to treat these trigger points, either by massage or needling, it will not really address the cause of the dysfunction; improper mandibular resting position and articulation. Proper resting position and mandibular movement must occur for the temporalis overuse to cease and the trigger points to disappear for good.
Fig. 13
The results indicate in the studied sample of cervicogenic headache patients, 44.1% had TMD. The group that received additional temporomandibular manual therapy techniques showed significantly decreased headache intensities and increased neck function after the treatment period. Based on these observations, we strongly believe that treatment of the temporomandibular region has beneficial effects for patients with cervicogenic headaches, even in the long-term. – Von Piekartz et al., 2011
Trigeminal neuralgia
The trigeminal nerve is the fifth and biggest cranial nerve, innervating a great load of structures. It has both somatic and autonomic innervations. The trigeminal ganglion spreads out and becomes three main parts called the ophthalamic (V1), maxillary (V2) og mandibular (V3) branches. It is mainly responsible for sensory feedback in the face, and motor functions with regards to mastication.
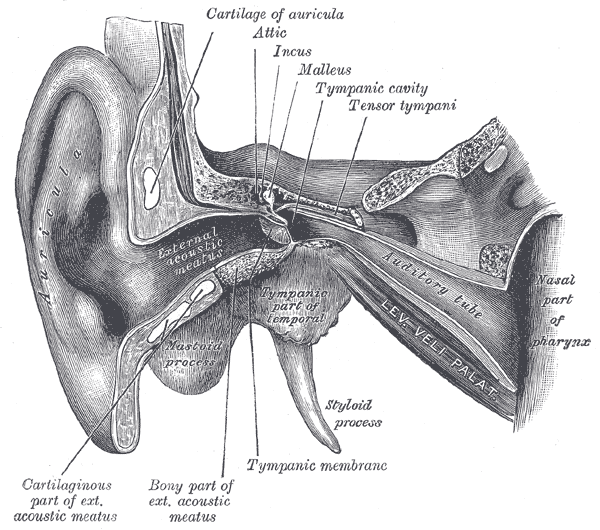
Symptoms of affection may vary greatly. Facial numbness, excruciating headaches, lightning type pain into the face and head, tinnitus, involuntary tear secretion, salivary gland pain, hyperacusis, hearing loss, palatal numbness, and more, are potential symptoms that I’ve seen in my office. Some of this occurs due to the trigeminal nerve’s relations to the pterygopalatine and submandibular ganglions that spreads into the salivary & lacrimal glands, palate, and due to its control over the tensor tympani and tensor veil palatini muscles which controls sound modulation in the ear.
Fig. 14
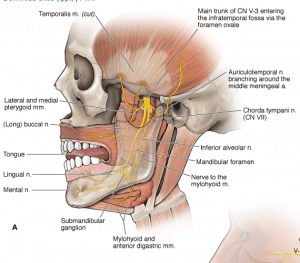
There are two main entrapment points for the trigeminal nerve. One is behind the mandibular ramus; the auriculotemporal part of the V3 mandibular branch (this is also called “Costen’s syndrome”). Excessive retraction of the mandible may compress this nerve between the mandibular ramus and temporal bone. This can be confirmed either by purposely retracting the jaw during opening and closing of the mouth, or by pushing into the nerve manually with your fingers. If this reproduces the symptoms in question, it is indeed affected, meaning it’s being compressed due to a continuously retracted position of the mandible. Information on how to deal with this is the main topic of this article, and will be addressed shortly, in the ‘Correctives’ section.
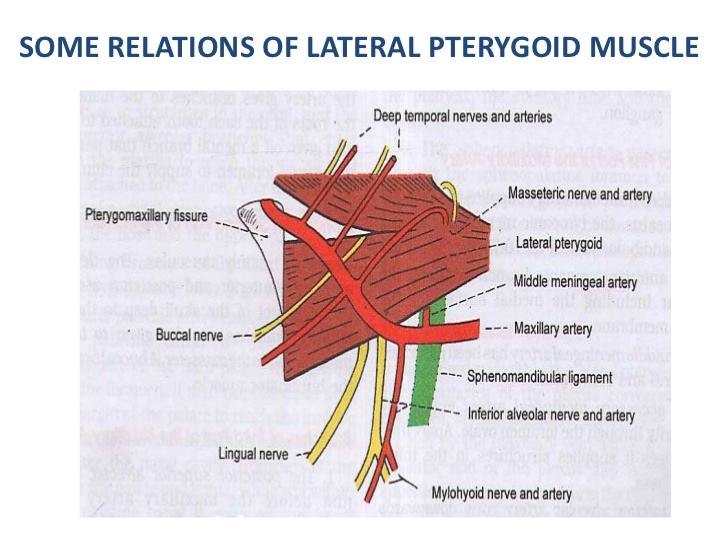
Secondly, the buccal nerve may be entrapped between the superior and inferior heads of the lateral pterygoid muscle. The buccal nerve is yet another part of the V3 mandibular branch, and may lead to the same symptoms as already mentioned, as nerve compression almost always spread to nearby structures (i.e sciatic compression within the piriformis spreading to the calf). Confirmation of this nerve’s affection may be performed by forcibly protracting the jaw against a resistance (don’t cheat by clenching your hyoid muscles). If the pain is reproduced, the buccal nerve is probably entrapped.
To solve buccal nerve entrapment, you need to strengthen the lateral pterygoid. You may massage it to get some relief, but it will always return, as the real cause (weakness, and habitual retraction of the mandible) hasn’t been dealt with. Symptoms may worsen initially, but that’s a normal part of rehabbing the muscle and is a positive sign that you’re doing it correctly. Don’t go harder than necessary, strengthen it gradually and the symptoms will resolve eventually, usually within a month or two.
Fig. 15
MANDIBULAR joint neuralgia (Costen’s syndrome), first reported by Costen in 1934,1 is accepted by otorhinolaryngologists and members of the dental profession as a definite clinical entity. It should be considered in every differential diagnosis of recurring facial pain. – Beyes & Teich, 1952
According to the author’s hypothesis, the lack of posterior support of the alveolar ridge led to mandibular vertical height loss which caused a slipping backward of the condyles over the articular disc thus resulting in TMJ discal damage, erosion of the glenoid fossa bone, compression of the Eustachian tubes and tympanic plates and consequent impingement of the auriculotemporal nerve (ATN), which runs on the postero-medial aspect of the TMJ capsule, and chorda tympani nerve4 . – Paparo et al., 2008
Normal spacing between the roof of the glenoid fossa of the temporal bone and the condyle of the mandible should be approximately three mm to support the disk between them. The retrodiskal tissues originate from the distal portion of the glenoid fossa and are inserted into the posterior portion of the disk. This tissue contains a matrix of blood vessels and nerves, particularly fibers of the auriculotemporal nerve, cranial nerve V, an afferent branch of the trigeminal nerve. If this space is insufficient or reduced or restricted and the condylar head grows posterosuperiorly or is iatrogenically repositioned posteriorly or posterosuperiorly, the condyle will pinch this tissue and usually the result will be pain. – Sims & Stack, 2007
Our clinical work suggests that the auriculotemporal (AT) nerve, a branch of the mandibular nerve, the largest of the three divisions of the trigeminal nerve, plays a critical role in TMD sequelae. The AT nerve provides the somatosensory fibers that supply the joint, the middle ear, and the temporal region. By projecting fibers toward the otic ganglion, the AT nerve establishes an important bridge to the sympathetic system. As it courses posteriorly to the condylar head of the TMJ, compression, injury or irritation of the AT nerve can lead to significant neurologic and neuro-muscular disorders, including Tourette’s syndrome,Torticolli, gait or balance disorders and Parkinson’s disease. Subsequent irritation and compression of the AT nerve can occur, with associated parasthesia, pain and discomfort. Symptoms can be local and specific (e.g., TMD), as well as varied and systemic (e.g., neurologic, dystonic and neuro-muscular disorders, including tremors, muscle spasms leading to impaired and awkward positional control of the head, hands, other extremities, speech impairment, incontinence, impaired sleep, associated depressive symptomatology). – Demerjian et al., 2011
Anatomical relationships between the auriculotemporal nerve and the muscles of mastication, temporomandibular joint, and surrounding vessels in the area of the infratemporal fossa create favourable conditions for entrapment syndromes. Entrapment of the auriculotemporal nerve plays a role in the pathogenesis of temporomandibular joint pain syndromes, headaches, as well as pain symptoms or paraesthesias within the external acoustic meatus and auricle. Komarnitki et al., 2012
The syndrome of symptoms (Table 1) as first described by Costen, an American otolaryngologist, was discussed. Costen attributed the symptoms to temporomandibular joint dysfunction consequent upon mandibular overclosure with distal condylar displacement. He assumed that the displaced condyle might lead to any of the following: Compression of the eustachian tube, erosion of the glenoid fossa or tympanic plate, pressure on the chorda tympani, or pressure on the main trunk of the auriculotemporal nerve. – Clarke, 1962
When a primary otologic cause is discarded in the diagnostic workup for tinnitus, vertigo, hypoacusis, hyperacusis, ear pain, or sensation of occluded ear, TMD may be the cause of these symptoms. Among patients with this dysfunction, the prevalence of ear pain, tinnitus, and dizziness varies between 33 and 76%.25 – de Moraes Marchiori et al., 2014
This study was undertaken in a retirement town, and the mean age of these TMD study patients was a mature 49.1 years. The data likely underrepresent the occurrence of TMD in younger adults. In the Figure, the statistical mode in the study group was 40 to 49 years; it was 60 to 69 years in the control group. The older control group would be expected to have an increased prevalence of recruitment hyperacusis, tinnitus, hearing changes, disequilibrium, and dysesthesias because these conditions increase with age. – Cox, 2008
Symptoms consistent with TTTS can include: a sharp stabbing pain in the ear; a dull earache; tinnitus, often with a clicking [11,12], rhythmic or buzzing quality; a sensation of aural pressure or blockage [8,9] tympanic flutter [13] pain/numbness/burning around the ear, along the cheek and the side of the neck; [7,8], mild vertigo and nausea [8,9]; a sensation of “muffled” or distorted hearing [14] and headache. Central pain sensitization can develop from chronic trigeminal neuralgic TTTS-induced pain. Tensor tympani spasm has been implicated in a range of conditions including Meniere’s disease, for which sectioning of the tensor tympani muscle has been a suggested treatment [15,16] and the secondary otologic symptoms, such as tinnitus, ear pain and other symptoms in and around the ear, which can develop in myofascial pain syndrome [16,17] temporomandibular disorder (TMD) and TMJ dysfunction [8,9,18,19]. – Westcott et al., 2016, Hyperacusis-induced Pain: Understanding and Management of Tonic Tensor Tympani Syndrome (TTTS) Symptoms
Dystonia & Tourette’s
Dr. Antomy Sims, DDS (et al., 2007) has written extensively about the connections between the underlying connections between the jaw, trigeminal dysfunction and its impact on other cranial nerves. He believes, and has proven with several patients, that removing the compression imposed on the auriculotemporal nerve caused by a too posteriorly positioned mandibular condyle will cure dystonia and tourette’s.
He believes that chronic noxious (damage) input to the auriculotemporal nerve caused by TMJ compression will cause signalling dysfunction between the trigeminal ganglia, subnucleus caudalis and the other cranial nerves, and that this is what caused involuntary movement of the neck, eyes, coughing, utterances, and so on. By decompressing the trigeminal nerve, he has seen that these symptoms vanish completely.
Constant stimulation of the auriculotemporal nerve (CN V) may then result in the stimulation of CN’s V, VII, IX, X, via crossover interneurons (ephapses) and other neural elements in the reticular formation. All of these nerves are intimately involved with movement disorders. In summary, we find that chronic noxious input via the auriculotemporal nerve causes reflex reactions with CN’s V, VII, IX, and X via the crossover pathways at various segmental levels within the spinal cord.
All patients showed a total discontinuance of their movement disorders immediately. All patients stated that their breathing was improved and better. All patients stated they did not have the urge to tic or make their involuntary movements. An upper appliance was made for the seven-year-old patient and again, the movement disorder ceased. – Sims & Stack, 2007
If the connection proposed by Dr. Sims et al is true, I believe these same results can be achieved without any dental appliance at all, but by simply altering the postural resting position of the mandible, as well as rehabilitating the lateral pterygoid muscles. Now, I have not had any dystonic or tourette’s patient in my clinic so far, but I think this was interesting enough to mention in this article.
Ménière’s disease
Several studies suggest a connection between temporomandibular disorder and ménière’s disease, which is not surprising, considering the close relationship between the trigeminal nerve and TMD. The trigeminal nerve is involved controlling the eustachian tube, and dysfunction of the latter has been strongly associated with ménière’s disease. Problems with the cervical spine may contribute to dysfunction of the eustachian tube, which I have written about in detail in my atlas joint article.
Irritation of the trigeminal nerve, most likely caused by impingement of its auriculotemporal branch due to TMD, can thus affect the eustachian tube’s function to such a degree that attacks of vertigo occur. So, by decompressing the trigeminal nerve, the noxious input will cease, and the jaw’s impairing effect on the eustachian tube will be resolved.
Fig. x

Unquestionably, the upper cervical spine, the temporomandibular joints, the eustachian tube, and the autonomic nervous system can contribute to the global symptom complex of Ménière’s disease. The eustachian tube is suspected to be the critical link. It has quite a remarkable representation of sensory neurons. This system could be activated through an axon reflex of the mandibular branch of the trigeminal nerve that innervates the temporomandibular joints and upper cervical facet joints. The autonomic nervous system, particularly the sympathetic portion of the autonomic nervous system, can be activated by a neck and temporomandibular joint disorder, and this combination can have the effect of neurogenic inflammation in the eustachian tube, with the consequence of reduced middle-ear ventilation.- Franz & Anderson, 2007
TMD patients often have associated complaints. Many of these patients complained of masticatory fatigue (40%), stiffness (20%), swelling (12%), and weakness (18%) in spite of no observable cranial nerve deficit. Otologic symptoms are also commonly reported among TMD patients. Many of these patients reported tinnitus (42%), ear pain (42%), dizziness (23%) and diminished hearing (18%). – Wright & Bifano, 1997
Symptoms of temporomandibular pain- dysfunction disorder include joint crepitus, joint locking, tinnitus, aural congestion, vertigo, hyper- or hypoacusis, blurred vision, hoarseness and orofacial dysaesthesia – Chan et al., 1994
The findings show that cholinergic nerve transmission, most likely from the parasympathetic division of the autonomic nervous system, can influence Eustachian tube function. We hypothesize that this effect is due to changes in surface tension in the Eustachian tube as a result of changes in secretion. – Franz & Anderson, 2002
Patients suffering from Ménière’s disease are particularly sensitive to negative pressure in the middle ear. For example, attacks of vertigo can be triggered by a descent in an aircraft when ventilation of the middle ear can become critical. – Franz & Van Der Laan, 2005
Bruxism
Bruxism, being teeth grinding in the night, is a response to mandibular instability. Lack of vertical height of the teeth, improper tongue posture (especially a completely lowered tongue), as well as TMJ stability will cause the nervous system to try to find stability in occlusion, by clenching the teeth together. This, of course, will just reduce the vertical dental height further over time as they are wearing out, and thus exacerbate the bruxism.
There are some dentists that repair the teeth’s dental height, or make night splints for the teeth. Usually though, establishing TMJ stability through strengthening the pterygoids, getting the tongue up to the roof of the mouth and changing the resting position of the mandible in daily posture will be sufficient measures. If this does not cure the bruxism, a splint or other relevant dental procedure may be necessary.
Tinnitus
As already mentioned, the trigeminal nerve innervates the muscles that control sound modulation in the ear, namely the tensor tympani and tensor veli palatini muscles. Compression of this nerve’s branches will often spread to the ear, which is why there is a high correlation between TMD and tinnitus complaints. Tinnitus may also occur because of buccal nerve compression, in which case it is not necessarily a TMD problem but a lateral pterygoid problem.
Additionally, the pterygoid muscles have fascial connections to the inner ear. Both pulsatile tinnitus and ordinary tinnitus may be treated by strengthening the pterygoid muscles and optimizing mandibular articulation and resting position.
Tinnitus may also be caused by sympathetic plexus irritation. Review my thoracic outlet syndrome and atlas articles for further information.
Fig. 16
Many patients with temporomandibular disorder and coexisting tinnitus find that therapy improves or resolves their tinnitus in conjunction with their TMD symptoms. – Wright & Bifano, 1997
It was observed that tinnitus was significantly associated with age, bruxism, otalgia, loss of posterior teeth, pain in masticatory muscles, TMJ pain, and existence of TMJ sounds (p<0.05). – Beriat at al., 2011
A few cases of tinnitus have been relieved temporarily by novocain block of the auriculotemporal nerve. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus
We surveyed 1032 patients: 338 had TMD and 694 served as two age-matched control groups. Tinnitus and vertigo symptoms were significantly more prevalent in the TMD group than in either of the control groups. – Chole & Parker, 1992
TMD patients with coexisting tinnitus report 46 to 96 percent have tinnitus improvement or resolution from TMD therapy (Table 1).9-15 A survey taken two years after TMD therapy suggests the tinnitus improvement is sustained over time – Wright & Bifano, 1997
Several findings indicating a relatively strong relationship between CMD, tinnitus and subjective hearing loss were noted. This relationship seemed to be independent of objectively assessed degree of hearing loss, occupational noise exposure, general morbidity, medication or socioeconomic status. The prevalence of frequent headaches and fatigue or tenderness in jaw muscles was higher in tinnitus patients than would be expected if these conditions were unrelated. About one third of the individuals affected by tinnitus reported influence on tinnitus by jaw movements or pressure on the temporomandibular joint (TMJ). – Rubinstein, 1993
The study concludes with a recommendation for TMJ referral for those tinnitus patients with unknown etiology who demonstrate any three or more of the TMJ indicators. – Vernon et al., 1992
Correctives
As the Mews mentioned, the solution may be perceived as too simple to be true. Although I don’t follow the exact same protocol that they use as dentists, their principles definitely led me to the solution of this issue as a structural corrective that can be maintained with proper myofascial and postural work.
I’ve touched on it already; maintain proper mandibular resting position by protracting the jaw slightly. You may disregard your occlusion, it is ok that the teeth are not touching, because your dysfunctional occlusion is what’s causing your TMD in the first place. Dentists probably won’t agree with me, but I have a close to 100% success rate treating TMD this way, and strongly believe that this outweighs any benefit that a dysfunctional occlusion may yield (if any). By optimizing tongue posture, and chewing harder foods, the maxilla may develop in a parallel manner and thus lead to a win win situation. Chewing hard foods may not be a great idea, however, if you have a lot of jaw pain. Moreover, for adults, significant growth of the maxilla cannot reasonably be expected.
Here is the protocol:
From maximal mandibular retraction, protract the jaw (2)-4 millimeters, and stay there. Read that twice if you need to, because it’s the foundation of this article and the most important principle of curing TMD. This single postural act will open up the TMJ, completely removing the chronic shear forces between the mandibular condyle and the joint’s disc and socket. You may end up with a slight underbite (rare), but this is still better than eating through a straw and living with chronic facial pain. Most people won’t end up with an underbite though; it’ll just feel a little weird not to maintain occlusion in posture. Once again, the molars can no longer occlude in this position, which is normal and not a problem. The key is to unjam the TMJ by getting the mandible forward.
The lips should be sealed, and you should breathe through the nose. This will keep the front teeth in check, hindering them from protruding. In fact, it’ll keep them in line. Of course, you must maintain your normal occlusion when eating, to crush the food with your molars. That’s fine, it won’t cause any injury as long as the TMJ is centrated at all other times. The body can cope with this minor joint shearing, as long as it ceases at the remainding hours of the day.
Pain levels will usually reduce quite quickly after optimizing joint resting position, unless there is severe bruxism at play. In such case, as mentioned, a night splint may be necessary.
Fig. 17

Additionally, it’s important to optimize mandibular movement by teaching it to protract properly during opening, and gradually (not maximally) retracting during closing. It’s difficult to learn both a new mandibular resting position and way of opening, but definitely doable with some practice and motivation.
Honestly, proper opening and closing of the mouth is something anyone can benefit from, TMD or not, as the pterygoids which promote proper mandibular kinematics also attach to the sphenoid bone. I’ve written more extensively about this in my atlas article, but my theory is that it controls posture due to its relations to the optic chiasm and nerve tracts. This is probably why so many studies show correlation between occlusion and posture; due to its relation and altered pull on this very special cranial bone.
Teeth clenching during stress, mouth breathing, etc, must also cease. Jaw clenching often reduce or cease on its own when proper resting position is assumed, as it’s not possible to protract the mandible and clench the molars simultaneously. Mouth breathing however, may be more difficult to stop with if the airways have been restricted as shown in the initial video in this article. If this is your or your patient’s problem, I recommend looking into the “Buteyko breathing method”, which addresses this issue.
Strengthening the pterygoids
Strengthening the lateral and medial pterygoids will often be necessary to promote proper joint kinematics (jaw movement), resting position, and also to free the buccal nerve from potential entrapment. An indication of weakness can be buccal nerve pain, tinnitus, or difficulty maintaining the new mandibular resting position.
A small number of sufferers may struggle to protract the jaw without clenching the suprahyoid musculature. This is a strong dysfunction, and indicates extreme weakness of the pterygoids. In such case, very light protractions without any resistance must take place, while simultaneously palpating the suprahyoid musculature and ensuring that it is not activating during protraction. To resolve TMD, it is CRITICAL to learn how to protract the jaw without tensing the supra hyoid muscles. Read this several times, if needed! It is vital.
Here are the exercises. Again, make sure that you’re not clenching the suprahyoid, which is a common cheat when the pterygoids are forced to work harder than their capacity allows.
- The lateral pterygoid can be strengthened by opening the jaw forward and downward while resisting with your palm. Make sure to also control the eccentric phase (reversal).
- The medial pterygoid can be strengthened by closing the jaw forward, form an open base position. Once again, use your palm as resistance and make sure to control the eccentric phase.
Beware that many patients have pterygoids that are extremely weak, and these patients will worsen with jaw protraction if it is done excessively. They will also worsen with proper tongue posture, as proper tongue posture pushes the jaw back, and this is resisted by the pterygoids. This increases their workload and results in premature exhaustion for certain vulnerable patients. In my experience, about half or slightly less of patients that suffer from TMD have severe pterygoidal weakness.
If you develop pterygoid pain with jaw protraction, and this will mainly pertain to patients with stronger TMD morbidity, it is important that you wait with optimizing tongue posture until they are stronger. Moreover, some patients may need to gradually introduce the jaw protraction over the course of several months, gradually increasing the pterygoidal strength and work capacity. Some patients may tolerate as little as one hour daily in the beginning, but many cna tolerate more. About half my TMD patients can tolerate holding their jaw forward all day long without developing significant problems with the pterygoids, as long as they are careful not to simultaneously overtrain them with exercises.
Cervical instability
Clenching of the hyoid muscles may also be a compensatory strategy which is secondary to cervical instability. Poor cervical postures, muscle weakness or injury (especially of the longus capitis & colli muscles), etc., may cause the patient to clench his throat (hyoidal muscles) as they have similar functions as that of the deep neck flexors. Clenching them will somewhat increase cervical stability. However, it will also pull the hyoid bone caudally (down) as well as the mandible back, and is thus an important factor to evaluate in neck and jaw patients. If the patient is clenching their throat in order to stabilize their necks, it is important to re-incorporate the impaired muscles’ function (often the deep neck flexors) and simultaneously work on ceasing his or her throat clenching. Read my atlas article for more information on this topic.
Summary
Temporomandibular dysfunction or TMD occurs when the mandibular condyle (head) is continuously resting or being pushed too far back into the joint socket. Over time, this may injure the articulate disc and cause its displacement, lead to joint degeneration, trigeminal neuralgia, postural anomalies and so on.
The main cause of the posterior position of the mandibular condyle, is an underdeveloped maxilla bone (upper jaw). This causes occlusion to establish too far back, ultimately jamming up the joint due to length differentials between the mandible and maxilla bones (as the mandible keeps growing to its full potential, no matter if the maxilla’s growth is inhibited). Proper tongue posture, nasal breathing and lip sealing may encourage the once inhibited maxillary horizontal growth process to reinitiate, even in adulthood.
Swayback posture leads to forward head posture, which causes the mandible to pull backward due to its sternal attachment through the hyoid musculature. Thoracopelvic and craniocervical posture is therefore a relatively important aspect in the treatment of TMD.
Maxillary underdevelopment or not, TMD may be relieved by these simple points, in the utmost majority of cases:
- Close your mouth with your lips, and breathe with your nose
- Posturally protract your mandible 2-4 millimeters from maximal retraction (most important). Sometimes more than 4 mm will be required.
- Learn proper jaw opening and closing (2nd most important)
- Optimize thoracopelvic and craniocervical posture
- Avoid habitual jaw clenching during stress, exercise, and so on
- Optimise your tongue posture and swallowing technique (proper tongue posture can overload the pterygoids in the beginning)
The information about TMD is excellent.
I have severe mandibular dysfunction. The mandibular is shifted left because of the excessive therapy done by a dentist. Can it be corrected without surgery?
Thanks,
Irene
Just 1 question sir am i suppose to maintain that position while talking and laughing , my ja really hurts while laughing.
Besides U are doing a great work may god bless u
Forward at all times except when eating.
Can this article help jaw clenching and tmj that was set off by antidepressant bruxism side effects? What is in these drugs which causes your jaw to clench ? Is it not the brain which is telling the jaw to clench so isn’t the brain the problem not the jaw? Thank you
Unless you’re dystonic, which I doubt, then your claim here is very unlikely.
In many internet articles about displacements i see disk is displaced forward when jaw closed and pops when jaw opens/protracts forward. But is it possible for disk to be displacet backwards? Like how i drawed in picture. Why i ask? Because when i push my jaw a little forward i hear a pop.
Does it mean that my jaw only gets into the normal disk position when I pull jaw forward? I can hold my jaw in that forward position all the time. But what IF my disk displaced backwards, as I have drawn in pic, then I will make myself worse if i keep this position.
TLDR: When i protract i hear a pop, but i don’t know if after the pop my jaw aligns with disc or vice versa – misaligns. So should i keep my jaw protracted?
Pic: https://i.imgur.com/azDat0r.png
From what I can tell the advice here only applies to people who cannot *open* their jaw or have trouble doing so. I have not seen anything applicable to the situation where you cannot *close* your jaw.
Cannot open; disc stuck infront of the condyle. Cannot close; disc stuck behind the condyle. The base mechanism is still the same. For those who cannot close, the superior head of the lateral pterygoid might require extra attention as it can help in pulling it forward, but remember that the real problem is disc tissue damage which is caused by an overly retracted condyle.
I don’t mean to come off as rude but isn’t it the other way around Kjetil? Using a image (fig. 12) as reference wouldn’t the disc being stuck in front of the condyle prevent closing? As the tissue holding the disc would create a barrier of sorts, blocking the condyle from re-entering the fossa?
Skiva blokkerer åpning når den ligger for langt frem, spesielt når den er fortykket, og hindrer lukking når den lukserer bak (posteriørt) for kondylen.
I have severe TMJ and I have been following the advice of protruding my jaw. My orthodontist told me that my chin is too far back — is there a corrective surgery that could bring my jaw forward to correct both of the issues simultaneously? In addition, my radius bone on one side is thinning & no specialist has been able to tell me why. Could it also be TMJ related? I’m in so much pain I can’t sleep at night & I was just told to take ibuprofen every night. Regardless, this article was helpful. Thank you so much.
The information about TMD is excellent.
I have severe mandibular dysfunction. The mandibular is shifted left because of the excessive therapy done by a dentist. Can it be corrected without surgery?
Thanks,
Irene
I don’t know, I need to examine you. Probably, if it was induced by dental treatment.
Hello,
I’m an 18 year old male and have had facial assymetry since I was about 13-14. I thought I was a normal thing until recently when a few thing started adding up – popping and cracking in my left side jaw, my left jaw and face being more defined and overworked due to chewing on them, which leads to my head slightly tilting to the right side which is weaker, accenting the caused assymetry – lower right eye, uneven mouth.
Since I’ve had this for a while but only recently discovered that It could be TMJ and jaw related, would my course of action be to follow the steps and hope for the best or have my bones grown like that and It’s too late to reverse. I don’t have a lot of pain, but my left jaw pops with every time I chew and I believe my left masseder muscle is overworked. Is it too late to fix this? I’d appreciate your reply greatly.
Just do some Mewing and hope for the best. If you have no pain then don’t overthink this. No one have a perfectly balanced face.
As well, Massage all the muscles around your cranium, face, neck, chest, upper back and shoulder, and practice range of motion exercises, to help reduce tension.
I had an underbite as a child. Botched ortho, plus a broken femur (that had me in traction for 2 months at 10, which twisted my hips, spine and shoulders into scoliosis)turned that into a crossbite, as well as the all the symptoms you mentioned. This article was like reading a case study on myself(thank you mskneurology, you’re the best info I’ve found on this!).
I’m 39 now and am almost fully recovered from severe symptoms, after about 1.5 years of corrective strengthening. But I was also fixing severe imbalances in my whole body, from many years of compensation while living an extremely active(further damaging) lifestyle. So I’d say you can definitely still reverse this.
I’ve even managed to straighten my teeth without orthodontics or aligners of any sort.
Good job
You’re saying the skull can change shape from muscle use even after becoming an adult?
Hi,
I was wondering if an open bite can disappear without surgery ?
What is the process ? (Does jawbone change its posture ? )
Do palate enlarge due to constant firm pressure and a good tongue posture, and then reduce the gap between upper and low teeth ?
Regards,
Peter
Doubt it
What if my jaw goes zig zag when I open and close it?
Hi,
I was wondering if an open bite can disappear without surgery ?
What is the process ? (Does jawbone change its posture ? )
Do palate enlarge due to constant firm pressure and a good tongue posture, and then reduce the gap between upper and low teeth ?
Regards,
Peter
If I follow all of the steps above “religiously” how long will it take before I start to see some improvements? Btw my tmd problem is relatively small. Thanks.
Depends if you do it right or not, but I’d say within 4 weeks. Probably earlier.
I believe I need surgery desperately, my pain in the left side of my jaw is excruciating. I live in Columbus Ohio is there anyone you could recommend for me to see?
Surgery is usually unsuccessful for TMD management, especially with regards to long term results. It can still be helpful to fix large injuries, eg. complete rupture of the retrodiscal ligament — thus evaluated on a case to case basis. I suggest that you book a skype session or get a splint that advances the mandible.
Hello Dr. Larson,
Your article is amazing and as many have stated, I have seen many doctors with no improvement. Long story short, I get daily tension like headaches and never had jaw pain so it took a very long time to finally validate my TMD, which I helped identify through due diligence and long time dentist. I just started applying your protraction recommendation and was wondering if I could schedule a Skype session, as you suggested to the above person, to validate my symptoms and obtain any other solutions or approach.
Thank you in advance for your support!
Happy to assist
Thankyou for your sharings! Do you offer Skype appointments? Where are you located?
If I follow all of the steps above “religiously” how long will it take before I start to see some improvements? Btw my tmd problem is relatively small. Thanks.
OMG thank you, thank you, thank you!!! It has been two years since I’ve been afflicted with TMJ issues. I’ve seen my doctor, dentist, an oral surgeon, a TMJ specialist, a physical therapist, an acupuncturist, and a chiropractor. My next stop, before finding your post, was to have Botox into the masseter. In just two days of following your jaw protraction exercise I am virtually back to myself. I literally felt the discs slip back into their place!!!! FANTASTIC!!!
OMG thank you, thank you, thank you!!! It has been two years since I’ve been afflicted with TMJ issues. I’ve seen my doctor, dentist, an oral surgeon, a TMJ specialist, a physical therapist, an acupuncturist, and a chiropractor. My next stop, before finding your post, was to have Botox into the masseter. In just two days of following your jaw protraction exercise I am virtually back to myself. I literally felt the discs slip back into their place!!!! FANTASTIC!!!
Can you tell me the exercise? I don’t know I have TMJ with reduction or without reduction. But one day i was eating, I heard poping sound and I immediately search on internet but next day i did heard poping sound rather jaw was paining and i couldn’t chew.
Another great article.
Is it best to stop wearing my orthodontic retainer (Essix retainer) in order to follow this method?
why do so many people think that retraction and opening super wide is the answer to TMJ they sell things claiming to cure tmj that open your mouth retracting it. I used these and it made it 10x worse. I just realized that after 20 mins doing protraction my pain is less intense. Thanks for the article
Another great article.
Is it best to stop wearing my orthodontic retainer (Essix retainer) in order to follow this method?
Depends on how it’s built. I can’t comment on it without seeing you.
Excellent article! After much pain and trouble swallowing for years, I have finally been told I have a problem with my right TMJ caused by the loss of the rear three molars from bottom jaw. I have advanced periodontal disease and the teeth have been removed sequentially over a 5 year period as bone density decreases and pockets of bone infection formed under the teeth. The dentist has said I need a splint. I’m really hoping it will help because the pain is excruciating and I have suffered for such a long time now.
Postural protaction exercise…how long do you hold the position? Is it worth doing in my case?
Kind regards
Excellent article! After much pain and trouble swallowing for years, I have finally been told I have a problem with my right TMJ caused by the loss of the rear three molars from bottom jaw. I have advanced periodontal disease and the teeth have been removed sequentially over a 5 year period as bone density decreases and pockets of bone infection formed under the teeth. The dentist has said I need a splint. I’m really hoping it will help because the pain is excruciating and I have suffered for such a long time now.
Postural protaction exercise…how long do you hold the position? Is it worth doing in my case?
Kind regards
I was on the verge of dedicating my life to yoga and exercise — so much pain from TMD and TOS! I knew I had both, but did not know that it was causing all my other symptoms. I was about to start a blog and track what I did know. I knew right before an episode, I would get hiccups that hurt. I haven’t slept well in years. My body has been in fight/flight mode forever it seems.
I just had another bad episode, from doing a little gardening, not much at all.. very little exercise for the amount of pain I had in my jaw. It was relentless pain, most of my teeth on one side felt like they were being pushed out. I cried it hurts so bad… then I started doing the protraction, and the pain went down.. and its still going down. I’m reading more and doing more of what you said. I’m yawning like crazy, I haven’t yawned in years!
THANK YOU! I LOVE YOU!
I was on the verge of dedicating my life to yoga and exercise — so much pain from TMD and TOS! I knew I had both, but did not know that it was causing all my other symptoms. I was about to start a blog and track what I did know. I knew right before an episode, I would get hiccups that hurt. I haven’t slept well in years. My body has been in fight/flight mode forever it seems.
I just had another bad episode, from doing a little gardening, not much at all.. very little exercise for the amount of pain I had in my jaw. It was relentless pain, most of my teeth on one side felt like they were being pushed out. I cried it hurts so bad… then I started doing the protraction, and the pain went down.. and its still going down. I’m reading more and doing more of what you said. I’m yawning like crazy, I haven’t yawned in years!
THANK YOU! I LOVE YOU!
Hello mister Kjetil,
I have a posterior TMJ dislocation that is very rare, so my jaw is already posterior, my bottom teeth are in front of the top ones. What kind of exercises or relief would you recommend for me. Same position 2 4 mm or something else. Thank you very much in advance
Hello,
I have developed pain in the area between jaw and ear when I open mouth wide a d clench teeth. The pain when teeth are clenched radiate to my ear and down the side of my neck behind ear. Will these exercises cure this pain?
Hi, it sounds like TMD. That’s all I can say without assessing your case.
Hello mister Kjetil,
I have a posterior TMJ dislocation that is very rare, so my jaw is already posterior, my bottom teeth are in front of the top ones. What kind of exercises or relief would you recommend for me. Same position 2 4 mm or something else. Thank you very much in advance
Same approach. Posterior dislocation of the disc is easier to treat, perhaps, because the lateral ptergyoid will pull the disc forward.
I m a oral surgeon , i think thath your concepts
about disfunction of tmj are wright and is a big revolution
Thank you, Dr. Enrico!
I m a oral surgeon , i think thath your concepts
about disfunction of tmj are wright and is a big revolution
My left jaw really hurt when I tried opening my mouth, and my dentist told me to stop clenching my teeth when I close my mouth. He told me to relax the lower jaw and push it back (my jaw juts forward a bit already) when my mouth is in resting position. But your article is telling me to protract the jaw, right?
Hi I have a question regarding some info in this article. I was diagnosed with bruxism and was told by my dentist that the ONLY option was to wear a discharge splint. When fitting it in, I was told that they were going to need to retract my mandible and that by wearing the splint over a long period of time I would retract the mandible permanently to prevent the effects of bruxism. This set off red flags after having read your article considering what you said about retracting your mandible.
In fact, I can´t retract my mandibule naturally as you said it would be most optimal to, and when fitting the splint, my dentist had to move my mandibule for several minutes just to fit the splint, which shows that in fact I shouldn´t be retracting my mandibule and in fact should be doing the opposite, assuming I understood your article correctly.
As you might surmise, I am very concerned over the conflicting information and would really appreciate a second opinion and some pointers on what the best course of action would be as my dentist doesn´t even allow me to ponder any other possibilities. I would also like I had braces to fix an overbite but I am not sure what effect it had on my general face structure as I don´t have any pre-braces photos. Yet, I add this extra detail in cause it might be of revelance to the topic.
My left jaw really hurt when I tried opening my mouth, and my dentist told me to stop clenching my teeth when I close my mouth. He told me to relax the lower jaw and push it back (my jaw juts forward a bit already) when my mouth is in resting position. But your article is telling me to protract the jaw, right?
IMO: Detrimental advice you have been given. It will make you MUCH worse. Pulling the mandible back will greatly increase compression within the TMJ.
I have the same problem with my left lower jaw. Nobody here recognizes this disorder ive been suffering from. The doctor gives me nuberol forte and tells me not to take stress and as an effect my jaw will be fine. This is the only cure he could give me. I mean I have a prominently abnormal left lower jaw and it is so much bigger than my right lower jaw. It has a drastic asymmetrical affect on my face. Iam in a misery. My left lower jaw is always jammed, in pain, uneasy, and ugly. Please tell me what shall I do
The article is free, read it.
I have the same problem with my left lower jaw. Nobody here recognizes this disorder ive been suffering from. The doctor gives me nuberol forte and tells me not to take stress and as an effect my jaw will be fine. This is the only cure he could give me. I mean I have a prominently abnormal left lower jaw and it is so much bigger than my right lower jaw. It has a drastic asymmetrical affect on my face. Iam in a misery. My left lower jaw is always jammed, in pain, uneasy, and ugly. Please tell me what shall I do
This article is an exceptional resource for those seeking to learn more about TMD. I’d be very appreciative if you could provide references for the citations. I’m writing my own medical appeal to get care for TMD and I’d really like to include some of the materials you cited.
This article is an exceptional resource for those seeking to learn more about TMD. I’d be very appreciative if you could provide references for the citations. I’m writing my own medical appeal to get care for TMD and I’d really like to include some of the materials you cited.
Just google the quotes, you’ll find the papers.
Hello, I’m 35 years old, female and have had bruxism very bad for about 5 years. It started when i took zopiclone for a short time. I have broken several teeth and about 8 are totally ruined and need to be extracted. I eat only soft foods due to an eating disorder but it had no effect on my jaw for ten years. My right jaw clicks and makes a creaking noise if i open it too wide and i feel there is less space between the teeth on the right side when i put my tongue between them. Is there anything i can do once they are out to protect my remaining teeth from breaking? I had a mouth guard i wore at night but i still broke my teeth with it in. Please help, thank you.
Hello, I’m 35 years old, female and have had bruxism very bad for about 5 years. It started when i took zopiclone for a short time. I have broken several teeth and about 8 are totally ruined and need to be extracted. I eat only soft foods due to an eating disorder but it had no effect on my jaw for ten years. My right jaw clicks and makes a creaking noise if i open it too wide and i feel there is less space between the teeth on the right side when i put my tongue between them. Is there anything i can do once they are out to protect my remaining teeth from breaking? I had a mouth guard i wore at night but i still broke my teeth with it in. Please help, thank you.
After countless doctor, dentist, and physiotherapist sessions in the past 6 years I’ve had this I just want to say thank you. I’ve tried everything on this article in the past week and I can already see and feel the differences in my jaw, it’s so much better than any advice I would get from specialists and I just wish I found this sooner.
I’ve also found that when I get clogged, echoing hearing when I talk in my one side, I just hold the lower mandible forward at it’s base behind my neck when I talk and it goes away within seconds. Although, I’m not sure how or why that works?
Beautiful job, well done.
After countless doctor, dentist, and physiotherapist sessions in the past 6 years I’ve had this I just want to say thank you. I’ve tried everything on this article in the past week and I can already see and feel the differences in my jaw, it’s so much better than any advice I would get from specialists and I just wish I found this sooner.
I’ve also found that when I get clogged, echoing hearing when I talk in my one side, I just hold the lower mandible forward at it’s base behind my neck when I talk and it goes away within seconds. Although, I’m not sure how or why that works?
Hi, I am 18 years old and I was a mouth breather pretty much my whole life. Recently I got my braces done, which did help me with my overbite and overcrowding issues, and I also started mewing. However, I was noticing jaw pains (TMD), which i think is the exact problem as shown in the first video of the article. I manually protract my jaw forward during the day, but when I sleep, I feel like my jaw would slide back downwards and rest in the posterior position of the joint socket. Is there any way to prevent this? Would a chin strap work? Any tips would be amazing thank you.
Use a splint at night if you wake up with pain. If you wake up feeling better, no need for a splint. Naturally, you can’t control your noctural habits.
Hello. Thank you. I’ve been diagnosed with severe degenerative OA of TMJ. Will these exercises still potentially help with such a condition? Also should it hurt and/or cause soreness initially when doing the protraction exercises?
Help, yes. Cure, not sure. But it’s your best bet regardless as far as I am concerned.
Hi, I am 18 years old and I was a mouth breather pretty much my whole life. Recently I got my braces done, which did help me with my overbite and overcrowding issues, and I also started mewing. However, I was noticing jaw pains (TMD), which i think is the exact problem as shown in the first video of the article. I manually protract my jaw forward during the day, but when I sleep, I feel like my jaw would slide back downwards and rest in the posterior position of the joint socket. Is there any way to prevent this? Would a chin strap work? Any tips would be amazing thank you.
Wow, most comprehensive article I have read so far! Lately I had tooth fillings, I would dislocate my left jaw after prolonged mouth opening, and my dentist had to reduce it back. No pain and no problem at home after the procedure. But everytime I go to the dentist for fillings, dislocation happens especially when I’m required to open my mouth wider. This never happened to me before. Can I apply the protocol to my case? Also, I realized that I’ve been chewing food at the right side for how many years already. Does the left jaw dislocation have something to do with my right sided chewing? I’m now trying to be cautious with proper mouth opening, and chewing food at both sides.
Learn to open your mouth properly, as per the video in this article.
Wow, most comprehensive article I have read so far! Lately I had tooth fillings, I would dislocate my left jaw after prolonged mouth opening, and my dentist had to reduce it back. No pain and no problem at home after the procedure. But everytime I go to the dentist for fillings, dislocation happens especially when I’m required to open my mouth wider. This never happened to me before. Can I apply the protocol to my case? Also, I realized that I’ve been chewing food at the right side for how many years already. Does the left jaw dislocation have something to do with my right sided chewing? I’m now trying to be cautious with proper mouth opening, and chewing food at both sides.
Use a splint at night if you wake up with pain. If you wake up feeling better, no need for a splint. Naturally, you can’t control your noctural habits.
Hi, I managed to dislocate the jaw joint on my right side unfortunately from chewing gum. Opening the mouth feels different than before, and I occasionally get pain when chewing on my right side. I was wondering if the tips still apply in this case, and is there anything I need to be especially conscious of? is it possible to undo the dislocation somehow, or is it something I just need to learn to live with?
Get an MRI
How long do I have to do these exercises?
The postural change is permanent, not an exercise. The exercises as such, can be done twice per week until healed, then once every 10 days or so for the rest of your life.
Amazed you get results with the pterygoid exercises when doing them just twice a week. Is rest and recovery the reason you don’t do them more often?
I just started doing both of them: 6 reps … massage … another 6 reps. Just started but I was going to do them everyday. I guess too much?
Big Thanks !!!!
Reps & sets:
https://youtu.be/HezNZkdt4Ug
Hi, I managed to dislocate the jaw joint on my right side unfortunately from chewing gum. Opening the mouth feels different than before, and I occasionally get pain when chewing on my right side. I was wondering if the tips still apply in this case, and is there anything I need to be especially conscious of? is it possible to undo the dislocation somehow, or is it something I just need to learn to live with?
Hi, excellent article. I don’t exhibit many of the symtoms of TDM you listed except for occasional clicking and popping in my jaw. However I do have an asymmetrical/uneven jaw with it tilting to one side which I didn’t have when I was younger and I believe is due to TDM. Do you think this is a reasonable belief and if so would it also be corrected by the methods you outlined? Thanks for any help.
Hi, excellent article. I don’t exhibit many of the symtoms of TDM you listed except for occasional clicking and popping in my jaw. However I do have an asymmetrical/uneven jaw with it tilting to one side which I didn’t have when I was younger and I believe is due to TDM. Do you think this is a reasonable belief and if so would it also be corrected by the methods you outlined? Thanks for any help.
Ive suffered at time severe TMD for over 20yrs, I always thought my bite was wrong, ive seen several specialist with no step forward, last week I finally had Botox injected into my masetter muscles and this has caused a shift forward in my mandible, a lot of my clicking has now gone and pain is subsiding. Now I can freely move my mandible your tongue rest position and mendible rest position has made me realise I have had quite a severely retracted mandible for a lomg,long time. When it shifted forwards after the Botox Ithough this new position was very wrong now i realise its actually sitting where it should.
Thank you
Botox usually just makes it worse, but I am happy that you got a good result.
Hello,
Could you please explain how botox in the masseter muscle causes jaw retraction and worsening of TMD. That is exactly what happened to me and I would like to know why.
Thank you
The masseter is a protractor and the main muscle of chewing. When inhibited by botox, you’re left with the temporalis muscle. The temporalis pulls the jaw back and thus worsens TMD.
Thank you for your response. Is it accurate to say that only the superficial part of the masseter is involved in protraction of the mandible and that the deep part is actually involved in the retraction of the mandible? Does that mean that botox to the masseter is usually done into the superficial part of the masseter?
Also, would botox into the fibers of the temporalis help protrude the mandible? And finally, would release of trigger points in the Lateral Pterygoid help protrude the mandible?
Thank you
Botox of the temporalis muscles is ok, sometimes even a good idea. I don’t recommend masseter botox, and I certainly strongly discourage botox injections of the pterygoids. Releasing tension from the pterygoid is strongly discouraged, as they are protractors, but also, because they are often very weak and vulnerable, and a common cause of TMD-related pain. Massaging weak muscles makes the problem worse.
Ive suffered at time severe TMD for over 20yrs, I always thought my bite was wrong, ive seen several specialist with no step forward, last week I finally had Botox injected into my masetter muscles and this has caused a shift forward in my mandible, a lot of my clicking has now gone and pain is subsiding. Now I can freely move my mandible your tongue rest position and mendible rest position has made me realise I have had quite a severely retracted mandible for a lomg,long time. When it shifted forwards after the Botox Ithough this new position was very wrong now i realise its actually sitting where it should.
Thank you
Dear Mr Larsen, just wanted to say THANK YOU, I can’t tell you the difference this article has made to the level of pain I have been in for a long time, and in turn my ability to function. I am also able to catch myself clenching my jaw muscles when I get stressed, and instead slide the jaw forward deliberately which gives immediate relief/a kind of stretch and prevents the severe locking/pain that would usually come in a couple of hours. You are a brilliant man, I wish you all the luck in the world, thank you for taking the time to share this, it is the only thing that has helped me properly. Kind regards, Lauren Wilson
Very happy to hear this. Good job on implementing the material.
Hello! I came across a very well written article that you wrote in regards to TMJ in detail. I was very impressed. I have been suffering from TMJ since I was 12 years old, but it only has been a month since it has gone out of hand. I started developing horrible symptoms all of the sudden all at once. Can you direct me to the appropriate person or procedure to fix this? Or any suggestions at all? I would be very grateful for any advise. I would appreciate it very much. As at this point, it is affecting every aspect of my life.
Consider booking a session.
hello Would like to b einformed on your tariffs with skype sessions for jaw clenching and bruxism
The prices are seen on the booking page
Dear Mr. Larsen,
I found your article about tmj two days ago and started practicing the protrusion right away. I`ve been suffering from tmj for 9 years and tried physiotherapy, different splints, Feldenkrais, but nothing helped.
However, what you say, i.e. the protraction, yielded immediate results. I can*t believe it. Is the solution really that simple? Thank you very much.
Simple, but not easy. Many complain that they aren’t able to hold their jaws forward. As you can see, by your own example, it’s just a matter of motivation. Well done on helping yourself.
Greetings from Canada
I am trying to follow your protocols. I have had TMJD for many years. I have tinnitus mainly in the left ear with many sounds which drives me nuts and causes intense anxiety. A psychiatrist tried me on 6 anti depressants which almost ended me. I am by the grace of God off the meds. I have headaches all the time. A ENT tells me I need hearing aids from many hearing tests over the years. I had a left jaw joint scope surgery 2 years ago. The right joint is painful and I think the disk moves as I have the popping when I open my mouth. That surgeon also told me to do the jaw opening exercised by stretching my jaw many times a day (you say this is detrimental). My hearing fluctuates and my left ear feels fullness or pressure. I have also seen 2 chiropractors who thought my spine and posture were good. Last year a dentist made a night splint to wear on my upper teeth. I had a recent head MRI but nothing shows.
At 54 years of age I am desperate to get my life back from all the problems I have been suffering with. I have lost my job as substitute teacher and have no income or benefits at this time because of the anxiety and depression. These struggles have been very trying for my wife and daughter.
From your detailed writing do I understand correctly I should not stretch my mouth open by force with my hands? And I should continue to hold my jaw forward and hold it there even though I find my cheek muscle getting sore and my molars are pressing on each other?
Thank you for sharing your work and reading my comments. Any help and suggestions are much appreciated.
Sincerely Adrian
Don’t have time to read through long text, very sorry. Consider booking a session.
Great article. I find when I protract my mandible I can hear a bit of a pop, is this an indication that the mandible is sufficiently protracted enough and I should hold it there? I’ve been doing this the last few days but it gets very tiring holding this position after 4-5 hours, hopefully it gets easier to do.
It’ll get easier. The pop is just relocation of the disc due to preexisting subluxation; ignore it.
Since protracting the mandible my TMD is better but it feels like there’s a blocking sensation with my epiglottis/hyroid area when I want to sleep and turn to the side. It takes hours to get to sleep. I dont really get how to train what you describe here
“Proper position is just open enough to maintain steady and full airflow. Initiate swallowing and try to breathe; it won’t work as the epiglottis is blocking the trachea. Now reverse the swallowing by a few millimeters; breathing should be possible but restricted. Reverse it some more; breathing should now be fully possible without restrictions, but the hyoid has still not dropped down or forward. Learn to breathe, and talk without allowing the epiglottis to drop down and forward
Do you have a video on that? Thanks!
This is likely not TMJ related. Perhaps upper cervical.
I have had tmd for about 4 months. In December, I took a bite out of a large sandwich and somehow hurt my jaw. I noticed that I have a slight underbite whick I will try to fix with this new position. I’m hopeful that it works. This injury has caused me a lot of anxiety and I just want it to go away!
Dear Mr. Larser,
I have Juvenile revmatoid arthritis and I am 23 years old. Before 6 years i had pain in my jaw, in the left side and the doctor told me that it was because of the arthritis. I have visited many doctors and I see that nobody can help me. I don’t like my face in one side because of that. It looks asymmetrical. Now I don’t feel any pain, but I want it to be more symmetrical and I don’t think that I must do surgery, as many doctors told me. I will do all of this in this article and I hope it will help me to look more beautiful. Please, please tell me your opinion. Thank you!
Dear Mr. Larson,
when opening the jaw, should we practice opening it WITHOUT the clicking and shifting? Or should we just focus on opening it correctly, no matter how much it shifts and clicks?
Also, after doing this, I can feel my mandible going forwards making me unable (!) to make my molars touch. After sleeping or not focusing on the posture, I revert back or wake up with my molars touching and my jaw hurting.
Thanks
You’ll push through it, presuming no excessive symptoms. Don’t try to build Rome in one day.
Obviously the molars won’t touch if your jaw is forward. this is fine. But you gotta chew as you would normally.
Thanks for this great article. Just a question: without a jaw expansion device and orthodontics to move/grow the premaxilla forward/move the upper teeth forward, what is the long-term way to keep the mandible forward? Wouldn’t the mandible fall back at night and wouldn’t the new position become untenable due to the occlusion during eating forcing the mandible backwards? Is the idea that eventually you don’t have to hold the mandible forward and it just rests there without effort? Also, you only made a passing comment about an underbite, but it seems to be that for many people protracting the mandible would make them feel self-conscious/produce a concave facial appearance.
Thank you for this article, Dr. Larsen. I’ve been working with a TMJ specializing dentist who gave me a night splint and exercises, but after a year I didn’t notice any improvement. I found your article and this past week I’ve been following the instructions. I can already feel the changes whenever I retract my jaw; there’s a cushioning sensation, and the clicks I’m used to feel softer and don’t pop loudly anymore!
One question: my right condyle is more damaged than my left, and I’ve been experiencing some occasional stinging pain from it usually while yawning, downward pressure from flossing, and after eating. It’s the same pain I’ve felt when I have to keep my jaw fully protracted and open during dental cleanings. Is it potentially healing/growing pains from my right condyle?
Thank you!
Thank you for this great article Dr. Larsen.
I’m trying to follow all your instructions, but I find it impossible to hold proper tongue posture while protracting the mandible because my tongue shifts forward with the mandible forcing me to rest the tip on my front teeth (I know this is wrong in the long term), and the posterior part on the hard palate. Am I doing something wrong?
Thank you again 🙂
See my response to “Milly”
Dear Dr. Larson,
Thank you for writing this article. I fell from about 10 feet onto my butt 6 months ago and when I landed my teeth slammed together. Since then I have had some face and jaw pain and one of my cheek muscles twitches a little when I smile partway. Two neurologists have said I likely irritated or damaged a nerve, but nothing abnormal showed up on my MRI of my head. The physical therapist thinks it is TMD related and that I will be able to improve this problem by working on my posture, not clenching, etc. I read your article with interest and I am trying to implement the techniques described. I am only able to open my mouth about an inch and a half wide, and I’m not sure if I’m using the correct opening method. Would it be best to just avoid opening wide at all until the posture problems and jaw positioning are doing better? Do you think it would be a good idea to also seek out a dental splint? Do you think that making these changes are likely to help in a few months in a case like mine?
Thank you very much for the article and for your help!
These questions are too case-specific. Consider booking a session.
Can I get treated in the US? Particularly St Louis, missouri
I was excited to find this article. I’m 33 years old and have been suffering tmd for almost 20 years. It all started with just clicking in the tmj. However 5 years ago I started to get pain and the flare ups have now become more and more frequent.
I have a question after reading your article. When I maintain proper tongue position by pressing it against the roof with the tip behind front teeth, I feel my suprahyoid muscles are clenched. And in the article you mentioned that we need to have the mandible protracted and tongue up without clenching the suprahyoid Muscles. How should I accomplish this?
I really appreciated if you could please help.
In some incidences, I let my TMD patients keep their tongues down until their pterygoids are stronger. Tongue posture can stress the TMJ more than helping it, if the stabilizing muscles are very weak. Suprahyoids; they may tense ever so slightly but they’ll elevate rather than depress. If they depress, you’re doing it wrong, likely pushing the tongue too hard up. Just leave it down while strengthening the pterygoids, and then try again later when you’re stronger.
Mr Larson,
First of all, thank you for this article, it is very complete and well written. However, I ask myself a question: I have a lot of tension in the masseters, will this tension decrease over time or will it remain even after permanent correction of the opening of the mouth and the mandible rest position ?
It will go away.
have you successfully treated any patients with dystonia since writing the article ? i developed dystonia after using a bulky, over-the-counter night guard for 2 weeks.
Yes
Hi Mr. Larsen. I follow your protocol and have good results in pain levels in jaw and ear. But one problem stays, when jaw is protract head of mandible go out laterally.
The question is too specific, I need to examine you. Most likely, either your disc is jamming the opening, or the pterygoids aren’t working properly
thanks for the reply. I will make an appointment for a Skype consultation.
Dr Larsen,
What is your opinion on AGGA (fixed appliance) treatment for underdeveloped maxilla? I’ve been going through the treatment about 3 months now. I can breathe through my nose better and my mandible is coming forward. I’m not cured yet, but my TMJ symptoms have improved. However every time the appliance is tightened I become nauseous and dizzy for a few weeks before it feels much better.
Thanks for your time
Jack
I believe that such devices may be helpful for kids under development but futile for adults with regards to facial development. Whether or not it’ll relieve TMD symptoms, depends on whether or not it encourages rostocaudal (forward and down) migration of the condyles.
Hello Sir,
Sir i feel pop while closing the jaw when i put my pinky finger in my left ear and press the area where the left side condyle rests when closed. Is this disc issue.I am having this problem right after my left side wisdom tooth removal. I have also got sensitivity to sounds after this. Please do reply please.
Definitely TMD, sounds like you’re developing some secondary hyperacusis. You’d do well to follow the advice given in this article.
My jaw shifts back to its old state at night. How do fix this?
I practice all day and the next day everything’s tense and my bite is back to “normal”.
Also how do you adress eating with a protracted mandible?
Excuse me, I have had this problem for 7 months due to excessive grinding and improper chewing, I already had my jaw developed before my problem, so I went to a chiropractor and the truth is that it helped me a lot with my problems. I have a month that I do what you mention on this page my question is how long does the pseudisk form and how long will I be able to chew things a little harder like meat
Hi, I have TMJ. I had been having botox for teeth grinding, for the last few years. Do you think this played a part of my disorder?
Thanks denise
The teeth grinding, yes. Botox, no.
Hello. Thanks for the article. I have been in a pivot splint for over a year (designed to bring the mandible forward). I now sleep in it at night as it keeps me from clenching. I’ve seen an OMT for tongue posture and a cranio-sacral therapist. The pivot split and mandible movement has made a noticeable improvement (I have a partially dislocated disc). The issue I’m still having is a ton of tension with muscles leading under my chin and into my neck. They create a pulling sensation that creates alot of apprehension. I need some dental work and I’m terrified of laying back in the chair where my jaw will assume the old position and the disc could catch. It makes my muscles quiver and feel wonky. The dentist wants to sedate me to do the work. Any suggestions on lessening the pulling sensation from the surrounding muscles?
Anxiety / stress. See my videos on the topic of relaxing the suprahyoids.
Can you link these videos please?
I’m 21 years old I’ve been getting pain in the TMJ area and after reading this article I’m starting to gently push my lower jaw forward. I feel like the pain is getting slightly worse, is it normal for it to initially get worse before it gets better? And if so for how long? Thanks for the article doctor.
Make sure that you’re not clenching the suprahyoids or tensing up too much. Some fatigue and worsening of the PTERYGOID MUSCLE is normal but not of the joint. Some people have to start with just 1-2 hours per day and gradually increase to all day, if they’re very weak in the pterygoids. Book a skype session if you can’t figure it out.
Great article doctor, learned a lot from it. So I’m definitely slim and have low body fat but you can see my hyoid bone has dropped as you said, cause my jawline is not prominent at all and I assume its from the forward head posture I’ve had most of my life. So if I just simply fix my head posture and start protracting my mandible, my hyoid bone will rise?
Check my youtube video on neck tucking
hi. if my MRI shows that my tmj is normal. should i believe that? because i still have pain
No
hello, i would like to say thank you. although i’ve started to have this problem only recently (most likely to due teeth clenching which i have developed in the past year, and a pre existing slight overbite) the daytime headaches and the pain in just a few days are reduced quite drastically (i am also using an occlusal splint for the night). one question though: when i first started to notice tmj problems a few weeks back, such as left jaw clicking, facial pain and dizziness, i noticed that my bite had suddenly changed (my lower jaw shifts to the right and i have a midline discrepancy). this has definitely caused changes in my face, i feel like everything has been slightly rotated counterclock wise. now my question is: will the decompression of the tmj realign the jaw back into its original position? i’m quite sure it is not a dental problem, as the upper and lower arches used to fit perfectly when the molars were in contact.
No, it’s a permanent change. You gotta chew like you would normally (with your molars).
Dear Dr. Larsen,
Thank you for this. I had some questions
Is it possible to know what is the right amount of protraction of the mandible?
Is it okay if the protraction is towards one particular side (towards right in my case)
My tongue feels tired after sometime and the muscle on my upper lip hurts(only on the TMJD side). Is this normal.
Thank you for your time.
1. 3-4 mm is usually sufficient
2. No, pull it straight forward. If you feel the jaw is uneven, it’ll straighten out once the pterygoids become stronger (strengthen them once to twice per week)
3. Some patients benefit from keeping their tongues down in the beginning, as it may make it harder to keep it up while simultaneously keeping the jaw forward; they reintroduce proper tongue posture after learning to keep the jaw forward.
Thank you so much for presenting so beautifully
Your post has been very nice. I am very happy to see your post
Thanks for the valuable info. I have only been doing the correct opening/closing of the jaw technique for 2 days now and I noticed less popping/noise in my jaw. I was amazed to wake up without a headache even though I’m pretty sure I haven’t figured out protracting consistently.
If I understand correctly we need to protract the lower jaw with sealed lips with the teeth not touching. The tongue must be flat against the upper palate without touching the teeth. When I looked up mewing exercises, many articles said that the teeth should touch lightly for the back of the tongue to lie against the palate? My question is should we keep the gap between the teeth without having a hanging jaw or be aiming for light touching of the teeth while protracting?
The incisors can gently touch, but if they don’t touch that’s ok too. My teeth gently touch. The tongue can be down while you’re learning to hold your jaw forward but eventually you’ll want the tongue up also.
I have tmd issues and a large overbite. Through xrays I was told the pains in my neck, jaw and head are from enlongated styloids and calcified stylohyoid ligaments causing Eagles symdrome. What are your thoughts on Eagles? And is surgery the only cure?
Depends if the diagnosis is correct or not. If it is correct, then yes, styloidectomy, and with good results.
Do you have any input on best sleeping position? I find that no matter whether I comfortably sleep on my side or try to sleep on my back, I always wake up with clicking and popping in my TMJ again. Would it be worthwhile to get a night guard, even if I’m not a night time grinder? What about some sort of chinstrap. It’s almost like my mandible hyper-relaxes in my sleep and once again has to be popped back into its rightful place in the morning.
If you struggle at night, get a splint that pulls the jaw forward. The dentists often refer to them as “anti-snoring splints”
Recognizing myself in a few of these examples.
I’m not a big believer in adult mewing, but what’s been outlined here makes sense and I’ll give it a shot.
I actually have a hunch that a nightsplint I got a year ago might have exacerbated the problem by being shaped around central occlusion, therefore pushing the mandible back.
Just to make 100% certain I understand: The mandible protusion will initially have to happen consciously, and will feel unnatural and strenuous to the underdeveloped pterygoids, correct?
And is there such a thing as overdoing this?
The splint must pull the jaw forward.
Yes.
Patients with very weak pterygoids may have to gradually introduce the postural change to avoid overloading of the pterygoid.
Hey Kjetil, thanks for the great article.
I’d like to ask a few questions:
-I recently started mewing, I feel that mewing works the pterygoids, could I get TMJ dislocation from overloading the lateral pterygoid? I think sudden mewing would tighten/ spasm the pterygoid, pulling the tmj disc out of the condyle
-Also, I see that many people recommend splints to bring the mandible forward, however, wouldn’t that only be temporary, and
wouldn’t pulling the mandible forward push the maxilla back?
Thanks, Ken
Keeping the mandible forward does not affect the maxilla in adults. It might in teens, and definitely will in children. You’d have to make a pro/con evaluation. Mewing is good for children and may also work pretty well for teens. For adults without pain you can do Mewing, for adults with pain I recommend a splint or simply holding the jaw forward.
Is it fine that in order to protract mandible forward I have to also move it downwards?
I don’t even have any TMJ pain yet, it’s just that after starting to improve posture my mandible automatically started moving forward towards underbite, and my upper incisors (because of recessed maxilla) won’t allow me to do it comfortably (verticaly, not only horizontally) forcing my mandible to move down.
I would probably do Mewing instead of this protocol if you don’t have any pain. This protocol is for pain management.
Last 2018 I opened my mouth too wide and I felt the popping sensation and my left jaw got locked, then September this year I was able to unlock it and the popping stopped too, but the popping came back (no lock) because I chewed too hard.
But just this week I accidentally hit the left of the mandible (same side that has TMD) while opening a door, but for some reason my right tmj started to pop too. Do you think that the disc got displaced, or did it just get a trauma and will heal if I let it rest? My mouth was closed when I hit it so I’m wondering why the other side also got affected by the shock. Many thanks!
Popping means that the disc is subluxed, and recaptures when you open the mouth. It’s not dangerous. Just follow the steps in this article.
What a refreshing article. I have TMJ dysfunction. Symptoms are better but no resolution after 3 months. I haven’t seen any comment on this so thought I’d ask.
Is there any wearable daytime device to encourage correct mandible forward posture? I was thinking about using an anti snoring type of device, e.g. SnoreRx, to help me correct my jaw retraction. However, I was thinking of wearing the device during the daytime as a training aide. Bad idea? Currently, I constantly protract jaw forward using muscles only.
Thanks! Don
You can try this if you want. Some patients struggle with either motivation or are very sensitive. In these cases, a splint might be a decent option, at least in the beginning.
Hi doctor, I’ve always had forward neck posture and decided I wanted to fix that, so lately ive been working on having my shoulders back and chest out, and neck straight instead of hinging for the past week. I feel like I have the right posture after reading your article but I’m now getting alot of pressure in my temples thats resulting in headaches, like heavy pressure in the temple area. I feel like my traps are pretty strong already though as I work those out alot at the gym. I want to maintain this good posture but this pressure in my head is killing me.
You’re probably pulling the neck too far back (ie. doing something wrong). I suggest that you setup a skype session.
Hello doctor,
I have an overbite (5mm) and tmj issues. Is it ok for me to follow the article?
And how much mm should I protract my jaw?
Thank you!
Not a problem. The second question is answered in the article.
Hello Doctor. This is an excellent article.
I started following the procedures mentioned about 4 days ago. Pain has gone 95% away and I used to have big problems with swelling in the face. That has mostly gone away too.
I’ve been trying to hold this position at all moments while awake besides eating. The first two days my face was on fire. It wasn’t pain, but soreness. I went through it and the next few days, it mostly went away. Now I’m not sure if the pterygoids are overworked or they’re stronger, but it’s harder to identify if I am doing it correctly, mainly because I am not feeling those same indicators. At first I could feel my mandible protract forward, but as time went on, it got harder to differentiate protracted mandible to non protracted as that posture got normalized. I use my incisors as an indicator and can tell the difference when I retract my mandible, but I fear it may become inefficient. Does activating the pterygoids muscle automatically bring forward the mandible or must you manually bring out the mandible forward mechanically?
Also, is holding the mandible forward with the pterygoids strengthening those muscles, meaning the exercises mentioned aren’t needed if they are already being strengthened?
You’re just getting tired. Give the pterygoids a week’s break and try again.
Hey I’m 13 I hard mewed improperly now my left jaw muscle is more developed than my right jaw muscle and when I the 4mm thing my left jaw muscle gets activated and I was wondering whether the muscle will get bigger or not
Then Mew properly. You have plenty of years to even it out.
Do you think hard mewing for years as an adult would be able to move the facial bones and affect the cranium/brain negatively?
Do you think hard mewing for years as an adult would be able to move the facial bones and affect the cranium/brain negatively?
Negatively, doubt it. I think Mewing works for children and adolescents. Does it also work for adults, ie. regarding facial development? I don’t know. I don’t recommend Mewing for TMD treatment for adults but I think it can have a great impact on children’s facial development and is definitely recommended for children. I respect the Mews
Hi Doctor. When you say, “Posturally protract your mandible 2-4 millimeters from maximal retraction (most important). Sometimes more than 4 mm will be required.” do you mean to push back your mandible as far back as possible and then protract it 2-3 mm forwards. When I try to do this it feels like my mandible is further back than where it naturally rests, and it feels like I have an overbite.
Thanks
I’m inclined to say no. I think you’re OCD-ing about this.
I have been dealing with tinnitus and jaw clicking for the past two months, and this article was one big epiphany to read. Absolutely brilliant.
How long does it typically take for your tinnitus/TMD patients to see their tinnitus subside once they start these postural practices? I am on day 5 now with considerable improvement on average, but sometimes the facial/jaw muscles seem to get tired from the new posture and the tinnitus spikes. Thank you for your incredible work on this subject.
Varies from patient to patient. If you already got relief in 5 days, you’re probably doing a good job.
Hi doctor,
My story might be a bit different than most of your patients.
Ive never had jaw issues in my life but last year I started chewing a lot of gum after hearing about the benefits it has for jaw growth. I was a dumb kid and did it for hours daily. One day I woke up with a sore jaw, and popping noises in my ear. my ear would pop when I burped and yawned and I would hear cracks when I opened my jaw.
I went to a dentist and he told me since I don’t naturally clench/have bruxism, quitting gum and switching to a soft diet will solve my problems. I listened to his advice and 99% of my symptoms dissapeared within 2 months.
However, it’s been half a year and the ear that I had these symptoms in keeps randomly twitching. I’m not sure what’s the cause. Sometimes when I eat harder foods that ear gets liquidy and some of the ear pops come back and my ear starts twitching faster. But when I stop chewing the symptoms dissapear within 5 minutes.
Do you think your advice will help my case? I’m going to follow it and let you know if it helps.
Should we do both exercises to strengthen lateral pterygoid and medial pterygoid?
I only have pain in the lateral pterygoid. Does this mean its overworked and does not need strenghening? Or is it weak and needs stregthening?
Strong muscles don’t hurt
You said in a reply to a different comment that you shouldnt protract the jaw if you don’t have any pain, and only do mewing in this case.
I don’t have any pain but have eustachian tube dysfunction symptoms (that get triggered when I chew). So would you advice against following your protocol in my case as well?
That’s only for children and adolescents
Thank you for writing this article. I’ve noticed immediate effects from jaw protraction, as well as how to avoid mouth breathing.
In doing the protraction exercises, I had two questions:
1. I *think* when you do the exercise, you protract and lower the jaw, then reverse by moving the jaw back up and retracting to a normal position. But maybe it is more like a circle, so you protract, lower, retract, raise? I wasn’t clear on this.
2. In doing these exercises, I’ve noticed that my left side (where I have the TMJ) is weaker than the right. Precisely as you’d expect. Should I attempt to work the left muscles more by moving the jaw to the right a little bit?
Thank you very much and I’m sorry if the answers can be found already in your post.
1. No, the protraction gradually reverses. It’s literally the opposite of the opening. You should not retract in the bottom.
2. No
Im 17, gonna be 18 in less than a month. When I was a younger I had an underbite and got a retainer for it. Now I have an overbite and tmj/tmd (still not 100% sure of the difference). I realized a couple weeks ago that I have bad sleep apnea. I realized a couple days ago that I am constantly tensing my tongue, because when I don’t my airway is blocked (even when I’m standing straight up). The only way i’ve managed this is by sleeping on my stomach and letting my jaw hang. I got invisalign for the overbite so I’m still on the trays. When I jut my jaw forward my incisors align (or they create another underbite depending on how far I push my jaw out), but everything else doesn’t touch. I also wanted to add that I ‘naturally’ have a correct jaw opening. Should I just mew and let my jaw hang? Or should I new and jut my jaw forward? Or should I mew with my molars lightly touching (even though that brings my jaw back)? I’ve read all the comments and saw that the treatment dependent on everybody’s situation so I just wanted to be sure. Also wanted to say thanks for this wonderful article!
Amazing article. Thank you! I’ve been on a wild goose chase for the past month trying to understand where my blurred vision, headaches, tinnitus and hyperaccusis were coming from. I’ve even had music in my ears and auditory hallucinations! First I had a lumbar puncture as they thought I had a brain infection. Then, they thought it might be a mental health condition. However, a quick trip to my dentist revealed lots of teeth grinding and jaw pain. Plus my spinal MRI showed a minor thoracolombar scoliosis concave to the left and minor discal dessication at C4/5 and L5/S1. Singing teachers always told me I stick my head out too far forward. Plus I have an overbite, lower crooked teeth and breathe a lot through my mouth.
Are these jaw and back problems likely behind the other symptoms? I’ve also found that sometimes my lower back starts to spasm and then I get spasms all down my right side from my foot all the way up to my head. When this happens the muscle clenching and tinnitus suddenly get worse.
I already do tons of Pilates so will keep doing those to help my back, along with your postural and jaw exercises.
However, I think I’m still tensing my supra hyoid muscles too much during protraction (I find that the pain changes from one side of my face to the other every few days and it tenses on whichever side is painful). My neck and back also hurts a lot. Should I focus on the jaw exercises to strengthen the pyterigoid muscles more first before doing the constant protraction? And is it ok if the neck and back hurt? Basically, how much pain is ok and how much is not ok? Sorry for the long question and thank you so much, in advance. Having had surgeries before, I’m really keen to try the conservative route here.
Should someone with eustachian tube dysfunction try this? I do not have any pain but my ears become full and liquidy from time to time. I am certain its caused by my tmj joint.
I’m not convinced that this is coming from your TMJ, but you can try.
Ironically I noticed my TMJ because advice from your videos led to me being able to maintain my overall body and particular my cervical spine in stronger and stabler positions. It seems as a result the TMJ ‘cracking’ I had taken for granted for years disappeared for a long time as a result. It just came back recently and I decided to research it properly and came across this article. I got immediate relief when I postured my jaw like you suggested.
Thanks for all your great research and presentation. The only question I have is how do you feel about more invasive interventions like jaw surgery or MARPE? Knowledge and techniques have improved my condition a lot, but being realistic about being an adult with a crossbite and maxillary restriction, I don’t think I can achieve permanent relief without skeletal expansion.
Good job. I am a proponent of maxillary advancement surgery in some cases.
Thanks for this amazing article.
My symptoms started out of no where two months ago. After portracting the mandible by 3 mm I feel better. However what is strange about my symptoms is that when I lay down, all of them go away. When I stand up they go back to normal almost immediately (Eustachian tube dysfunction and stiffness of the jaw for opening and closing) do you think the issue is from somewhere else other than my tmj?
I started noticing TMD about 3 days ago. I was practicing mewing for a few months. I had mistakingly thought my molars needed to touch so my maxilla was always retracted.
I naturally started protracting my maxilla to prevent pain but started to become paranoid that my bite has become messed up. I didn’t know if it was natural to protract as much as I do when I relax my jaw so it’s relieving to read this.
It feels like after a long period of a relaxed slightly protracted maxilla, when I do need to retract to eat, it feels like my bite is off slightly. My top front teeth touch my bottom teeth. After eating for a while, it seems to correct and I find the right position. Perhaps this is caused by inflamed TMJ? It is painful when I do end up retracting to eat.
Is there any danger to allowing the maxilla to set in a protracted position for long periods or is this needed to heal the TMJ? I fear my bite will get messed up.
This could just be paranoid thinking but I want to ensure I understand this correctly. The mewing was a big mistake and I’m hoping I didn’t cause permanent damage.
Get your anxiety under control
You won’t believe how much i am grateful for your article! Thanks a million!
unfortunate my dentist have forced a greater opening on my jaw about a month ago and it increased my jawlock symptoms he aslo prescribed exercises to stretch the muscles and open my mouth wider to “relieve spams” . the digastric, suprahoids and scm are very tense right now and they are clenched even more when i try to maintain the new posture. do you think switching to a very soft diet for about two weeks to a month while getting used to this posture is beneficial to lessen the spasms and let the disc heal?
Or just do what I recommend in the article?
Thanks for your reply! I am following what you suggested exactly. it’s just that my mouth opening is quite limited, even with the new mechanics it’s difficult to open the mouth for a normal diet. i don’t mind pushing through the difficulty. however, i fear i will be inflicting further damage to the the whole area like my dentist did with his forced mouth opening
You need to give it time to recover. When you move the jaw forward, the disc gradually heals. Don’t push through the difficulty, give it time.
approximately how long will it take to get out of a jawlock (about two fingers mouth opening) after doing your recommendations when it comes to opening mechanics and posture?
Varies from patient to patient. Get an MRI
I am not able to perform protrusion movement of the jaw. Since my disk was displaced, I am only able to open and shut the jaw. The 2 other movements (sideways & back/forth) is impossible and has been for 2 years. What could the reason be and what’s should I do?
Would have to see the images
– What if my upper incisors are too far back and down and prevents me from protracting my lower jaw?
– Is there any risk to trying a splint? Could it permanently put me in an underbite or make my face longer?
1. that makes no sense, as your lower jaw is separate.
2. No.
Mr. Kjetil you are a legend!
Should we protract the mandible even more than the already done portraction in the new posture when opening the mouth? if so by approximately how many millimeters before depressing it? i was doing almost maximal portraction when opening but it feels off
i did watch the video you posted about it, only this little detail is confusing me
Kind regards,
John
Thanks buddy
Yes. Don’t overthink
Been implementing what you recommended and it’s life changing. I wish you all the best man!
Do you recommend any supplements to help the scar tissue/joints become in better health and heal faster? I have had issues with this for about 5 month now and I hope I can at least counter some of the damage.
I also read “Anna” comment and I think it’s detrimental if you change to a soft diet as not using the joints will make them less lubricated, am I correct Mr. Kjetil?
Hi, happy to hear.
1. No
2. No
Hi, my jaw is deviating slightly to the right when using your mouth opening, should I continue normally and it will resolve with time or should I try not to let it deviate?
I am getting a bit of eustachian tube dysfunction after the new posture, can that happen from weak pterygoids?
The deviation is either due to disc subluxation, pterygoid weakness or simply structural. The two initial options will resolve gradually if you follow my protocol. The eustachian tube problem is usually neck related, my if you feel it after changing the jaw posture then it could potentially be caused by trigeminal dysfunction and will resolve gradually as you get accustomed to the new posture.
Is jaw deviation when opening to one side a sign of disc displacement?
Will it resolve on it’s own while doing these exercises or should we try to make not deviated.
Usually, yes. Yes it should resolve spontaneously as you decompress the joint and give it some time.
I see a lot of people praticing mewing have struggled the side effect of mewing such as headache, eyeache, teeth changing position, tmj,… Can you explain the reason and introduce the way to get out of it?
I respect the Mews but I don’t agree that patients with symptomatic TMD should be Mewing, as it worsens the joint compression. If they’re very young, it some exceptions could be made. I must emphasize that I completely agree with the Mew approach for non-symptomatic patients (patients without jaw pain) who have stunted maxillary growth. I have been mewing myself and I also follo the mew principles for my son. We have nearly cured my 6 year old son’s very stunted maxillary (congenital) development at this point by following Mew principles.
My right mandibular condyle is popping out of the fossa a little. Will this resolve within time on it’s own after following the mouth opening protocol you made?
Regards,
Jack
It may ameliorate as you learn to open the jaw properly, but the ligamentous laxity will probably not reverse to previous state. That said, my experience is that you can still become completely pain free by following the principles in this article.
I’m so glad I found this page! Incredibly comprehensive. Amazing work good sir!
What if I am not sure in which direction to protract the jaw? It goes zig-zag kind of and also pops when I push it forward.
Just do your best. the zig-zagging will improve as the discs heal.
I am going to spread your article everywhere. No other good resources about tmj online.
Can jaw deviation cause trigemnial dysfunction only on the side that it is deviating to while opening? as the symptoms only happen when opening the mouth.
My disc is displaced slightly sideways and anteriorly. will following your protocol religiously solve it within time?
Unlikely to be caused only by that. Probably a combination of several factors. yes, you should be fine if you follow the protocol.
Hey so I have trigeminal Neuralgia symptoms and also have tmd like symptoms and jaw pop and discomfort, my question is if my trigeminal neurgia is caused by my tmd and I solve the tmd with your protocol will by trigeminal neuralgia go away? And also if my trigeminal neuralgia originates from something else can this protocol still help?
If Costen’s syndrome (TMD-induced TN), then yes, of course. If it’s coming from somewhere else, then of course not. But most incidences of TN originate in the jaw, and then some few cases develop due to intracranial pressure exerted on the nerves as they emanate from the brainstem. I have seen huge sucess in treating TN in cases where there is a normal brain MRI and the patient’s symptoms worsen with chewing. If your symptoms do not worsen with chewing or similar TMJ-strain, then it is less likely.
Do you recommend just maxillary advancement or maxillary and mandible advancement for very stunted maxillary development? Thanks.
Just maxillary
Very informative article…
Over the last 4 years I have had a lot of issues with my jaw shifting to the right (5mm) and when I sleep I have a lot pain in the base of my skull. I’m currently seeking care with an Oral Surgeon that suggest that I have orthognathic surgery….I ‘m looking for any and all alternatives. I’m also exploring an orthogonal chiropractor….thoughts?
Planning to start the above mentioned exercises as well…..any other suggestions you would have for me?
Happy new year!
I have a mild medial disc dislocation due to trauma. does it resolve on its own as well after following your method?
Probably
Hi Kjetil, thank you for the article. My jaw clicks a lot, going left to right, it seems like a misalignment. (The clicking is mostly on the right side). When I push my jaw forward, I can’t work out if I should be in the left alignment or right alignment.
Do you have any thoughts on this?
You’re overthinking this.
Does strengthening excercise help chronicaly tight lateral pterygoid? I have tightness on one side lf jaw when I open my mouth. After I chew my food I start having great tightness in it. It is very tender. I even start noticing tingling and numbness in my cheek area. I have been recommended botox but I think your approach makes much more sense. My jaw also deviates to the side that is tight. No disc displacement yet though. No clicking or popping as well.
I want to solve this as soon as possible as I read the tight pterygoid over time pulls the disc out of place.
Thanks for your time man!
Tight = weak, in most circumstances.
Hello Mr.Larsen.
I have had an infection in my upper molar and have done root canal and taken anti biotic to treat it.
I now have jaw deviation upon opening and I am suspecting pterygoid failure. Can this happen after an infection and prolonged dental treatment? Will it resolve with the strengthening or I need to take some meds first?
Can’t answer this one without consulting. Could be neurogenic, or could be MSK.
I have been burxing heavily for about a year
after doing the protraction. It stopped for me thank you very much!
My muscle are super tight and mouth opening is tight from all this time clenching.
I also had some jaw muscle injuries from dental treatments.
Do you think it could take a long time to get back normal function? like more than a month? Should I let the muscles relax for a bit and get good sleep before I do the strengthining?
Give it 3-6 months but don’t train too hard
Do you recommend ultra sound therapy for mascular tmj? I don’t have pain, MRI cleared my joints. I just have a level of discomfort when speaking and mild tightness during the day that is worst when waking up but goes away pretty quickly after moving the jaw a bit. My phsio said this could be scar tissue and adhesions on your muscles which is causing restrictions and recommend Ultra sound therapy with great expected results.
No
I am really confused tbh. I have undergone orthognatic surgery 2 weeks ago. I have been recommended rest and stretching starting from week 3 to gain jaw mobility because the surgery overloaded the ptergoids. Some sources recommend only rest some only stretching. You are recommending strengthening which the first time I heard. Which one do you think is best to prevent permanent trismus after surgery
Kind regards,
Daniella
You’re missing the point here. What you are talking about is a temporary condition. This article is for TMD treatment.
Can tendon inflammation cause jaw tightness by effecting the nearby the nerves?
Yes, see what I write about the pterygoids
Very informative read! Quick question, most ringing and tinnitus that is TMJ related changes in pitch as the jaw is moved around, correct? Does it make sense that the ringing would get slightly louder when the jaw is protracted? When only moved forward a couple millimeters, my change is minimal or zero, but if moved into intentional overbite territory, it gets quite loud.
Are my top and bottom front teeth suppose to touch when I protract? I’m not sure if I’m doing this right. Should my lower teeth be resting just behind my front teeth?
Depends on your baseline position. That’s why I recommend 3-4mm forward rather than giving you a teeth alignment estimation.
You once commented on youtube about jaw surgery saying:
Maxillary advancement surgery will decompress the TMJ. It should be done at a light oblique angle, to put the maxilla forward and ever so slightly down. Worsening may occur temporarily due to tremendous induced load on the pterygoid muscle, but as I said, this will pass within some time. You can take my advice or leave it. Good luck.
How do you overcome this overload, is it just by complete rest? and how long it may take to be back to normal?
Rest it off, then gradually increase their work capacity.
Thank you for this fantastic article. It is the best information I’ve found on TMD. Will working on this help relieve jaw clenching during sleep? I’ve always had this issue, but it has become progressively worse as an adult. Thank you!
Yes, it can, but I still recommend using a mandibular advancement device for those patients who struggle with night clenching
I had Covid-19 in january, and since then, I have these TMJ-like issues. I clench my jaw because I have lots of stress, my jaw joint hurts, I have head aches and often my left eye muscle is very tense, and I recentlt got very light tinnitus in my left ear. Can TMJ occur within ‘just’ two months? Just moving forward my lower jaw will suffice?
1. yes 2. depends
does this approach fix oromandibular dystonia? My jaw involuntary spasms to the right as soon as I open the mouth with electric feelings in the cheek
Depends on the cause. Tends to be an upper neck-, rather than TMD, problem in my experience.
Do you think dtr fixes muscular tmj or not?
I saw videos of a dentist in the us who is preaching as the best fix for mascular tmj. Does just strengthening the muscles have the same effect?
Depends on who you see.
Can nerve entrapment in the pterygoid cause to spasm once used? I get a feeling of shock like painless tingling then it kinda stops moving which limits my jaw opening.
Extreme weakness of the muscles can cause spasm, yes. Don’t go too hard too fast. Give them time to recuperate.
I have zero pain in my joint and I actually have a well developed face so my joint is not compressed. I can go back about 3-4 mm from occlusion. I am under very high stress recently and I am clenching my teeth all night long and unfortunately can’t control the stress very much right now. Is a normal fitted night guard good for me now at least until the stress is gone?a mad appliance will push my jaw way forward
Holding the jaw forward during the stressful period will inhibit you from clenching. Using a mandibular advancement splint during the night can also help. This, of course, until the stressful period has been terminated.
I tend to hold my breath when I am opening my mouth or while focusing on basic tasks. I am a chronic clencher it seems. meditation is not helping, do you recommend anything other than awareness of it. I am all tensed up while writing this comment, it’s like it’s in my dna.
I am afraid of drug therapies as I heard they increase bruxism if you know of any that doesn’t have a bruxism increasing effect please let me know
Sorry to hear this. The treatment for this, in cases where self-awareness has not helped (despite trying over a long course of time), then there might be some types of counselors or drug therapies that can help you. Reach out to a psychologist or similar professional.
i have tmj syvonitis and have been recommended arthroscopy. do you think this approach is better for the treatment of my condition?
Can’t comment on that without assessing you
I saw your article posted on tmj groupm
Does the great auricular nerve effect this at all? Can it cause jaw spasm when opening mouth. I have it only on one side.
Will training the scm and scalene solve it then?
No
Do you make an exception about releasing tension from the pterygoids just twice before strengthening if one was bruxing heavily for a while? My medial pterygoid is super tender and very tense so I am wondering if I released it twice during one week before stretching is better.
Bruxing does not stimulate the lateral pterygoid. As to the medial, I usually don’t focus on it that much.
I just read your published study about myositis of the pterygoids, I think this is what is happening with me now from all the past clenching (chronic myositis). so gentle strengthening is the way to go? not letting it recover on it’s own or releasing.
Depends on time frame.
What about the temporalis tendon? is this a muscle you allow the release of?
I have chronic tendonitis which is just a feeling of pressure around the jaw joint and it limits my jaw mobility big time, it happend from jaw clenching.
Yes
Thanks man!
for me the problem is either medial pterygoid tightness or a mild form of ernest syndrome of styloid ligament laxity from forward head posture. My only symtom is tenderness at the angle of the mandible, no other symtom and yes if I press on the ligament it hurts a bit. Will terminating forward head posture fix this problem within time if it was ernest syndrome in it’s early stages
Man I can’t express how I am grateful for your suggestion about getting mad appliance for bruxism.
I have suffered for heavy bruxism for 2 years and it never stopped, it’s in my muscle memory. My life has been miserable, my face is always on fire. my jaw barely moves and it’s super tight, I barely speak a bit and it locks up. I wouldn’t say my bruxism has stopped completely but it’s 85% better. Can I expect a recovery from this condition of Supreme facial tightness if bruxism is terminated soon. I don’t mind if it takes a full year as long as I can return to normal later on (no problems with the joints, Just purely mascular).
Thank you for the article and taking so many questions !
Question is … how long do you have to practice this ??? After you get some symptom relief do things just go back to normal ? Do you have to continue forever ? Is there a bite change eventually needed?
Thank you !
Depends if the cause is related to clenching or due to frank craniofacial dystrophy
Do you think the pulling on the mandible from the suprahyoids during FHP can cause overbite?
Keeping your mouth open during childhood and adolescence along with poor tongue posture is what causes craniofacial dystrophy and malocclusion, cf. John Mew’s work
Thanks for replying.
I tried Mike Mew’s method of “mewing” for 3 years and it did very little. Then I tried combining it with your method of protracting the mandible and results started showing just after a few months. It’s a game-changer both healthwise and aesthetically. You sir are a genius!
What do you mean by aesthetically? Are you saying your skull changed shape?
Can the streghtening protocol be used to overcome a jaw overuse chronic injury?
Combined with good nutrition and adequate rest?
my jaw have been rigid for 5 month since I had multiple lengthy dental treatment and stretching and rest hasn’t helped at all.
I have had multiple treatments for my TMD over the last 25 years. I clench to the degree that I popped a bracket off my permanent upper retainer. I had a consultation with a dentist specializing in TMD recently. My jaw bone is completely compressed into the socket on one side both top and rear, and the other side is rear. The discs are not even seen in the X-rays – even when zooming in. They showed me where the bone has “remodeled” the socket on both sides from constant compression and how the shape of my lower jaw shows severe clenching. The suggested treatment is to lower the bottom jaw and bring it forward using splints. In the office, I couldn’t even get it far enough forward to stop the popping and shifting. Does this sound like a reasonable treatment? Is it usually successful?
I’ve been practicing most of these for 6 months, had my jaw forward, but it is still clicking and moves zig zag 🙁 I have had it soon after I got braces and since then it’s been 5 years. It’s so depressing, I’m 20 :/
Might be night bracing, or you just need more time. Generally, significant pain reduction is seen within a few months. You write nothing about your pain levels and whether or not they have improved.
I did notice something going on with my jaw when I started practicing what you wrote here. Pain did reduce a little but when I hold it forward for long time side of jaw hurts and clicks really bad.
Ok now I feel like I can touch my joint on left side, like it slips and it pulls my face to that side, is this a good sign or bad?
Hi,
I bought a jaw excising tool and it gave me tmj symptoms. After I stopped using it and switched to a soft diet, within 2 months 90% of my symptoms went away. But, whenever I try to chew harder foods I get pain near/in my ear. I’ve had an MRI and there’s no sign of dislocation. I’ve been doing your lateral pterygoid exercise (since that’s near the ear) and I’m not sure if it’s helping. Do you have any other advice?
How frequently should these be done? How many sets/reps? Daily? Weekly?
Thx!
does this approach fix internal derangements within a certain time. mine is antro medial and am hoping this is going to help. thanks!
It feel weird when I get my teeth back in contact after portracting my jaw. is this normal? it feels unnatural and like i am pushing my jaw way back on purpose. (it felt normal previously) is this a common thing or maybe is it a change of bite?
Yes, ish. It does suggest loss of vertical molar height. But it is quite normal for these patients.
good information dan thanks
Would this forward movement overtime cause irreversible stretching in the ligaments?
No.
My tinnitus is worse when I protract my jaw. It goes away when I retract my jaw. If I turn my head towards the shoulders, somatic tinnitus disappears when I retract the jaw. Seems counter to what you are advising. Please help. Thanks.
Compression increases when you pull the jaw back, which may cause temporary numbness and improvement of symptoms, but afterwards will result in worsening. As of deleting your comments, I am not. They are sent for moderation. Take a second to look at the message from the system before you complain. With regards to following my advices, you take my advice or you leave it.
Hey what exercises would you recommend for temporalis tendonitis? You’re post touched on it a little under the heacache section and it mentioned jaw retraction but Im not too sure. Thx
Stop clenching your jaw
How do you convince a surgeon that your lower jaw (mandible) has overgrown beyond your upper jaw, but it needs to be moved forward enough to produce an underbite (which you had most of your life without problems and without TMJ/TMD)? I am having much difficulty getting a doctor to believe me when I’m trying to fix my TMD, which now after reading your website I understand that my lower jaw had grown longer than the upper one, causing a discrepancy. They seem to have this obsession with an equal bite, which was never possible in my case. How long before I notice a difference with TMD after maxillomandibular advancement surgery of 8m? Thank you.
They would probably do 8mm upper and 5-6mm lower, then. This isn’t protocol, which is why they are hesitant to doing it. You would probably have to sign a waiver. I would recommend that you go for conserative options insteada
Is it possible to move the mandible more forward while you are an adult? I want the TMJ to move forward since I feel it is still backwardly displaced. I have muffled hearing and those other symptoms mentioned.
The problem is the postural element, I had an underbite before with no TMJ for most of my life, and had much better posture, now it’s too forward and it’s causing me thoracic outlet syndrome, tinnitus, and host of other issues. How do I get back to normal from that? I went to visit one doctor in Germany who tells me 50% of our posture comes from the jaw alone.
What is your opinion of Endoscopically Assisted Surgical Expansion (EASE) to expand the maxilla? The rationale of the operation is based on the findings that people with narrow jaws result in constricted nasal airways and posterior tongue displacement with resultant airway obstruction. Do you think this would be helpful for someone with TMJ? I have a narrow maxilla, and I’m mainly getting the surgery for sleep apnea issues, stuffy nasal breathing, and improper tongue posture due to a lack of space in my mouth. do you think this could also help with my TMJ, on top of the postural lifestyle changes that you recommend?
I was going to get the surgery regardless (for my apnea), but I was intrigued by your description of a narrow maxilla’s role in compressing the TMJ joint, and I am hoping that I can kill two birds with one stone with this operation. Also, the operation would create more room in my mouth and allow me to achieve proper tongue posture easier.
Can you recommend a really good clinic in Mexico or USA for proper TMJ diagnosis and treatment?
Hi KJetil,
Thanks for the helpful advice.
Do you think TMD can be caused by retractive orthodontics? If so, beyond surgery is palette expansion and tooth repositioning a possible resolution? Cheers
1. Without a doubt
2. If they do not over-expand the mandible
Hello,
My joint pops when i do the protraction oipening/closing. Is that ok? I have severe face pain due to tmj which developed 6 months after the pandemic started and we were left sitting at home office.
Yes, but if it pops aggressively then it will probably be sufficient to just do the protraction (postural change) until you are a little better.
Hello there and thank you for this article. One queston, how often should i protract my jaw to full extend? Or needs this be done all the time?
thank you
Hello, this is a doubt That I have already for a while, if you can answer will be of immense use! Can the hyoid bone popping have any relation with tmj/tmd??
Suprahyoid clenching
When I try protracting my jaw, I feel pain and discomfort in my TMJ and a headache. Is this expected? Should I be doing something differently?
Give it some time. Make sure you don’t overload the pterygoid and make sure you don’t clench the suprahyoid.
I have right sided jaw soreness/ TMD. When I protract the jaw, I experience pain on the inside of my right mandible, right pharynx, and the area just anterior to the right ear. Should I fight through the pain and continue to protrude the jaw?
Pharyngeal pain is usually not a component of TMD. I suspect there’s something more going on here. But yes, protruding the jaw (with some exceptions, eg., pterygoid inflammation) will make good results with some patience. I recommend booking a session to evaluate what’s really going on.
If one started this protraction at a young age like 14 would there be any permanent facial structure changes after about 2 years or so, because I think we’ve noticed this in our son.
I wouldn’t really recommend this protocol to a developing child unless their symptoms are very aggressive. There are other ways one can treat TMD to avoid the facial changes that it would bring in children.
i can’t tell if my mouth opening is correct or not. if i try to protract the jaw and open i will have to retract back to normal to open it fully. also how much distance between resting mandibular position and maximal retraction should i feel to know if it’s normal? are a few millimeters okay? lastly, it may seem like a silly question but i was wondering if it is normal to not be able to open your jaw to the fullest while smiling at the same time? i don’t really have tmj problems at the moment but some things have made me very paranoid about it lately
You are overthinking too much
I may have an entirely unique situation. In my late teens, hating a small chin, I began protracting my jaw forward to make it look stronger. Usually the bottom front teeth were in line with the top. Sometimes a little back. This became a habit and I did it for about 19 YEARS.
After probably 15 years or so, I started to clench and was diagnosed with bruxism. I lessened the protraction over time but still did it to a degree. Tinnitus kicked in and eventually I stopped.
Since stopping, TMJ symptoms worsen. Hearing loss in an ear, 4 tinnitus sounds, tension headaches, and now the newest and worst, pain.
I had braced as a kid, an expander and wisdom teeth out. My occlusion seemed good, until I protracted. My question…you may be the only in the world would may understand what the years of protraction may have done, especially while still developing and how can I tried the TMJ. I can deal with all of it except chronic pain. I have other health issues and it’s moving to the point where I wouldn’t hurt myself but I think how nice it would be for an end to the suffering.
In a situation like this, what could one do? Dentist gave a splint, physio has me working neck and shoulders.
The protraction doesn’t do anything as long as you started it after developing age. I started protracting at 12, and I have kept my jaw forward since then. I can easily keep my jaw closed for a month if I want, without developing any symptoms. Thus, several questions arise here:
* How developed was your jaw at the age of initiated protraction
* Are there any other predisposing factors involved such as anxiety disorder, OCD, very bad neck posture or history of head neck injury
* When you went back to non-protracted habit, did you start clenching the suprahyoids?
* Is the mandible opening and closing properly?
* Wisdom teeth pulled?
* Other important dental work preceding these events?
If you’re doing nothing wrong, then it could be that your teeth and maxilla developed poorly and that this is causing your problem. But, honestly, I doubt it. You clearly have Costen’s syndrome. Now, more likely is the notion that you’re clenching the suprahyoids or something of similar nature.
I am replying with such detail for yourself and other readers to learn that it’s not “that simple”. You’d have to book a session if you want case-specific advice; this isn’t something I can go back and forth on here on the forum.
Hi Dr Larsen, thank you so much for this detailed guide. I have found the correct posture for my jaw by protracting it forward. I usually have an overbite but protracting my jaw in this way leaves me with an underbite, and I also cannot smile or speak while in this position or I look completely unnatural and slightly unnerving. I was wondering whether this improves over time or whether this is an indicator of another postural problem. Thank you again for this wealth of great advice, much appreciated
If you had an overbite and now, have un underbite, you’re likely overprotracting. The feeling of the correction being “natural”, yes, this is just a matter of time if you’re doing it correctly. Now, clearly, I wouldn’t know if you are or aren’t.
Hello Dr. Been dealing with tmj issues for 7 years. Thankfully no pain. Jaw clicks 50% of the time I open my mouth. Left and right jaw. It all started when i hear a loud crack in my right jaw when I opened my mouth to eat. When I retract and protract and move my jaw left and right I’ll hear clicks and pops in my jaw. Again, no pain. I can open 3 fingers wide. Jaw muscles feel tight often. What seems to help over the last 7 years is when I manually push my mandible left and right with my thumbs. When I do this I’ll hear a click/pop in my joints. No pain. This kind of relaxes my face and makes opening wide even easier and seems to stop the clicking of the jaw temporarily. I have a normal bite. If I had to live the rest of my life how I have in the past 7 years, I would be fine. Im just terrified of it potentially getting worse in the future. Im only 26 years old.
What would you recommend for me Dr? To follow everything you mentioned in the article? Or are there certain things you don’t recommmed?
Thank you so much again, god bless you
Hello,
First thank you so much for this article, this is amazing!
Are we supposed to protract during sleep too? Since that seems really hard to do.
I was wearing an (anterior repositioning) splint at night that would push the jaw forward, and it helped with mouth opening first, but then it was causing a lot of muscle pain and spasm in the head so I stopped it. I was also told to stop wearing it by my new doctor because I no longer have disc displacement and wearing it now would only put more tension on tmj.
If that’s true, is there any other option beside a splint to protract the jaw at night?
Many thanks,
Fjori
Hi Dr Larsen, do you have any recommendation on how to stop clenching? I only clench at night and I can tell it makes my tmj pain worse when I clench a lot. I have tried most recommendations I see online, i exercise regularly too. I have also tried Botox which helped a bit but it gave me pain at the joints and I have heard it’s not recommended if you have issues with the joint.
Just wanted to check if you have additional insight here, because resolving clenching will play big part to fixing tmj. Would be happy to schedule Skype session too.
Read my article on clenching
Wow that was mind blowing, thank you! I have pain in my forearm too, now wondering how many of my issues are related 😓
Do you have any type of exercise you recommend in particular?
Also if it helps your patients, I have realized that I breath with my chest and that can be a contributor. I have started to learn how to breath with my diaphragm and seeing slight improvement already.
Thank you for this article, it is appearing to be life changing for me. I’m 38 and have been suffering with TMD for decades, rarely painful which has made me neglect treatment at times, but constant left ear pressure that never equalized. Over the last couple years, I’ve developed tinnitus and a creaky jaw. The last straw was pressure below the temple so I had to find something to reduce the discomfort. Moving the mandible forward almost immediately relieved the temple pressure, though I still think I’m clenching my jaw at times. Oddly enough, a lymph node in my neck that has always been a bit large swelled after starting this and I felt a bit unbalanced for a day (sort of scary to be honest). However, after a week of practice, the swelling greatly reduced to a point where it’s smaller than it’s been in years and the area behind my left jaw that has been inflamed for decades is also much, much smaller than it has been in basically my whole adult life. Additionally, the pressure disequilibrium in my Eustachian tube is basically none existent. The temple pressure comes and goes but again, I sort of feel like I need to relax my jaw still. It’s a work in progress but I finally have some hope now!
When swallowing with the new mandibular position (protracted out about 2-4mm), am I correct to assume the mandible must remain in the new position throughout the whole swallow without falling back? I wanted to make sure of this because of the new popping I’m experiencing when I hold the mandible in its new position. I love the article by the way!
This is a rabbit hole question that will just confuse readers more if I was to answer with all the details. The short answer is that it doesn’t really matter.
Someone posted this article on Reddit/TMJ quite a while ago. I saved it, but didn’t have time to read it at that moment. I wish I had. I had what I call “suicide jaw”… where I wake up to severe jaw pain, and it was so disheartening. Sleeping is supposed to refresh us – for me, it was just hell because my jaw was all over the place. I came across this article again and took the time to read it, and started protracting my jaw, and using the nnnnn sound to place my tongue in the correct position (it’s easy to overdo the mewing- I have -it’s painful). My pain was gone in less than a day, and is still gone- (I still have some cracking when I open my mouth wide). I thought the pain would return at night when I was unable to consciously protract my jaw, but it doesn’t. I can’t begin to thank you enough for this information – I will share it with anyone who needs it. I also have screaming tinnitus, and I need to look up the article you reference about that – I would love a link if there is one. Thank you thank you thank you!!
Great job, well done. If you get some relapse due to night grinding then get a night splint that advances the lower jaw.
Make sure to eliminate any suprahyoid clenching problems as well.
Is it possible to heal the disc if it is too far anteriorly displaced? I think I have been rubbing bone on bone on my right side for a while now and heard the disc will only get more displaced. Should I still do this protocol or just wait and hope pseudo-disc forms or pain goes away?
That’s what I would do. I think there’s a fair chance of tissue recovery as far as the retrodiscal tissue isn’t perforated severely
I should have mentioned that I have braces on and my orthodontist assured me that once he fixes my open bite (which will upswing my lower jaw slightly) then my TMJ pain will be easily manageable.
I had dental surgery and I suffered for 4 years. Now 25 years later, it’s bad again. MRI shows crumbled disk. Cant wear dental splints. Can this help?
This is an amazing in-depth article. I started getting tmj issues 2 years ago and i stumbled across your article back then. I tried your jaw protraction recommendation and noticed immediate improvements. But that was it, it gave me some improvements but it never cured my tmj symptoms.
2 years later i stumble upon this article again and noticed that in addition to recommending jaw protraction you also recommend fixing overall body posture. I took a week off from work and literally just spent the entire day standing and walking (just tried to stay away from my computer which forces hunch posture), and im pretty much cured of all tmj issues. I dont even have to protract my jaw anymore, i just have to focus on fixing my hunch back posture and my tmj issues comepletely dissappear.
Thank you for this information. I just have a couple questions:
1.) After practicing protuding my mandible long enough, should I no longer need to think about doing it consciously?
2.)While protruding my mandible, should my lower teeth extend past my top teeth or no?
Thank you,
Alex
1. yes but how long this takes will be extremely individual
2. depends on starting position. It’s an invalid question. 3-4mm is my recommendation as clearly stated in the article
Thank you for your insight. I’ve always thiught you were the best when it comes to correcting pain. This is the first time seeing this article. I have had debilitating tmjd for the past 4 years. I have tried everything. The only things that have helped me are chiropractor, correcring my posture, myofunctional therapy, a tongue tie release and a palette expander appliance that advances my lower jaw forward. Despite all of this I still am not near cured. I’d say my symptoms are 50% better but still have a lot of pain and dizziness and panic/anxiety when my jaw and neck tighten up. Am I missing something? I will try the exact exercises you recommend as they are new to me and weren’t introduced in myofunctional therapy. Thanks for your work you have an amazing understanding of the human body.
Hello , my symptoms decreased a lot , i want to thank you a lot , if i continue will it heal completely or it’sonly be a temporary relief ?
If you follow the protocol properly, it won’t come back unless you go back to old habits
This is a great article that seems to clear alot of things for me personally, and its very interesting how this stacks with overall postural problems. I have been trying to follow the advice you gave, but am noticing that when maintaining both the suggested tongue and mandible posture, that my jaw starts to feel tired/fatigued in a manner that I cant seem to rest. Also I feel like I am producing excess saliva and I notice a occasional tingling sensation around my jaw. Is this a normal part of the process or am I perhaps irritating a nerve somehow?
Careful with tongue posture in the beginning. Implement that AFTER you’ve held your jaw forward long enough for it to be easy. If your pterygoids aren’t recovering, take some breaks.
Thank you for this. I kept returning to this site until it clicked for me. For anyone not getting it, you have to unclench, not hinge at the neck, and protract (check the articles & videos here on all 3 of these things). If you just protract your jaw ignoring what he says here about posture, it won’t work. This requires a lot of awareness at first, but it’s way simpler and cheaper than what most specialists out there will tell you. Plus, it addresses the cause, not just the symptoms. I’m very thankful for the relief and improved mobility. Thanks so much!
I have been wearing essix retainers which I feel create a slight right posterior open bite when I wear them. I recently noticed I have right posterior open bite all the time, along with a right pterygoid tight/spasm, but no issues opening/closing the jaw. When I sleep without the retainers, I wake with a relaxed right pterygoid and a completely closed bite, but what feels like a right slipped disc that restricts opening (can maneuver around it) and “clunks” on closing. How can I get and keep the disc in place for unrestricted opening and also relaxing the pterygoid and closing my bite? Right now it’s one or the other. (I am of course applying your recommendations, and only wearing the retainers when I will not occlude on them.)
I have been trying to protract my jaw for a couple days now. My only symptoms were headaches and ear fullness. The headaches are gone, but still feel weird in the ears. Is protracting the jaw supposed to feel this strange? When I let it go back to my base line, the muscles in my jaw and ears feel very strange. Thank you!
Give it some time. Good thing pain is already gone.
Thank you for your article. I echo many when I say that your protocol of moving the lower jaw forward has offered tremendous reduction in my jaw pain immediately and since I encountered the info. just 48 hours ago. I wonder if you recommend any doctors local to the US who understand TMD in the same way that you do? I have undergone countless treatments as well as 2 major surgeries without any reduction in pain for nearly 5 years.
Hello,
Will this work aswell if I am 90% sure that my TMJ / bruxism is caused by exessive chewing gum?
A couple years ago I really got into mewing and looksmaxxing, where they recommend to constantly chew gum. I think this may have when my teeth grinding started at night, and since then it has never gone away.
I am trying recently to do facial stretches before bed but I’m wondering if this article may help my case aswell?
Thank you.
I finally think I have some hope. I’m 32 and ever since I can remember I’ve had problems with my jaw. It feels out of place, loose, have difficulty speaking, chewing, breathing or even laughing. I’ve been following your advice since the last 10 days. Some days I feel like it’s improving, some days I feel it’s doing nothing and feels very weird. I still cannot keep it protracted while speaking. Sleeping is a totally different story where it feels like I undid all the progress I might have made yesterday. Am I doing something wrong or is it just the normal healing process?
Hi, i have 6 months of everyday pain and headaches. and i think my disc is misaligned on one side when my mouth is closed. And whenever i open mouth or push jaw forward i hear pop sound, as if it “takes right position into disk”. Should i always keep my jaw forward in order to push disk back?
After one day of keeping my jaw forward i have feeling that this disk is slowly moves back. But im too scared to continue, because it starts to feel like something it stretching there when im trying to keep jaw in disc position.
This may be a little unrelated but What muscles would need work after a orbital and zygomatic trauma fracture
I am SO glad I have found this information. Thank you so much for this.
I am 38 years old and have been struggling with this since I was at least 16. Everything you have said here perfectly explains what I’ve been dealing with. My daughter, who is 14, is now beginning to have this issue. I have been so concerned about what to do to help her and prevent her issue from getting worse, and have feared a dentist might make her condition worse as well. I can’t wait to show her this info and allow her to begin to fix her issue while she’s still young!
Also, I saw that you mentioned that the teeth touching is not essential when moving the jaw forward. Is there any spacer like device that can rest between the upper and lower back teeth to make this position a little more comfortable?
Thanks so much!
As someone that works on TMD Im trying to get a more complete understanding of the dysfunction so as to have a greater understanding of the rationale for intervention. I dont do well when there is a disconnect between the two. I had a recent CE class that spent a lot of time and focus on the changes in superior head of lateral pterygoid (contracture, shortness etc) as found on MRI in cases of TMD. It was his take that the lateral pterygoid shortness was perpetuating an anteriority of the disc causing the displacement on closing and recapture on opening. It seems to me your take is more one of posteriority of the condyle in the fossa rather than anteriority of the disc. Im guessing it is a combination of the two in lots of cases. Ultimately… is it your take that lengthening retractors (temporalis and portions of masseter) is more important than lengthening/relaxing of lateral pterygoid as far as soft tissue work would be concerned or is none of that useful ultimately and it purely is a matter of retraining movement and resting posture and the muscles will remodel themselves accordingly with time? Thanks for your work! Ive also been spending a lot of time digesting your scapular dysfunction article. We learned early on the foundational importance of healthy scapular biomechanics but I think you have some unique insights and certainly a novel approach to correction…. so thank you!
Hi, I have a disk displacement with reduction and I’ve managed to keep the mandible forward and it seems that this keeps the jaw onto the disc. However, this has slightly altered my bite. However, If I bite with my jaw too far back, it causes the jaw to slip off the disc sometimes. Could this new forward position permanently change my bite? Should I continue to slightly protrude my jaw and train myself to bite more forward than usual? Could this not create issues with my teeth? Now, my top front teeth and lower front teeth slightly touch, whereas there used to be a significant gap. Could this new alignment cause dental problems like teeth wear?
I’m just a regular non-scientific person trying to understand this for my own ear / jaw pain. Is this the right way to translate this into plain human language? Sorry I have a hard time with all the jargon in this article!
Posturally protract your mandible 2-4 millimeters from maximal retraction (most important). Sometimes more than 4 mm will be required.
Find the position where your jaw is sitting as far back as it tends to go, then gently let it rest a few millimeters forward from that position — without clenching or forcing it?
Mr Larson I am conflicted in what I should do. I am nearly 16 and have had jaw clicking symptoms for a while, although without pain. Recently though this has changed and I have been having pain in the tmj area. This led me to you. After reading this article, I noticed that with full occlusion of molars, I am unable to move back much more. So I started to protract my jaw slightly, (Which in hindsight may have been a mistake considering my age) but in order for it to be enough distance, my bottom front teeth must be pretty much level with the top ones as I think my maxilla has recessed, along with a bit of tooth flare, much like another person said in the comments. They said they didn’t have any pain and so as they are still relatively young you suggested to just mew. I don’t know if I should continue protrusion as I am worried that the lack of occlusion this causes could be further detrimental to my facial growth as I am still relatively young. I’m aware that my jaw has had habitual retraction and that I have developed habitual forward head posture. I am aware that these probably caused my tmd. I will improve posture but as for my jaw position I don’t know what to do. Should I keep occlusion in mewing even though I feel it’s still too far back and hope I grow forward from the shearing forces over time or should I continue mandible protraction?
Thanks so much
First of all you say that you “recently” started holding your jaw forward, but I don’t find it logical that your teeth would start coming forward (this is not a result of mandibular protraction anyway, unless you push your lower incisors toward your upper incisors — I never recommended that), and see clear facial hypotrophy, in a short time; doubtful. However, on a general token: If you are a teenager or child and has TMD symptoms, it’s probably best to keep mouth shut on molars (you could protract a little if you’re under a lot of stress) and work simultaneously on ceasing jaw and suprahyoid clenching habits. Most TMD patients have underlying stress that’s causing them to clench.
Some mild Mewing whilst also avoiding clenching and lowering stress is probably the best approach for your specific case.
With best wishes I’ll tell you this: My general impression on your post is that you’re thinking too much. Find something else to spend your time and energy on; you don’t even have any pain.
I have had TMD without reduction for just over 3 years after an injury to it. But in the past 2 weeks- after a dentist checkup- I’ve been experiencing frequent low pain in the joint and actually in all areas of the jaw bone, but more often in the joint. It doesn’t get worse when opening so it’s not triggered by opening the jaw or chewing.
I wonder if you have any ideas about what might be going wrong with it?
Now the pain seems to happen in the left side of the jaw. The one without the slipped disc, it pops and sometimes hurts frequently atm the right side also hurts but not as much. I wonder what that indicates?
Oh also I forgot the most important point. It gets worse when I look down and open the mouth
Hi! I’ve been searching TMJD on the internet a lot, and I found your article very clear and profound, among a lot of rubbish you can find on web regarding this topic. Now I share with you my condition and if you will be so generous to read and give me any answer I will be very happy 🙂 I am a 18 years old boy. 3 months ago I noticed that I was often banging my teeth together in stressful situations (without, however, grinding them, just banging them hard without wanting) I made something very stupid and unnecessary, I know, and I will always hate myself for this; Thinking that my problem might be my slight overbite, and wanting to correct it I protracted my jaw to the maximum of my ability (but really to the maximum) and I clenched my teeth hard in that position trying to get as far up as I could until I covered my upper incisors with my lower incisors. Stupidly, I stayed in that position for like 5 minutes ignoring all the signals my body was sending me “please, stop!”; for some reason, i was upset with myself and I felt it like a training at the gym -kind of a challenge- “I do this set and I reach my limit!!!” without thinking I was venting my muscolar energy out of the normal TMJ ROM. To make it brief, when my muscles got too tired and my jaw abruptly went back to its usual position of slight overbite, I heard a loud “snap.” From that day, I have jaw clicking on both joints every time I close all my teeth togheter and re-opens my mount, or when I yawn widely. Sometimes (rarely) when i byte into something hard I hear a pop followed by grating sound that lasts few minutes during ALL MOVEMENTS, than disappears completely but scars me a lot. All these sounds produce zero pain, and have diminished with time, but I am really concerned that I have produced irreversible damage to some ligament or similar structure in such an idiot way and now my jaw won’t recover 100%.( I will do a MRI very soon). Now, I’ve never had jaw problems before, there are no functional/ ROM changes and my teeth fits togheter well and are healthy. Would you suggest me to protract slightly my jaw as you demonstrate in the article, iven if this is the “direction” that caused my “injury”, if injury we can call it, or simply relax and do nothing? Sorry for my English. Thank you so, so, so much
Hi there, when I protract more than 4mm, I get ringing in my ear and I have also got a stuffy left ear after doing this. Does this mean I am doing the exercise too far?
Either the trigeminal nerve is just recovering from the compression and it’ll go away by itself, or the pterygoids are overloaded from the protraction and you’ll have to go more gradual to ease the burden.
Thank you so much! I have TMD swelling around lower face. Can this take some time to go down? I have been doing this for 9 days. Pain is reducing!
How long can it take after doing the jaw protraction can I expect TMD swelling to go down? I have been doing this for 9 days. Thank you so much!
Hey I read this article after having 5 years of clicking and bad posture I decided to get the opinion of a maxillofacial surgeon and ortho who both are leaders in the TMD space in canada one of whom has 16 papers. They both said there is not enough evidence regarding tongue posture and they had never heard of suprahyoid clenching and told me I had health anxiety and that I shouldn’t do my research on google and only look at peer reviewed papers. Anyway based on their advice I was told to do manual therapy, muscle relaxants, mouth opening exercises keep in mind my posture was terrible and guess what now my tmj no longer clicks but I get a click on subluxation with less mouth opening I have cbct and mri that both seemed fine from their perspectives. My symptoms went from face pain -> breathing difficulty, snoring (new confirmed with partner), full body pain numbness, confusion, brain fog and frankly well I will be following this article however I think my neck and jaw is so dysfunctional its extremely difficult. Thanks for the content regardless.
Hi, Can you let me know the name of your doctor in Canada?
When I sleep, Should I sleep on my back or on the side? When i sleep on my back, my jaw falls backwards and is not protracted. When i sleep on the side, my jaw tilts to 1 side and my neck becomes tight.
Dr Larsen, thank you for the article I found it very useful. I have overbite and had braces for it, I feel popping and Locking of jaw when chewing on hard items, tension headaches and my lower jaw is retracted too backwards. Is this due to TMD? If I start mewing will it go away or is it a temporary solution? What should be done to protrude the mandible? I am in my early 20’s. Thanks
What are your thoughts on the SOMA (Splint Orthopedic Myofunctional Appliance) developed by Dr Joe Da Cruz for treating TMJ and cervical pain? Here is their website: https://wholisticdentistry.com.au/soma/
Hi, Is it okay with you if I print the article and keep it. Because I am fascinated with your explanations.
hey thanks so much for the article. i got a constant, dull and one-sided headache for nearly 2 years now. it sits exactly at the points you mentioned. no other “big” tmj problems besides that (except dizziness etc.). You think i have a good probability to get rid of the pain with your protocool? Thanks
Dr. Larsen, I cannot hear anymore, I have a constant terrible headache, I am very dizzy and unsteady most of the time. I have worn braces twice, once in my teens and once as an adult combined with splint therapy to hopefully alleviate the symptoms from the TMJ. I also used to get terrible vertigo 2 and 3 times a week before I had the TMJ treatment and braces. Splint therapy brought much of my hearing back and also made the headaches better but unfortunately I have lost almost all of my hearing and headaches are back since the conclusion of my treatment and not wearing a splint anymore. I live in Texas and it has been extremely hard to find a dentist who understands and will help me. I was hoping you might be aware of a doctor close to North Texas that understands the condition like you do, I have been fighting this for 20 years and I am so tired. Even if it’s another state it could be helpful, just as close to Texas as possible. I am no doctor but I can tell you all of the things you mention in your article are very real, many of which I experience. Thank you for the article and the time that you have dedicated to studying this, it is very terrible for some people.
Would any of your suggested treatment differ for a Skeletal class III underbite (previously ‘corrected’ with orthodontics but now with lower teeth drifting forwards) where protracting the jaw forward would cause premature contact of the front teeth. I’m in agony.
The concept will be the same; to distance the condyle from the glenoid cavity. Presuming your symptoms are mechanical. If they’re muscular then you’ll need to look at the pterygoid muscles.