
So many of our clients struggle with chronic shoulder pain. A study conducted by Luime et al., (2007) estimated that between 60-70% of the population will at some point struggle with shoulder pain. Why is this specific problem, often so difficult to resolve? Why do some get complete resolution of symptoms by utilizing simple rotator cuff exercises, whilst others have no effect at all?
Naturally, it depends on the true cause of the injury. So, let’s talk about the most common dysfunctional traits with regards to shoulder impingement syndrome.
This is a simplified version of my other shoulder/scapular articles in norwegian.
The triggers of shoulder impingement
In my experience, there are a few criterias that seperate healthy and unhealthy shoulders.
- Scapular resting position
- Scapular movement in humeral abduction and flexion
- Rotator cuff strength
The most common things I see in the clinic, is that the scapula has a too depressed (low) resting position. This causes a cascade of issues, such as inhibition of the scapular movers and stabilizers. As a result, the scapula will no longer move properly during loading, either. Which in turn may dramatically reduce the stimulus and function of the rotator cuff.
It is absolutely necessary to understand that these issues are rooted in motor control dysfunction, and not muscular strength deficiencies (Osar, 2012). Resolving these three points have, at the time of writing, resolved almost 100% of our clients’ shoulder pain, be it chronic or acute. It really works, when done right.
Scapular resting position
It is critical that the scapular resting position is optimal, especially for athletes. Why? Because proper scapular resting position means that the muscles that should hold and move the scapula, are active in posture! Ask yourself this: Why would they magically work during heavy loading, if they do not even activate in unloaded posture? They won’t! It thus makes the proper foundation for the scapula and its movement.
Fig. 1

The scapula should, in standing posture, be held between the T2 and T7 vertebrae (Sahrmann, 2002). It’s simple to measure, just run the finger down the neck of the person examined until you palpate the first prominent spinous process, which is the C7. From there, count two steps down, to the T2. Then measure the position between T2 and the superior angle of the scapula. This is a simple way to determine, for the untrained eye, whether the scapula is too depressed to too high.
Fig. 2

Most shoulder patients have a scapula too low, in my experience! It’s simple to correct, by simply raising it to the proper height and staying there. It is in reality a postural awareness issue, and has to be fixed by changing into good habits. Strengthening alone will NEVER cure malpositioning of the scapula! The trapezius muscle should be palpably active in posture, holding the scapula in proper position. Below we see a prime example of how postural/habitual depression of the scapula causes winging, faulty movement (and a super common cause of chronic neck pain, aswell!).
Fig. 3

If the scapula is too high, which is rare, it’s usually an imbalance between the muscles that elevate and depress it, that’s the problem. In this case, a corrective exercise protocol can be very beneficial. I.e stretching the upper trap or levator scapulae, and training the serratus anterior and lats.
Scapular movement
When the resting position is addressed, establishing proper scapular movement is the next critical, and sometimes most difficult step to correct. It’s very important to understand how the scapula should move during movement and when loaded! The scapula actually makes up 1:3 (30%!) of the shoulder joint’s movement capability, by rotating the glenoid cavity in the same direction as the arm.
- When the arm raises forward, the scapula should posteriorly tilt (tilt backward). Straight raising of the arm thus involves 120º of humeral flexion and 60º of scapular posterior tilt = 180º total ROM
- When the arm abducts, the scapula should upwardly rotate (AC joint raises and moves toward the head). Straight abduction of the arm involves 120º of humeral abduction and 60º of scapular upward rotation.
- Eccentrically, the scapula must not collapse into depression, anterior tilt or downward rotation, as this will also cause impingement. More examples of this in my video library.
Briefly, nine of 11 studies reviewed demonstrated a statistically significant scapular movement deviation in at least 1 variable, as compared to healthy control groups. The most frequent findings have been reduced ST posterior tilting, reduced ST upward rotation, increased ST internal rotation – Ludewig & Braman et al,. 2011
Fig. 4

Figure 5 vaguely illustrates the difference between normal and abnormal abduction of the arm. I say vaguely, because it’s not just a glenohumeral muscle-activation problem, as illustrated below. This picture shows that when the middle deltoid fires up without coactivation of the supraspinatus, it will cause the humeral head to move upward and jam into the AC-joint, causing impingement.
The above statement is true, but it just covers a a small part of the problem. One could ask: “Why does the supraspinatus not activate?”. Is it simply a strength deficit? No. The supraspinatus will not activate as it should, if the scapula rotates downward (or stabilizes dysfunctionally). This causes both mechanical and motoric problems. When the scapula rotates in the opposite direction of the arm’s abduction, the humeral head will certainly jam into the acromion. Secondly, because the supraspinatus will not activate properly, the humeral head will be translating up and the joint thus jams up even more!
On the contrary, when the humeral head is held down by the rotator cuff as a coactivation by proper scapular articulation, impingement CAN NOT occur! It simply can not. And this is why following these principles lead to a very high success rate when done properly.
Fig. 5

So, what does proper and improper scapular movement look like in practice? It’s imperative to be able to assess and identify the scapular movement, if one is to correct the problem.
Below we have a typical impingement-case scenario. The person is, firstly, unable to maintain proper height of the scapula during loading, due to inhibition of the trapezius. This causes the cascade that has already been mentioned, where [all] the scapular stabilizes cease to fire up and do their job. As a result we see tremendous retraction, anterior tilt and downward rotation of the scapula, surely jamming up that AC-joint.
Fig. 6 – Scapular depression, downwardly rotates and anteriorly tilts when horizontally loaded

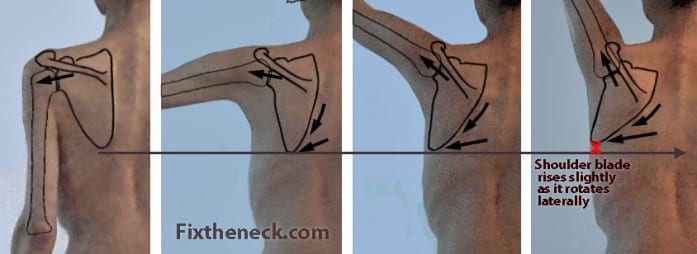
To address this, the person must first learn to maintain proper height (superior scapular angle : T2 vertebrae), during movement and loading. Secondly, when this is accomplished, the serratus anterior and lower trapezius must posteriorly tilt and upwardly rotate, as the humeral angle increases (arm raises higher). Again, this is motor-control training and not really strength training – But sure, the scapular stabilizers can positively be strengthened in a parallel manner, to supplement the ongoing motor control corrections. Figure 7 illustrates proper scapular movement during shoulder abduction.
Fig. 7
Finally, enjoy a real-time demonstration by my chunky self.
Scapular control in the overhead press
Scapular control in the pull-down
For the horizontal pull and press, the same principles apply; but with lesser degree of posterior and upward scapular rotation during the movement.
Rotator cuff strength
The rotator cuff is important, but not that important. It’s true, as you’ve seen, that it depresses the humeral head and therefore hinders impingement (superior translation of the humerus, in the glenoid cavity). However, these muscular forces – if they even do activate – can under no circumstances stop impingement if the scapula moves in opposite direction of the arm bone (humerus). That said, weakness of the rotator cuff is a real thing; it does matter and often has to be addressed. Especially for athletes, as the higher load imposed on the joint will require greater rotator cuff strength to be able to properly stabilize and centrate the humeral head in the socket.
There are four rotator cuff muscles.
- Subscapularis – Pulls humerus back, and down. Internal rotator.
- Infraspinatus & teres minor – Pulls humerus down. External rotators.
- Supraspinatus – Hinders superior humeral translation. Abductor.
Once again, more examples of rotator cuff exercises is found in my video library.
Fig. 8

When training the rotator cuff, we have to keep in mind that these muscles perform rotation. The cleaner we can perform that rotation over the humeral axis, the better stimulus and less compensation we will get. This applies especially to the subscapularis, which is often inhibited. The subscapularis is an internal rotator; the same are the pecs, lats, teres major and medial deltoid. As the reader can understand, there is extreme potential for compensation by these bigger, stronger surrounding muscles. Training of the subscapularis has to be done in a very specific way, to be effective.
Strength wise, there are some guidelines that we can follow. I got the ER strength table from Charles Poliquin, and the IR from Bill Hartmann.
- External rotation: 10 reps at 10% of 1rm horizontal press / pull.
- Internal rotation, 30% stronger than external rotators.
So, if you have a 300lb bench press, you will want an estimated 10 clean reps at 30lbs (300*0.10) external rotation, and (300*0.13=) 39lbs for internal rotation. This way you can easily compare your strength levels with your rotator cuff stabilizing adequacy at any time; no guessing. I advice to train it after your session, as you do not want to exhaust these muscles prior to training heavy exercises that strain the shoulders. 2×12, twice per week should work fine for most people.
Coracoid impingement
A much rare, but often chronic state of shoulder pain is impingement between the lesser humeral tubercle (and subscapularis tendon) and the coracoid process.
Coracoid impingement syndrome is a less common cause of shoulder pain. Symptoms are presumed to occur when the subscapularis tendon impinges between the coracoid and lesser tuberosity of the humerus. It is the variation in the height and length of the coracoid process in most cases that is responsible for altering the size and shape of the space between the coracoacromial arch and the rotator cuff. – Okoro et al., 2009
Fig. 9

Coracoid impingement often presents with pain in the coracoid area, when the shoulder is elevated (flexion), adducted and internally rotated. Elevation and horizontal adduction seems to be the two most relevant factors. The main cause of this occurrance seems to be anatomical (structural) anomalies, such as excessive length, pointiness or angle of the coracoid process, causing the margin of error of scapular movement to become drastically reduced.
To understand why this happens, you have to also understand how the humerus and acromion moves together when the scapula medially, laterally, anteriorly and posteriorly rotates. It’s a little complicated, but basically the coracoid process moves away from the subscapularis’ tendon and lesser humeral tubercle when the scapula posteriorly and medially rotates. If it anteriorly and laterally rotates, they draw closer together, and if the acromial process then has excessive length they may ram into each other, often leading to chornic inflammation of the subscapularis aswell as potential rupture of the tendon. AC-impingement, which is far more prevalent, will not injure the subscapularis tendon.
If you go back and look at figure 6, although in severe anterior rotation, this is not a scenario that will cause coracoid impingement. The scapular position in the picture below however, if the arms raise and horizontally adduct in the current scapular position (which is sadly promoted by many quacks out there), may definitely cause coracoid impingement if there is excessive length or lateral position of the coracoid process. Although it has a nice posterior tilt, it is in full retraction and lateral rotation, putting the coracoid process in a much more lateral position than it would if the scapula medially rotated as it should.
Fig. 10

The solution to coracoid impingement is to encourage a greater degree of medial rotation of the scapula during shoulder flexion and horizontal adduction. By thinking about doing the opposite as in figure 10, in other words pulling the scapula inward, this will distance the coracoid from the subsapularis tendon. Additionally, strengthening of the shoulder external rotators, teres major, pecs and often the infamous pectoralis minor may be very beneficial. Remember though, that the motor pattern must be dealt with simultaneously by actually practicing proper movement, just as mentioned earlier.
And stop pulling your shoulders back. It’s dysfunctional; based on nothing but bro-science. Yes, it will reduce your ROM, but it will also cause a dysfunctional relationship between the scapula and thorax, inhibiting proper force transfer. Imagine a boxer pulling his scapula back before he punched. No, it will never happen, because it is indeed dysfunction. Many people may get away by doing it, but for someone with predisposition to coracoid impingement, it’s a devastating strategy for scapular control.
If the coracoid is extremely long, pointy and laterally shifted, surgery (shortening) of the coracoid process may be necessary. I’d say that almost all cases should be able to rehabilitate by learning proper motor patterns, though. Severe cases (severe coracoid anomalies) may need to encourage a greater degree of medial rotation during shoulder flexion and horizontal adduction than others.
In conclusion
The majority of difficult shoulder problems, are in reality a scapular stability problem. Assessing and treating scapular dyskinesis can be difficult to learn, but well worth the hassle. First the scapular resting position must be optimized, secondly its movement. Third, or in a parallel manner, the rotator cuff can be strengthened. The rotator cuff dysfunction should be viewed as a symptom and not the cause of the problem, in the utmost majority of cases. If a person has shoulder pain, and there’s no sign of scapular dyskinesis – presuming your assessment is correct – then it’s most likely just a rotator cuff weakness issue.
- Scapular resting position – Superior angle : T2 vertebrae
- Scapula (glenoid cavity) must follow arms’s direction, to avoid impingement
- The rotator cuff’s strength must be strong enough to withstand the loads imposed on the joint
Once scapular movement is really optimized, chances are you’ll never have a shoulder problem in training, again.
Sir im from mauritius and I’m 20years pods and still school… it would be great if you could seem me by email the book evan osar corrective exercises and any other boooks of you…. please i dont have the means to buy books are very expensive and i dont have parents. I live with my grandma and grandpa.
Please send me some books of evan osar and you please….
Sir im from mauritius and I’m 20years pods and still school… it would be great if you could seem me by email the book evan osar corrective exercises and any other boooks of you…. please i dont have the means to buy books are very expensive and i dont have parents. I live with my grandma and grandpa.
Please send me some books of evan osar and you please….
Hi,
first thanks for the very useful articles, i read a lot about shoulder issues etc, but most of them teach things like “pull back and down your shoulders”. I have one question: is it possible to get biceps tendonitis from coracoid impingement? Since 3 years now, when i start to train again, my anterior shoulder (near the coracoid) starts to hurt, and if I dont stop training for a few weeks, the pain also starts moving down the long biceps tendon. I already visited some orthopaedic specialists, and had 2 MRI’s done. They all said the MRI looks fine, and that i should just stop lifting.
Biceps; yes, the tendon rubs into the coracoid during flexion and adduction. This can also be musculocutaneous nerve entrapment, which has other potential causes such as coracobrachialis dysfunction (severe weakness), and thoracic outlet syndrome (“double crush”).
Hi,
first thanks for the very useful articles, i read a lot about shoulder issues etc, but most of them teach things like “pull back and down your shoulders”. I have one question: is it possible to get biceps tendonitis from coracoid impingement? Since 3 years now, when i start to train again, my anterior shoulder (near the coracoid) starts to hurt, and if I dont stop training for a few weeks, the pain also starts moving down the long biceps tendon. I already visited some orthopaedic specialists, and had 2 MRI’s done. They all said the MRI looks fine, and that i should just stop lifting.
Biceps; yes, the tendon rubs into the coracoid during flexion and adduction. This can also be musculocutaneous nerve entrapment, which has other potential causes such as coracobrachialis dysfunction (severe weakness), and thoracic outlet syndrome (“double crush”).
Hi,
I found this article extremely useful, but I am confused on how to exactly fix my scapular positioning. It the scapulae are too low and this is due to the traps being inhibited how to you engage the traps to lift them? Should I be doing a mini shoulder shrug all the time? Thanks for any advice!
Sam
Hi,
I found this article extremely useful, but I am confused on how to exactly fix my scapular positioning. It the scapulae are too low and this is due to the traps being inhibited how to you engage the traps to lift them? Should I be doing a mini shoulder shrug all the time? Thanks for any advice!
Sam
Sam: Glad to hear it. Yes, minishrug all the time, that’s a good way to put it. You’ll get used to it within a few weeks.
very informative. What difference would “internal impingement” be compared to the impingements you mentioned here on the article, if any. Or is coracoid impingement internal impingement? Anyhow i do understand that basically any type of impingement is because of scapular position and movement.
It is a nonspecific term suggesting pain upon internal rotation. it is usually related to the coracoid in my experience, and anterior shoulder pain
kjetil pleasure man, i highly admire you, I am struggling with shoulder pain, I am a amateur boxer and its been literal hell not being able to train i need to get back. In the middle of setting up a skype with you, see you soon. Thank you for your knowledge.
Hi I’ve been working with PT for almost 9 months for anterior shoulder pain. Now they just discovered that my upper traps are overactive and my supraspinatus is atrophied. MRI shows tendonosis of the subscapularis. Also have numbness and tingling in hand when stretching pecs or doing the T exercise. My progress has been almost non-existent. The therapists have been doing lots of stretching and low weight internal and external rotation, wall slides, foam roller thoracic spine. They also have me pull back and down – which flares the numbness. The painful shoulder is also rotated forward – I cannot rotate it back. What would you recommend that I try to help me recover? Thank you for your willingness to share you knowledge
Your upper trap is not overactive. This is a huge myth and following “therapy” for this “problem” will only make you worse. You are most likely dealing with a combination of mild thoracic outlet syndrome as well as scapular dyskinesia. As for treatment, I recommend that you read my scapular dyskinesis article.
Thank you for a very informative article. I feel like Ive had a @winged out,” right scapula all of my life.
Have an isolated winged scapula issue where if I don’t focus I face a problem during normal Glenohumeral Extension. I can activate the muscles to prevent it but curious which muscles likely need to be strengthened. Been doing stretches for months to allow the proper position so now I think strengthening is next.