
Chronic knee pain has a high prevalence in westernized societies, where osteoarthritis, ligamentous ruptures and meniscus injuries are on the top of the statistics. Scientists estimate that up to 25% of the adult population struggle with frequent knee pain (Jinks et al., 2002); every 4th adult person you’ll see on the street!
Could malcompressive, imbalanced forces within the knee, be the real culprit behind chronic knee pain? In our experience; yes, absolutelyt! This article will address the most common causes of these injuries, and how to identify and treat the underlying dysfunction.
This is a simplified version of my norwegian articles about knee pain.
The knee joint
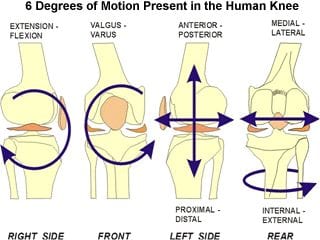
The knee joint is roughly made up of the femur (leg bone), patella (knee cap), tibia (shin bone) and fibula (calf bone) bones. Although the knee is mainly a hinge-type joint, it also performs gliding, rotation and side-bending to some degree.
At the end of the femur we have the inner and outer epicondyles, fitting into the meniscus’ articular surfaces. If muscular imbalances or postural/habitual strategies cause the femoral condyle to load the meniscus unevenly, wear and tear may occur much more rapidly than it would under normal circumstances.
Fig. 1
Joint misalignment
As I said, although the knee is a hinge-joint by nature, it’s also capable of certain degrees of gliding, rotation and rolling between the femur and tibia. Muscular and ligamentous tension sees to that no excessive movement occurs within the joint, especially when in a loaded position. When the knee is bent, there is a significantly higher degree of rotation available in the knee, than when straight.
Fig. 2
Problems ofte arise when the knee is habitually or posturally forced to stabilize in improper alignment, as an uneven loading foundation will increase the strain and friction on certain structures, whilst unloading others. The structures that become compromised, are often the ones under frequent excessive and unbalanced loading. The most common misalignments are, by most to least common occurrence:
- Tibia pulled too far back (posterior glide)
- Functional varus knee position (bent outward)
- Tibia too inwardly rotated
- Tibia pulled too far forward (anterior glide)
- Tibia too outwardly rotated
Tibial posterior glide
Posterior gliding of the tibia usually occur when the knees are being locked back into hyper extension in posture. This postural deviation is often a secondary compensation to swayback posture, which you can read about HERE.
When the knees are jammed backward, the hamstring can hyper activate to create posterior stability in the knee, so that they do not completely bend backward and rupture the PCL; it’s often a protective mechanism. Because of its attachments, the hamstring will then, over time, pull the tibia further and further backward, eventually causing excessive posterior tibial glide. This may be identified by palpating the transition between the femoral condyle and tibial plateau (the knee has to be straight and muscles relaxed), and you will feel a height difference (inward dent) when moving onto the tibia rather than a smooth straight transition between the two.
This backward pulling of the tibia will cause quadriceps and patellar tendon to stretch more than normal, thus greatly increasing the friction of the patella gliding over the femoral condyle when the knee is bending, which may wear down the condylar cartilage and cause tremendous pain “deep within the knee”, often referred to as “patellofemoral pain syndrome”. Additionally, the posterior cruciate ligament (which restricts posterior glide of the tibia or vice versa) will stretch more and more as the tibia malaligns, and may ultimately strain or rupture.
Fig. 3
![hyperextension[1]](https://mskneurology.com/wp-content/uploads/2016/01/hyperextension1.jpg)
Simplified, we could say that this is an issue of imbalances between the muscles that pull the tibia forward (quadriceps, gastrocnemius) and backward (hamstring). One way of dealing with it, could be to stretch the hamstrings and train the quadriceps and calves. I’d recommend, though, that the postural corrections are additionally utilized; primarily by correcting the swayback posture and locked-knees. To “unlock” the knees, simply open them by a quarter inch and avoid falling back into full extension. They should not be bent, just opened slightly.
Measure the rehab progress by repalpating the transition and seeing whether the difference between the two is closing in.
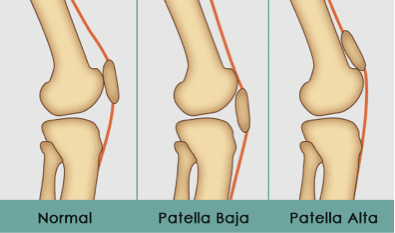
Patellar height
The height of the patella will affect how well and symmetrically it can glide in the patellofemoral groove (trochlear groove). Several factors affect this, such as tibial gliding and rotations, and muscular function. If the tibia translates posteriorly, the patella is pulled somewhat downward. If it’s translated anteriorly, the patella will come somewhat upward.
If the patella resides too far cranially, it may impinge the hoffa’s fat pad as the knee bends. When excessive, it may also cause it to rest outside of the groove, and thus resting onto the bone structures that isn’t covered with cartilage. This will, of course, greatly increase the risk of cartilaginous damage, and osteoarthritis. Guided by the evidence, it seems that there is much more trouble involved with patella alta, than patella baja, where the latter is only associated with schlatter’s lesions in a few studies. Genereally, there is little evidence regarding patella baja.
Fig. x
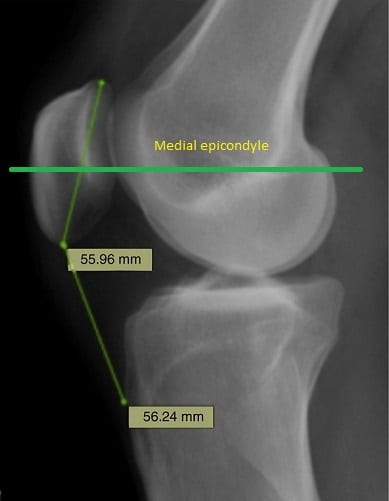
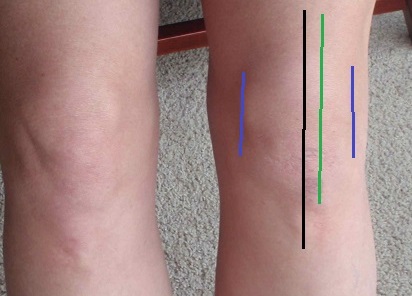
The medial femoral epicondyle’s prominence tends to be slightly higher than the lateral one. Furthermore, the lateral epicondyle tends to have two prominent tubercles rather than one, which makes the medial epicondyle a more reliable landmark for measurement. To identify patellar height, you may evaluate the distance between the center of the patella, and the palpable prominence of the medial femoral epicondyle. The center of the patella should be in line with, or perhaps just slightly above or below the medial epicondyle. If the central patellar imaginary line is way higher than the medial epicondyle, this indicates patellar alta.
If the patella resides too high, the tibia may be translated forward. In such case, posterior tibial gliding (which will be dealt with shortly) may help the patella to come down a little bit. If the tibia is not forward, or even backward, this is indicative of patellar tendon laxity. Prolotherapy will likely be the next best treatment strategy, along with identification and removal of any habits (such as a tendency to sit in the office with maximal knee bend all day, and similar). You may also want to find out whether or not the quadriceps is strong and tight, or weak and tight. If it’s weak and tight, it requires strengthening. If it’s strong and tight, stretch it. A muscle test along with palpative evaluation of the tissue may guide you to such an answer. If not, just try one of the above; it probably won’t make a huge difference anyway.
On the other hand, if there is patellar baja, releasing the patellar ligament along with strengthening of the rectus femoris and the rest of the quadriceps muscles may be beneficial. Also, if there is posterior glide of the tibia, the gastrocnemius may be strengthened as well, as therapeutic intervention.
Fig. x
Patellar alta is the most common, and sadly also most difficult scenario to treat, as we can not merely strengthen the tendon. Habitual correctives, simple strengthening exercises along with prolotherapy is most probably the viable route to go. It is important to mention, though, that even if a [very] cranially positioned patella is found, it may not be the cause of the pain. A full examination is necessary in order to include or exclude differential issues.
A higher position of the patella (patella alta) is also associated with HFP impingement. The impingement is typically observed during full flexion of the knee. – Draghi et al., 2016
The presence of a high patella in the group of athletes with chronic tendinopathy of the knee extensor mechanism was significantly higher than in the control group. – Garms et al., 2011
A high ISR, indicative of patella alta, is associated with structural features of OA in the PFJ. Additionally, the same knees have increased risk of worsening of these same features over time. – Stefanik et al., 2010
Patella alta was associated with the highest maximal patellofemoral contact force and contact pressure. When averaged across all flexion angles, a normal patellar position was associated with the lowest contact pressures. – Luyckx et al., 2009
Functional varus & tibial internal rotation
Functional knee varus is one of the utmost common causes of knee pain, in my experience. This strategy will place uneven loads upon the medial and lateral meniscus, where much greater loads will be imposed on the medial meniscus, and the lateral meniscus will somewhat unload.
Fig. 4
![oa3a[1]](https://mskneurology.com/wp-content/uploads/2016/01/oa3a1.jpg)
The most common cause of functional knee varus, is posterior pelvic tilt (PPT), which is one of the most misdiagnosed and unidentified postural abnormalities out there (learn how to deal with this in the same link as with swayback posture). PPT causes constant abduction and external rotation of the femur, which places continuous misloading onto the medial meniscus and locks the knee in maximal internal tibial rotation. Over time this may lead to injury of the medial meniscus, and even osteoarthritis. (Functional valgus, which is more rare, will cause the opposite; lateral meniscal injuries).
This can be a brutal combination in my experience, often causing chronic injuries and pain in the joint. The varus positioning of the knees will also cause shear forces between the lateral femoral epicondyle and the IT-band, and when this shearing becomes great enough, a so-called “adventitious bursae” may develop between the IT-band and femoral epicondyle in order to relieve the friction, causing chronic runner’s knee syndrome. In other words, solving functional knee varus will also resolve chronic runner’s knee syndrome.
Fig. 5 –Left side; optimal knee coronal alignment – Right side; functional varus-knee alignment

The rotation within the knee is relatively easy to measure, but the functional varus-position is often quite subtle and not easily identified (ref. figure 5). I usually ask the client if they feel that they are “pushing the knees” or “hanging/slouching the knees” outward in posture. They’ll need to think a bit, but often conclude that yes, they do. If the client’s knee is jammed in maximal internal rotation, they usually have functional varus knee posture as well, which is why these traits are within the same subheading.
The rotation between the femur and tibia is measured by comparing the position of the center of the patella, to the tibial tuberosity. The tibial tuberosity should NOT be lined up with the mid-patella; it should be approximately 25% more outwardly rotated. Figure 6 represents a typical “internally jammed” knee joint, where the tibial tuberosity is directly centered with the patella. Once again, it should be about 10 degrees more externally rotated, to line up vertically with the 3:4th lateral position of the patella (like this).
{kind=link}
Fig. 6

To fix this we firstly need to get the person out of posterior pelvic tilt. This alone will often cause immediate adduction and internal rotation of the femur, but it’s often a good idea to supplement with exercises for the muscles that furthers the reversal of the dysfunction.
- Tensor fascia latae – External tibial rotation, internal femoral rotation, knee valgus
- Peroneus longus – External tibial rotation, cooperates with TFL
- Adductors – Internal rotation of the femur, knee valgus
- Psoas – Adduction of femur in gait
Measure the rehab’s progress by checking the alignment between the tibial tuberosity and patella, pelvic alignment, and whether the person is able to utilize the TFL, adductors and peroneus longus during walking and other knee loading activities.
In training
Another common cause of knee varus, is pushing the knees too far out in the squat and similar exercises. A common misconception is that the knees should be pushed “torqued” as far out as possible. I see so many patients wreaking havoc on their knees due to this harmful cue!
The knee’s optimal position depend on the relation between foot and femur. It’s too big of a subject to address in detail in this article, but generally you’ll want to point the knee toward the #2nd toe if your foot is flat, and if you have a higher arch, you’ll want to point the kne toward your big toe.
Fig. 7 – The father of busted knees
![squat_stance[1]](https://mskneurology.com/wp-content/uploads/2016/01/squat_stance1.jpg)
Optimal knee tracking is MUCH more adducted than most people think! Here’s an illustration of how the knees and feet should be aligned in the squat. Figure 8 has pretty close to optimal knee positioning in the squat; the feet and femur are rotated in the same direction, with the knees pointing at the big toe. The only small detail is that the foot is too flat, but it’s the best illustration I could find.
Another fact is that excessive “pushing out” (varus) of the knees, will inhibit the adductors. Many do not know this, but the adductors are powerful hip extensors, and functional knee extensors (due to fixated tibia) in the squat, and thus act as synergists to the glutes and quads. This is why you see many of the asian weightlifting champions go into (excessive) knee valgus on the squat’s ascent (not recommended). Either way, proper knee alignment is a winning combo both with regards to injury prevention and to performance.
Fig. 8
By now everyone knows that allowing the knees to fall too far in, is detrimental. However, there seems to be no real consensus of what is truly neutral, in the exercise community! Hopefully this article will clear up some of the confusion.
Anterior tibial glide
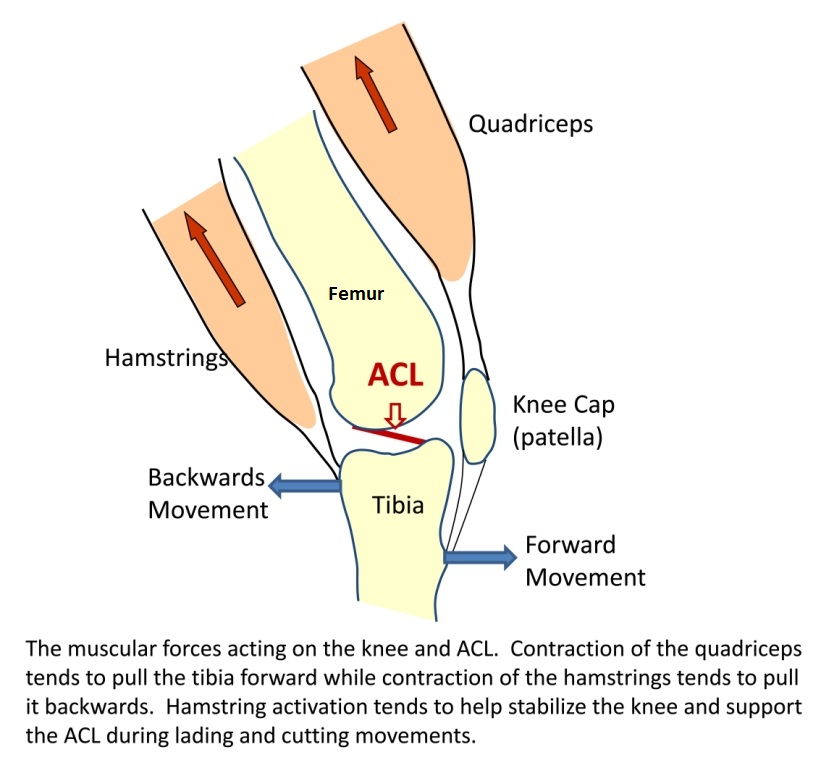
This is the real cause of jumper’s knee; a too anteriorly positioned tibial bone. The tibia can translate forward due to several reasons. The most common is hyperactivity of either the calves or quadriceps, which usually occur if the person if gripping (clenching) their calves or quads posturally/habitually. A weak popliteus will also allow the tibia to translate forward. It is usually weak because excessive foot pronation and medial femoral rotation occurs in posture and gait. Addressing both the causes and the symptoms (muscle weakness) is therefore often necessary.
When the tibia translates forward, it alters the angle of which the patellar tendon is pulled, often to such a degree that it may grind the patellar tendon into the tibial plateau as well as the infrapatellar bursa, causing constant wear and tear when the knee is bent. Secondly, it can strain the anterior cruciate ligament (ACL), which restricts anterior translation of the tibia. It simply can not do this, over time, if not being adequately helped by the hamstrings.
Fig. 9
To identify anterior tibial glide, similar to posterior glide, palpate the transition between the femoral condyle and the tibial plateau; it’ll feel prominent, and sticking out compared to the femur. The degree of translation varies, and is something you’ll need a bit of experience in to properly evaluate. It should, however, be a very smooth transition between the two; so any posterior or anterior glide means that there is room for improvement.
Correction is relatively simple. Stretch the quadriceps and gastrocnemius, train the hamstrings and popliteus muscles. There could be underlying reasons of hamstring inhibition, such as inadequate hip extension in gait, but this is once again too complicated for this article’s purpose. As with posterior glide, it will also be beneficial to stop clenching the quadriceps and/or calves in posture.
Excessive external tibial rotation
Now, this one is a little more rare. A too outwardly rotated tibia (or inwardly rotated femur) will cause faulty tracking of the patella in the patellar groove, causing it to grind into the lateral (outer) aspect of the condyle. This condition is often referred to as “chondromalacia patella”.
Once again, as seen in the illustration below, we use the center of the patella and tibial tuberosity as landmarks for measurement. If the tibial tuberosity is vertically in line with the lateral edge of the patella, or further than that, this is a positive indication for excessive lateral tibial rotation.
Fig. 10
![12191418_1651062028497842_2449019230007389414_n[1]](https://mskneurology.com/wp-content/uploads/2016/01/12191418_1651062028497842_2449019230007389414_n1.jpg)
This condition is often caused by a combination of flat feet, and/or weakness of the hip flexors or gluteal complex, causing tibial external rotation or femoral internal rotation to excessive degree. To correct it, it’s a good and simple start to train the muscles that oppose the dysfunction:
- Psoas – External femoral rotation
- Gluteus maximus – External femoral rotation
- Posterior gluteus medius – External femoral rotation
- Piriformis (and deep six) – External femoral rotation
- Tibialis posterior – Internal tibial rotation
- Popliteus – Internal tibial rotation
Once again, measure the rehab’s progress by using the landmarks of the knee. You’ll want the tibial tuberosity in line with the 3:4th lateral aspect of the patella (ref. illustration that was linked in the opposite subheading).
In conclusion
Knee pain is very common. Thankfully it’s possible to reverse the causes of the condition as well as the symptoms, in most cases, if one is able to identify and correct the imbalanced forces in and around the knee.
In my experience, the utmost common underlying causes of chronic knee pain, is posterior pelvic tilt and functional varus-position of the knees. These are both very subtle biomechanical factors that most of the time remain unidentified by the majority of therapists. I hope that this article has shed some light on these conditions and on how to treat them.
Summary:
- Functional varus causes malcompression of the medial meniscus
- Functional valgus causes malcompression of the lateral meniscus (not so common)
- Posterior tibial glide causes patellofemoral pain syndrome
- Anterior tibial glide causes jumper’s knee
- Excessive external tibial (internal femoral) rotation cause chondromalacia patella
- Maximal internal rotation of the knee, will jam it up and increase shear forces onto the meniscus
- Stop pushing your knees too far out. Rather, point them toward the big toe. Unless your foot is extremely flat, then point it to the second toe.
Most interesting
Most interesting
Hello Kjetil. I love your work in trying to correct misconceptions about posture. It seems I have postural varus as you said in this article. My fibular head stick out A LOT. I can easily see that my knee is usually in a varus position like figure 4. I think that I have a overactive hamstring tendon that pulls my fibular head laterally. What would be a specific movemnt I could do to best get my pelvis out of a posterior pelvic tilt. Thanks
Relax hammies, slight increased low back arch, weight on mid foot, strengthen TFL and peroneals.
I’m confused with the fact that a externally rotated femur would cause misloading on the Medial side of the knee. If true, then why would functional varus position be associated with medial meniscus pain? Wouldn’t a force on the medial side cause a potential tear on the lateral side due to the amount of stretch on the LCL? Thanks.
Lateral femoral rotation induces varus and medial femoral rotation induces valgus. Valgus loads lateral meniscus and varus loads medial meniscus.
I have an issue where my knees seems to be stuck if I sit at my desk with my right knee bent and foot flat on the floor. When I get up there is a “pop or stretch” and sharp pain but then is fine afterwards. If I sit with my leg extended out, it doesn’t do this….what are your thoughts?
Most likely either cartilage damage or meniscus tear.
I have right knee alignment problem. Knee very painful unable to bend fully pain is chronic if catches when bending and centred on medial side of knee just off centre when bent. What exercises do you recommend to maintain power and strength. I’m waiting to have MRI
Depends on the diagnosis. It’s probably either a cartilage defect or medial meniscus injury.
Hello,
I just stumbled across this article and realize how incredible this break down is. Its extremely easy to understand. I am curious though. As anyone who has came to this page is due to some sort of knee pain. For myself my knee randomly begins to hurt as an uncomfortable pain. My knee feels like its not aligned properly. Only when I’m standing it has weight on it. Now when it feels like this, if I sit down and relax my leg and press on the skin below my knee cap I feel that same pain. I believe I got this pain about 2 years ago when I was doing leg press, I was doing a lot of weight and my knee began to bend inward slight as I was pushing out. Do you have any ideas to as of what this could be or whom I should see?
Book a skype consult and provide me with a knee MRI
Kjetil, I’ve had right lateral knee pain for a couple years which started getting worse earlier this year. No one has been able to diagnose and I’ve had 2 negative mri’s. I’ve noticed when I walk my left foot points straight but upon landing my right foot it points to the right. When I bike both feet get locked in straight by the straps, it doesn’t hurt when I bike but when I get off and start walking it is very uncomfortable. Could my feet or hip alignment be causing my lateral knee pain? I would really love to get your input.
hello
Mr. Doctor, I’m sorry to bother you. I have a few problems. Thank you for your answer.
1 When I walk, my buttocks rotate a lot, that is, it goes too far to the right and left or up and down, and I am a man. I am 20 years old. What could be the problem? Are my buttock muscles weak?
……………………..
I think my knees are braced. When I go, my knees bend. What could be the reason?
Sounds like you have hip impingement
Great article – I am a runner in Australia who collapses mediallly at times and is experiencing medial knee pain. No swelling or end range knee flexion extension stiffness. MRI states typical runners knee however measurements appear normal as is HHD strength . pelvic alignment appears normal during 2D gait. could /hamstring tension be generating the issue?. Quad and hamstring rehab (SL) + 4 weeks has resulted In subtle changes. Re Varus loading relating to excessive lateral femoral rotation – Would you recommend strengthening IR of the hip, keeping length to hamstrings and improving peroneal strength?
If medial joint line test is positive, train the TFL and peroneals. Don’t do the adductors. If MJL test negative, consider saphenous neuralgia, in which you’ll have to strengthen the psoas.
You wrote that the tibial tuberosity should be in the 3/4 part of the lateral patella. Thats the case for me when the leg is extended and relaxed. When I tense my quadriceps the patella moves laterally, about 1cm, and then is centred with the tuberosity. Is that normal or should it ideally stay in its position? Is it due to quadriceps inbalance? I have anterior knee pain and the patella is grinding. My doctor told me it’s because of patellar dysplasia, but I think theres another cause. I also have slightly pes valgus.
You write laterally, but I assume that you mean that the patella tracks medially when you tense the quad. Try to strengthen the TFL and peroneus muscles. Avoid “falling out” excessively with your knees when walking.
Thanks for your answer. No I mean it tracks laterally/outwards. Any idea? Or is it normal that it comes in line with the tibial tuberosity when tensed or flexed?
Hello I am recovering from right tibia plateau fracture. I recovered at home . In PT now but my knee is locked. I’m at 90 now but my knee is constantly swollen. Is there a brace that can help with alignment. I’m in Drytex hinged knee pop but it pushed it out of alignment. Thanks for your help.
Needs imaging
Hello Kjetil,
I am having knee pain most of the time. My fibula looks like it is out of alignment and when I walk I feel by bones grinding. I had surgery to remove the cartilage about 35 years ago. Any suggestions on exercise that might strengthen or realign my knee?
Read the article, I can’t help you with such a vague description. My apologies.
Dr. Kjetil,
A truly informative article.
In 2013 I had a hip replacement which failed and was replaced in 2018. A glutus maximus transfer was done but did not hold. This has left me with a trendelenburg limp. I think this has caused a mis-alignment of both knees causing swelling and mild pain. I walk a mile or more every two to three days with the use of a cane. Afterwards the knees are sore. I sit on a bench and swing the knees back and forth with ease but this does not seem to offer improvement. It is difficult to walk up and down stairs as the muscles are weak. Is there a fix for this?
Respectfully,
Frank Smulders
Sir
As seen in this article, the corrections needed, will depend on the clinical examination and your symptoms. Unfortunately, your description is too unspecific for me to be able to advise.
This is the first and (at least according to my brief internet research) only source that discusses the problem of knee varus in a meaningful way. I’ve been looking for a solution to my knee problem for years and my symptomatology fits perfectly. Pain in the medial knee area, weakened medial musculature and chronically hardened latereal structures. This leads to a patellar click in the latereal area when the knee is extended (thank god not painful but 10/10 annoying). I had knievalgus as a child and obviously overcompensated.
Do you need an MRI for a skype appointment or is it possible without? By the way, I am happy about further literature recommendations (I found your recommendation Dr Even Osar amazing. Unfortunately he does not treat knee varus in his book)
Best regards
Hi, thanks. The knee alignment material is my own; there is not any published work on it as far as I know. Maybe some in the orthopaedic literature. I might publish it eventually but my research interest is not mainly in MSK, as the MSK research is full of nonsense.
Hi Kjetil! Do you have to do the measurements (tibia vs femur // patella VS tibial tuberosity // patella VS medial femoral condyle) when the patient is in supine position (and in this position flexed or extended knee?) or upright? Thank you.
Transverse plane measurements are best done standing.
For longitudinal plane measurements, have them clench the quadriceps
Very good article.Can u suggest some book on biomechanical explanation of pain?
Thanks buddy. Not really
Hi Kjetil, Great article. I have had lower back pain on my right side for 6 years and had various treatments, injections, hip scope but still as bad as ever. I’m convinced its an alignment issue and reading this i can say that both of my knees turn in (more so on the right side) and my Tibia points straight down. It affects my whole right side from my knee to my right elbow and is at worst first thing in the morning when i would barely be able to arch my back. It loosing’s up during the day after alot of stretching but its the same again the next morning. Is there any treatment, exercises or anything you can suggest to help me with this. Thanks
Hi, I suggest that you read my low back article, or consider booking a skype consult
Hello, Thank you for this really interesting article. I was diagnosed with hip and knee osteoarthritis earlier this year but feel there are underlying problems that should be looked into for full diagnosis and effective treatment. My hope is that you may be able to tell me what type of referrals and examinations to discuss with my doctor. In brief; retired female, flatfooted all my life, wear insoles, recognise myself in your picture and description of someone with a posterior pelvic tilt. Acute lower back problem in 2014, with severe pain going down leg; said to have a slipped disc but no imaging done to confirm this diagnosis. Sudden onset of sharp pain in left thigh earlier this year, developed into knee pain in same leg, with pain on walking, sitting and standing. X-rays showed some osteoarthritis of hips and knees and ‘grade 1 spondylolisthesis present L4 on L5 with intervertebral disc space narrowing and endplate sclerosis at same level’. Requested MRI scan not felt to be necessary, only offered pain relief, possible cortison injections and possible future hip/knee operations/replacements. Continued and variable pain despite following exercise regime for osteoarthritis. Right leg starting to bow, right foot points outwards with knee over or outside of big toe. Severe knee in left knee, 2nd bump below patella on that leg (patella alta, camelback sign?). Pain in left hip region, also lower back pain. I would be so grateful for advice on what to say to my GP.
Additional comment to previous message: Forgot to mention that there is also over pronation of the feet, painful left foot, bunion developing and diagnosis of osteoarthritis in left big toe (hallux rigidus) . Apart from the above and osteopenia there are no major health issues and under average weight.
Hi Kjetil, thanks very much for the article. Very informative as always. I was wondering, since some of us (probably most of us in fact) don’t have good palpation skills, what kind of tests/scans would you recommend we obtain before booking an appointment with you?
For knee pain? Just an MRI
Thanks again. You are amazing.
Should the indent/prominence of the tibial plateau be equal on the medial and lateral side as long as the knee is not in varus/valgus position?
Wow you are great answering all these questions, I admire you. I have anterior pelvic tilt, chondromalacia patella to the right knee, though my pain is in the left by the Hoffa Fat Pad this can get puffy,(MRI to the left shows NAD). I also have tibial varum & hallux limitus. A podiatrist said my arches are fine. I enjoy running, cycling & swimming. Running I feel like I am wonky & experience left knee pain, lumbar & right hip tightness, & left foot doesn’t feel comfortable. Also have numbness & tingling in both feet after running 3miles, which goes after another 3miles, trainers are nice & wide (Altra, zero drop). Cycling I feel happy with right leg but left leg I don’t pedal the same, the foot naturally goes heel inwards but I fight it & push it outwards to stop my knee hurting, very odd, it’s like the foot wants a medial post (varus) but a forefoot lateral post (valgus). Trying a reverse Morton’s at the moment for the hallux limitus. Also I have no marked leg length discrepancy. Swimming causes pain in the left Hoffa pad when kicking off the wall.
Hey Kjetil, during football game my foot slipped and my knee bent excessive laterally or medially (varus/valgus) (I cannot remember cause this happened too quickly). Now i don’t have really a pain but knee is really unstable. I can’t extend fully my knee cause i feel that knee will slip out to a side if I wouldn’t pay attention to it. I suspect that ligaments are lax and it takes time to heal. What muscles should I rehab/train? Hamstrings, calves and popliteus? Thanks.
Need a proper exam. Go see an orthopaedic doctor who is a great knee surgeon. You’re likely looking at surgery here.
Hi Kjetil, my 11 yo daughter has a leg length discrepancy causing a whole lot of issues. She’s a competitive gymnasts so we are constantly dealing with injuries. Her left tibia is 3/4″ shorter than her right side. Femurs are equal. Her left hip is tilted down. She is going to have eight plate surgery to help correct the difference. My question is about her bad posture and if it can be corrected. She has developed knee flexion over the last few years where she can’t fully straighten her knees. Her shins are slightly forward over her ankles, knees slightly bent, hips tilted forward, lower back slightly arched, shoulders slightly forward. With all the training she does you’d think she would have better posture. I’m worried her bones are growing out of alignment (specifically femur and hips). Is there some physical therapy she could do to get back in alignment to straighten her legs?
She won’t be able to straighten if there’s a length discrepancy. That said, most patients can live with minor discrepancies in length without any problems. We would have to talk more specifically about her injuries rather than blaming generics, in my experience.
Hi Kjetil,
Recently my left knee feels pain when I hyperextension a bit of my left knee, my right knee is fine. When I stand, I tried to contract my quad muscle, I can see my right leg is able to do the contraction, but my left cannot. When I sit on the floor and extend my legs, I tried to internal rotate my legs, I feel pain on my left knee and feel locked. I don’t what structure on my left knee is the issue. Is MRI can help to identify the problem?
hello…. i.m from london and have never done anything more aggressive that a daily 1hr walk. with some resting…..
the problem is with my r knee. its currently swollen (3rd month now) and had a second dvt in calf in sep22 its ok now…. (xaretto 10mg daily)… 1st was also a 2 week hospitalised pe in 2013……
fast walking brought on warmth to touch while slow walking reduced the warmth. the dvt is in my popliteus vein and i am having a problem distinguishing between it and misallignment due to my r foot being flatter than left foot…. i appreciate that it gets complicated but….. can you help ? surely its not a big deal like meniscus or tendon or ligament ? ps podiatrist insoles helped now but returned to normal sneakers today ( pain upon walking up and down stairs)
in the last 2 weeks i never allowed my r foot to bear weight while walking up… and always r foot first walking down…. so keeping load on left foot only ha ha so it takes ages… twice as long actually….. things have improved because no more warmth…. but i await the outcome….. could you point me in the right direction please, the nhs is quite useless……
Hello, thank you for all your articles. Do you think there is a big connection between varicose veins and bad walk or posture?
No
big thanks!
Even with low bar squatting the legs should not be too far apart right? Like farther than shoulder width? The knees should not be too far regardless of high bar or low bar. Also, is a sumo stance safe with squatting or deadlifting? I know you warn about legs being too wide.
Depends on femoral angle. 1. align feet roughtly to where knees are pointing. 2. fine-adjust knees towards big toe or 2nd toe
Thanks. Is a sumo stance deadlift a safe exercise? I would think yes.