Tinnitus is a common hearing disorder that affects up to 80% of the population at one time in their life, whilst approximately 5-20% of the younger (than 50 years of age) population are experiencing it in a prolonged manner. It is more common in senior population. Although, in general, only about 2,5% of the affected people are experiencing severe, continuous tinnitus symptoms (Møller, Textbook of tinnitus, 2010)
It is known that the cause of tinnitus and similar disorders may have many causes, such as being exposed to excessive sounds, otitis, otosclerosis, MS, atherosclerosis, tumors, aneurysms and so on. Less known, is the notion that temporomandibular joint, and neck disorders also may cause tinnitus. This article will be addressing the lesser known causes of tinnitus, relating to jaw and neck disorders, how to identify them, and how to treat them. The principles in this article are also applicable when treating vestibular and other otic disorders who have MSK (musculoskeletal) components.
Function and anatomy of the ear
To understand why the neck and jaw may influence our hearing, we first need to look at how sound signals are generated and sent to the brain for interpretation, as well as get acquainted with the relevant anatomy.
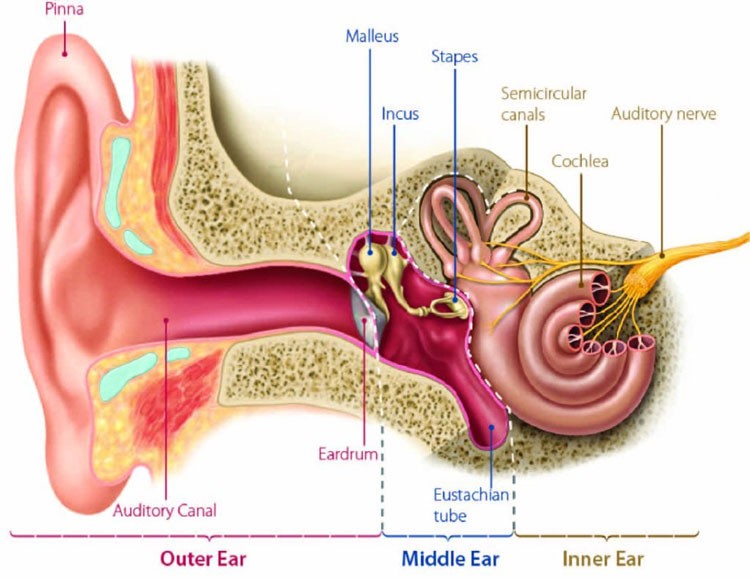
The ear is a very complex network of structures which contribute both to our sense of hearing as well as balance, i.e the vestibular system. There are three main segments of the ear, namely the external, middle and inner portions. Let’s have a closer look.
Fig. x
The external ear, also called the ‘pinna’ or ‘auricle’, is designed mainly to capture the sound waves. The design of the ear’s lobes make it perfect to collect waves and funnel them to the eardrum, which is also known as the tympanic membrane, via the external auditory canal. The external auditory canal is an approximately one inch long tubular structure that the sound waves travel through, ultimately hitting the eardrum and causing its vibration. It has a natural secretion of cerumen (ear wax) that protects the canal and prevents unwanted entities or particles to enter it, thus protecting the eardrum and middle & inner ear segments.
Fig. x

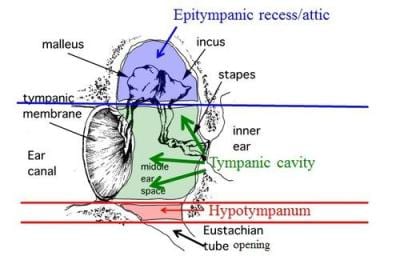
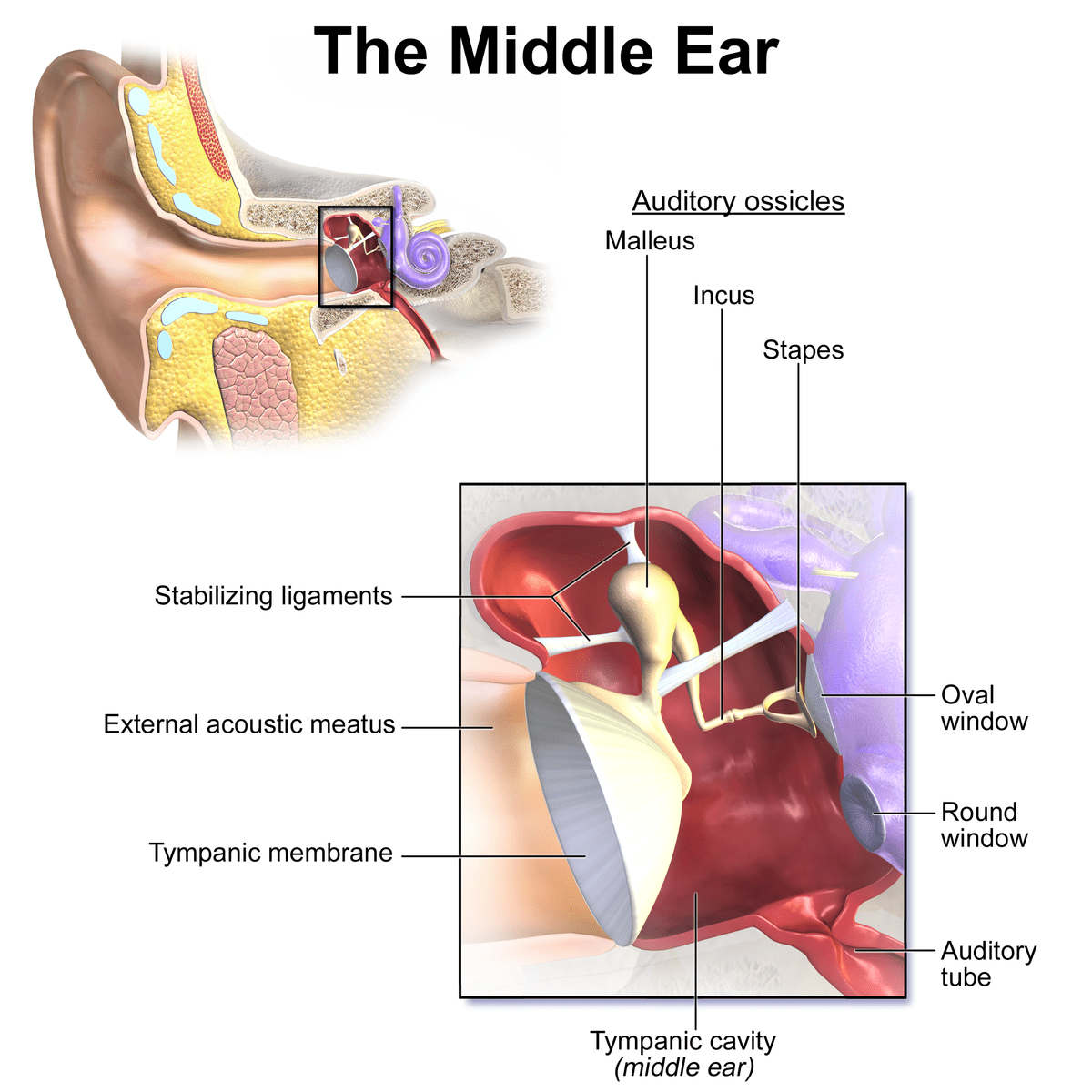
The middle ear involves the parts between the ear drum and the oval window of the cochlea. This area mainly consist of the ossicles, eustachian tube and the tympanic plexus. It is a space that has three named segments, called the epitympanic, mesotympanic, and hypotympanic recesses. These walls of these compartments have mucosal membranes, which are used for clearing out waste products. This transport mechanism (i.e the mucociliary transport mechanism) drains mucus away from the middle ear, and into the nasopharynx via the eustachian tube, thus preventing infection from occurring in the middle ear.
Fig. x
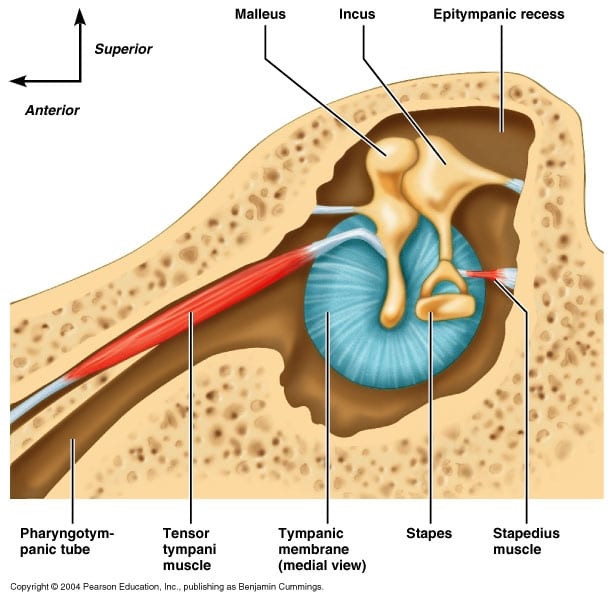
The ossicles are the three smallest bones in the human body, and their job is to transfer but also modulate the strength of vibratory energy (sound wave vibrations) into the cochlea. These three bones are the hammer (malleus), anvil (incus), and the stirrup (stapes), where the latter connects with the oval window, which is a membrane that covers the entrance to the cochlea. Two muscles control the tension between the hammer and tympanic membrane, as well as between the oval window and stirrup, namely the stapedius and tensor tympani muscles. When they contract, vibration and thus also sound is dampened, which should occur when loud sounds enter the auditory canal (i.e the acoustic reflex). Louder sounds will cause greater contraction, and vice versa. This is important to remember because we will be talking about this more.
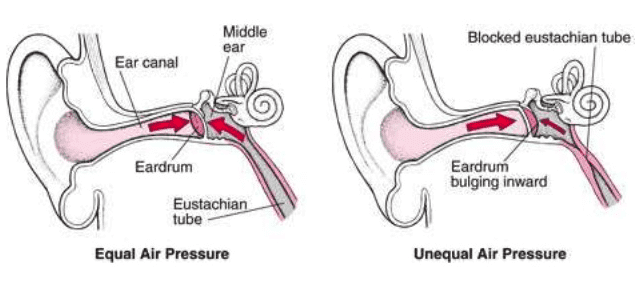
The eustachian tube’s main role is to equalize the pressure between the in- and outside of the ear, i.e on both sides of the eardrum. It is (in normal circumstances) closed at rest, as it’s being compressed by the surrounding structures, as well as due to being recoiled by the distal cartilaginous part (Bluestone & Klein, Otitis media in infants and children, 2001). If there are uneven pressures, the eardrum can not vibrate normally and thus hearing may become impaired to various degrees, depending on the degree of pressure discrepancy. Increased pressure in the middle ear, usually due to inability of the eustachian tube to open, will restrict vibrations in the eardrum and thus also dampen hearing. It may also cause pain. On the contrary, inadequate pressure may cause excessive mobility of the eardrum, making it more sensitive to imposed vibration. The eustachian tube automatically opens when you swallow, which is the pressure regulatory mechanism, and it is controllde by three muscles called the tensor veli palatini, levator veli palatini and salpingopharyngeus.
Fig. x
The inner ear consists of the cochlea, the vestibular labyrinth, and the vestibulocochlear nerve.
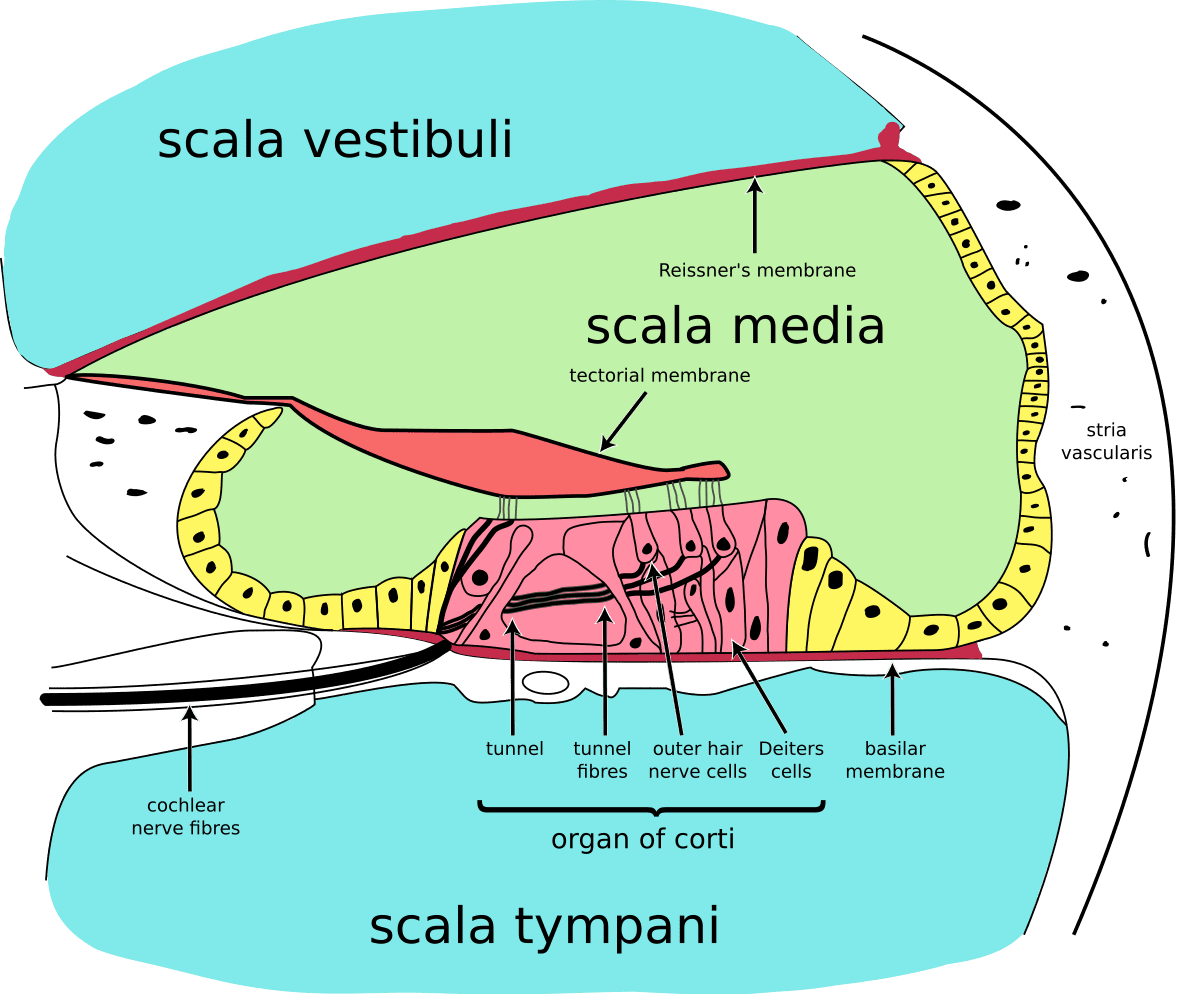
The cochlea, as mentioned, is the snail-shell-like organ that transforms vibrations into electrical signals that the brain can interpret. This organ has three channels. Two perilymph ducts called the scala vestibuli, which is the duct which receives vibration via the oval window, and scala tympani, which is a continuation of the scala vestibuli that ends at the round window (see illustration below). The last and different channel is called the scala media.
The scala media is also called the endolymphatic duct, and it containts endolymphatic fluid, as well as the main hearing organ which is called the organ of Corti. The organ of Corti holds hair cells called stereocilia, and it is situated on a membrane called the basilar membrane. Above the organ of corti (still inside the endolymph duct) is the tectorial membrane, and above this, the Reissner’s membrane. The Reissner’s and basilar membranes separate the endolymphatic duct from the two perilymphatic ducts.
Fig. x
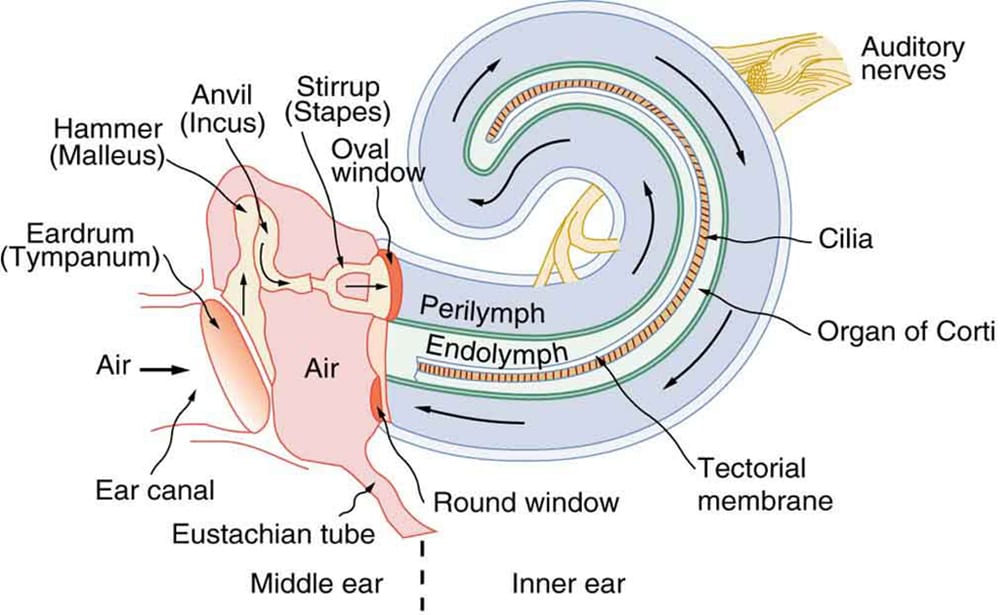
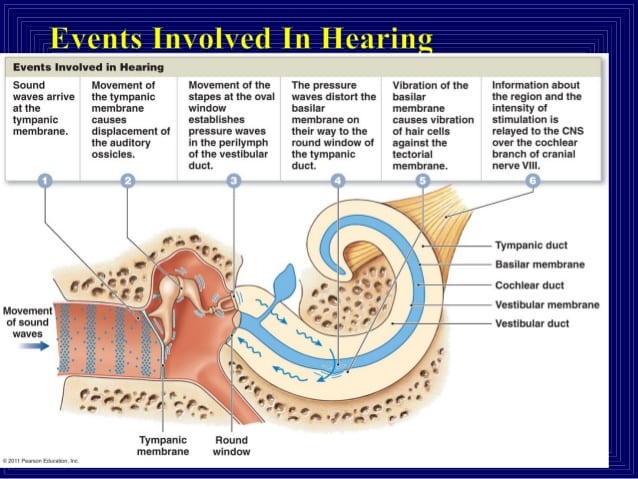
When the stapes vibrate onto the oval window membrane, vibrations enter the perilymph duct (scala vestibuli) causing its fluid to vibrate. In turn, this will vibrate onto the Reissner’s and basilar membranes, subsequently causing the organ of Corti and tectorial membrane to vibrate as well, which stimulates the stereocilia (hair sensors), which in turn produce the electrical signals that are sent to the brain for interpretation.
The round window has no direct function in vibratory reception, but rather acts like an elastic membrane, so that the cochlear fluids are enabled to move. Fluid is generally incompressible, and if the distal cochlear duct (perilymph) had a rigid distal wall, the vibratory energy received in the oval window would inevitably be prevented. However, because the elastic round window membrane is present, it allows the vibratory energy to move through the perilymphatic fluids.
Fig. x
The vestibular portion of the inner ear, also known as the labyrinth, consists of two otolith organs: The utricle and sacculus, which register linear movements (anterior, posterior, lateral, medial, up, down), and three semicircular canals which register rotational movements (yaw, pitch, roll).
Although the vestibular system is not the subject of this article, it is undeniable that hearing and the vestibular functions are linked, as the cochlea and vestibular chambers are literally connected. Let us briefly talk about how it works.
Fig. x
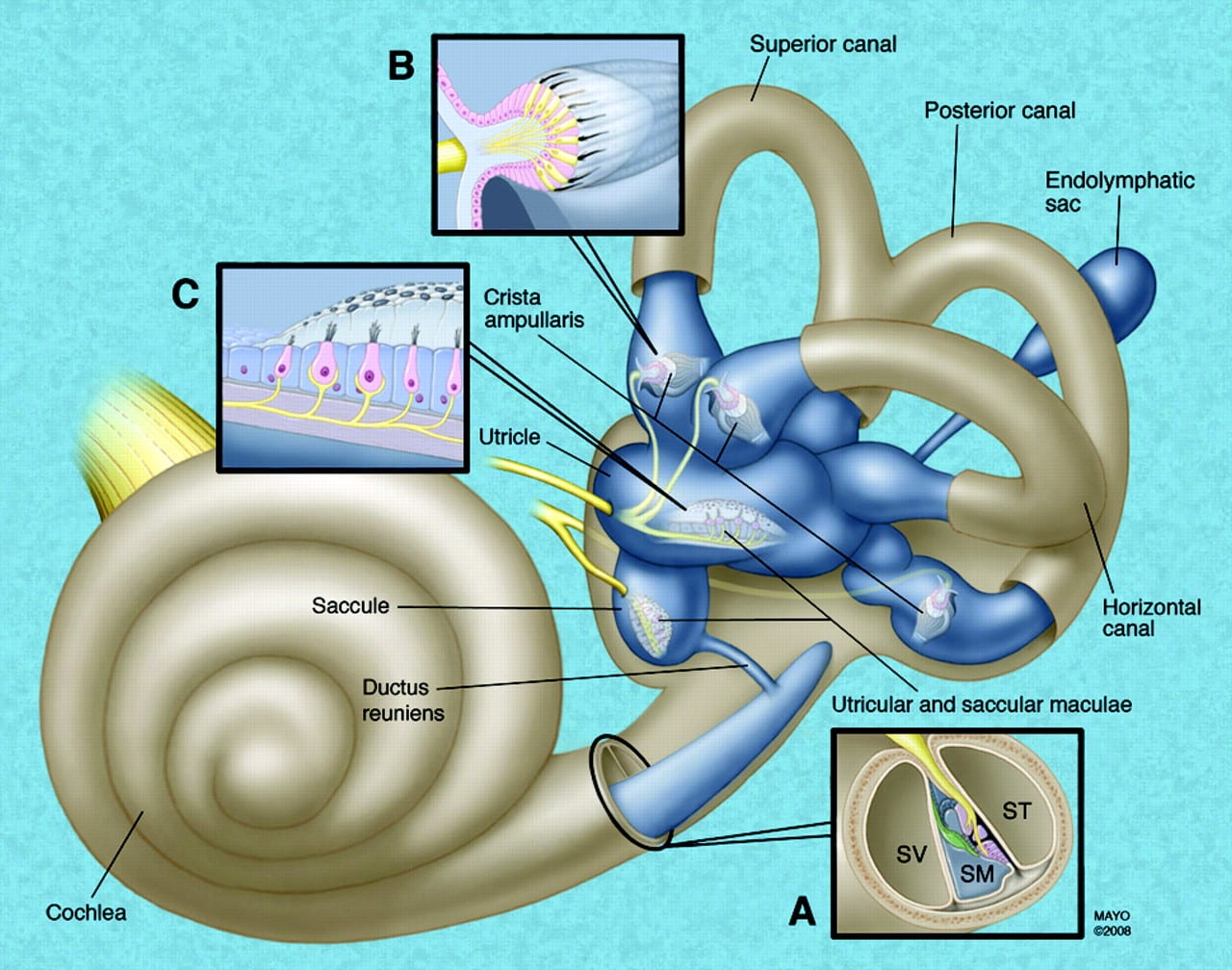
The otolith organs consist of a otolith crystals, the otolithic membrane and the stereocilia hair sensors. The otolith crystals are attached to the otolithic membrane, as showed below, and they move in accordance with gravitational forces as well as momentum. If someone pushes you forward, for example, the otolith & hair sensors would be pulled backwards, creating electrical signals translated from the body’s position and movement to your brain and thus allowing precise counter movement being organized in the cerebellum.
The sacculus register vertical (longitudinal) and lateral (coronal) movements, and the utricle register forward, backwards (sagittal) and lateral movements. Thus they both have a common ground in coronal movements, but are unique in perceiving longitudinal and sagittal movements. This is because the sacculus is positioned in a 90˚ angle compared to the flat-lying utricle.
Fig. x
There are three semicircular canals, as mentioned already. The posterior canal registers pitch, which is a coronal axis rotation. The anterior canal registers rolls, which is a sagittal axis rotation. And, finally, the lateral canal registers yaw, which is a longitudinal axis rotational movement.
The hair sensors in the semicircular canals are stimulated a little differently than the otolith organs. The canals are filled with endolymphatic fluids, just like in the cochlea, and movement of this fluid will move the hair cells and thus create signals as to which movements are occurring, which are then sent to the cerebellum for interpretation. The endolymphatic fluid is produced by the stria vascularis, which is the outer wall of the cochlear canal, as well as by dark cells within the labyrinth, located in the saculus and utricle. It is also regulated by the endolymphatic sac, as well by the tympanic plexus. Improper endolymphatic regulation will influence both hearing and balance, which we will discuss in a minute.
The stria vascularis and vestibular dark cells are the two main structures responsible for endolymph secretion, and possess many similarities. The characteristics of these structures are the basis for regulation of inner-ear homeostasis – Ciuman, 2009
Fig. x
In summary
Sound waves hit the eardrum, which in turn carries the vibration via the ossicles to the oval window membrane. The strength of the vibrations delivered to the oval window membrane depend on the pressure within the middle ear (which is controlled by the eustachian tube), as well as the degree of contraction of the stapedius and tensor tympani muscles, which attenuate the vibratory signal. From the oval window, the vibratory motion is transfered into the perilymphatic liquid, which in turn cause the basilar membrane which the organ of corti is situated upon, as well as the Reissner’s membrane, to vibrate. This vibration causes the organ of Corti and its hair cells to contact with the tectorial membrane. Degree of vibration is regulated by amount endolymphatic volume, i.e. hydraulic pressure within the scala media. Finally, the stimulus of these hair cells generate electrical signals which are sent to the brain for interpretation.
Fig. x
The mechanism of sound attenuation & amplification
As I see it, there are five main controllable factors that will alter sound perception (this list is not written in stone):
- Tympanic membrane tension
- Degree of mobility of malleus
- Degree of mobility of the stapes
- Middle ear cavity pressure
- Endolymphatic fluid volume
Tension of the tympanic membrane & ossicles
As we have learned, level of vibration of the tympanic membrane will under normal circumstances correlate with the level of sound we perceive. There are several mechanisms that reduce both its own vibration, as well as the vibratory translation that reaches the organ of corti. However let us now speak about vibratory attenuation and amplification of the tympanic membrane itself and the ossicles, as this will be one of the main and initial mechanisms for sound modulation.
The tympanic membrane attaches to the malleus, and the looser these structures are, the more sensitive they will be to the sound waves that enter the external auditory tunnel. The tensor tympani attaches to the handle of the malleus, and when contracted, it will pull the handle medially, tensing both the eardrum and the malleus, thus reducing vibratory sensitivity as well as ability. Laxity of the tensor tympani will increase sound wave sensitivity. The tensor tympani also attaches to the eustachian tube, but it is unlikely to control the E.T. as this would require force so great that auditory transmission would be impaired. It is much more likely that the tensor tympani sense the status of the E.T. (amongst other factors), and regulate tension on the malleus and tympanic membrane in accordance with this.
At the end of the ossicular complex, namely at the stapes (stirrup), another modulatory mechanism is at place; the stapedius muscle. It works in similar fashion: It attaches to the stapes, and pulls it laterally when contracting. This will tense the stapedius and thus attenuate the level of vibratory energy that is transfered into the cochlea through the oval window. Once again, laxity of the stapedius will increase vibratory potential as well as transmission into the cochlea. Thus, both the stapedius and tensor tympani muscles are crucial elements of sound modulation in the ear.
Fig. x
Tympanic and ossicular innervation
It is very, very important to understand – at least know of – these structures’ basic innervation, as its originating from the neck and jaw. These nerves may entrapped several places and thus its electrical signalling may become impaired, which I will be talking more in depth about later.
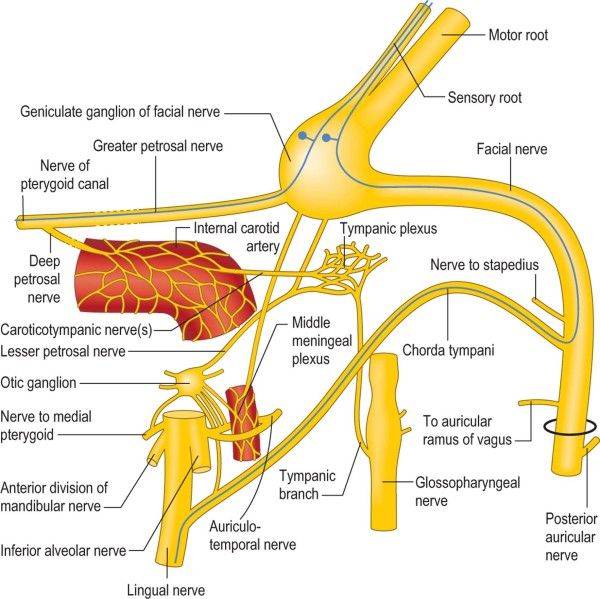
The tympanic membrane is innervated by several nerves. The external surface receives sensory innervation from the auriculotemporal branch of the trigeminal nerve, the auricular branch of the facial nerve, the auricular branch of the vagus nerve, and the glossopharyngeal nerve. The inner surface, however, is solely innervated by the tympanic branch of the glossopharyngeal nerve (Szymanski & Bhimji, 2017). These nerve sense the tympanic membrane’s movement and regulate the rest of the chain in accordance with this, i.e. endolymphatic volume, TT & stapedius tension, as well as tympanic cavity pressure.
The tensor tympani is innervated by the tympanic plexus and trigeminal nerve, while the stapedius is innervated by the facial nerve (O’Rahilly et al., Basic human anatomy).
The tympanic plexus is formed by several nerves, namely the glossopharyngeal nerve, the facial nerve, and sympathetic fibers coming from the internal carotid plexus. However, it also communicates with the trigeminal nerve via the otic and pterygopalatine ganglia as well as the vagus nerve via the glossophargyneal nerve. It supplies the mucosa of the middle ear, the mastoid cells, the auditory tube, and parotid glands. – Barral & Croibier, Manual Therapy for the Cranial Nerves, 2009
From the tympanic plexus, two branching patterns arise: one to pass to the mucous membranes of the tympanic cavity, auditory tube, and mastoid air cells. The other branch gives the lesser petrosal nerve. It is this nerve that contains the fibers destined for the parotid gland. – Rea, 2016
Fig. x
Tympanic cavity pressure & the eustachian tube
As touched upon, the pressure within the tympanic cavity (middle ear) can both attenuate and amplify perceived sound.
Increased pressure within the middle ear cavity will restrict movement of the tympanic membrane and thus attenuate vibratory motion (presuming the pressure is relatively stable). For normal vibratory motion of the tympanic membrane to occur, there must be equalized pressure between the external and internal sides of the eardrum, and this is controlled, as mentioned, by opening of the eustachian tube during swalloing. Inability to close the eustachian tube (called ‘patulous eustachian tube’) will thus, genereally, cause loss of tympanic cavity pressure and subsequent hypermobiliy of the tympanic membrane. Studies have however suggested that a patulous eustachian tube may cause increased tympanic pressure (and laterally bulging tympanic membrane) during exhale, and the opposite (lack of pressure and medially pulled tympanic membrane) during inhale. On the contrary, inability to close the eustachian tube (called ‘eustachian tube dysfunction’) will cause continuous pressure build up, which in turn may cause hearing loss, as the eardrum becomes hypomobile.
Pressure equalization in the tympanic cavity is largely based on the sensory input from the tympanic membrane. As I mentioned above, it is richly innervated by many autonomic nerves. The degree of movement as well as its resting positioning (concave/convex) would indicate whether or not the pressure is equalized, and the eustachian tube will open or stay closed in order to regulate this. The main mobile part of the tympanic membrane is called pars flaccida, which has been shown to alter position in accordance with pressure changes. If there is a low pressure even when the eustachian tube is closed, gas may enter the tympanic cavity via the mastoid cells or tympanic mucosa, to aid in barometric equalization. Abnormal position or movement of the tympanic membrane may thus reasonably cause a chain reaction where the body tries to ‘fix the mess’, perhaps only to exacerbate the situation, e.g. if the eustachian tube is unable to open or close. Both the eustachian tube, mastoid cells, and the tympanic mucosa has been suggested to be involved in tympanic cavity pressure regulation.
In children with ostitis media effusion, the functional volume of mastoid cell system acting as a pressure buffer and the surface area serving for gas exchange are small. – Csakanyi et al., 2011
Small fluctuations in pressure gradients of the middle ear can be buffered by the limited mobility of tympanic membrane. The two compartments are covered by the same respiratory mucosa. As the gas is exchanged through the mucosa of these cells, the total area of the mucosal surface directly reflects the rate of gas exchange.5 Sadé reported that the retraction of the TM is a compensatory mechanism that aims to keep the ME pressure constant.7 – Rios Lima et al., 2014
By using a sond placed either in the tympanic bulla or in the Eustachian tube in the rat, the middle ear can be insufflated or aspirated with exact volumes of air. Pars flaccida reacted promptly to the changes, while pars tensa remained immobile. A large air volume caused perforation of the pars flaccida. It seems that pars flaccida’s function may consist in maintaining a constant middle ear pressure within certain limits, by changing its position. – Stenfors et al., 1979
As mentioned, the eustachian tube should be closed at rest. Three muscles are involved with opening the eustachian tube, however, which occur when swallowing, by pulling on the torus tubarius (the nasopharyngeal, cartilaginous part of the eustachian tube). These are the tensor veli palatini (innervated by the trigeminal nerve), as well as the levator veli palatini and salpingopharyngeus muscles (both innervated by the vagus nerve). Also, in opposition with some claims, the tensor tympani has no active role with regards to function of the eustachian tube; if it did, each swallow would greatly affect tympanic tension and hearing. Moreover, according to Bluestone & Klein (2001), the internal (lateral) pterygoid muscle aids in closure of the eustachian tube in certain population. They also claim that only the tensor veli palatini has a significant role in opening the eustachian tube.
The eustachian tube itself is innervated by a branch from the otic ganglion, the sphenopalatine nerve, and the pharyngeal plexus, as well as sensory innervation from the tympanic plexus and the pharyngeal plexus.
It was revealed that contraction of the tensor tympani muscle during swallowing did not result in any tympanic pressure rise which might assist in tubal ventilation. Acoustic stimulation was then used to measure consistent contraction of the tensor tympani muscle. Combined contraction of the tensor veli palatini and tensor tympani muscle under the condition of positive tympanic pressure failed to open the tube. It was concluded that the tensor tympani muscle might not play any part in tubal function. – Honjo et al., 1983
The eustachian tube also functions to protect the middle ear from excessive sound pressure, and nasopharyngeal secretions. The eustachian tube helps drain the middle ear during opening and closing by pumping secretions from the middle ear; clearance of secretions also occurs. – Bluestone & Doyle, 1988
The glossopharyngeal nerve probably plays the predominant role in tubal innervation. Sympathetic innervation of the tube depends on the sphenopalatine ganglion, the otic ganglion, paired glossopharyngeal nerves, the petrosal nerves, and the caroticotympanic nerve (Proctor, 1967). Mitchell (1954) suggested that the parasympathetic nerve supply is derived from the tympanic branch of the glossopharyngeal nerve. Nathanson and Jackson (1976) provided experimental evidence for secondary parasympathetic innervation via the Vidian nerve from the sphenopalatine ganglion. – Swarts & Rood, 2005
The Eustachian tube mucosa was found to be sympathetically innervated by fibres originating in the ipsilateral superior and middle cervical ganglia, but not by those originating in the stellate ganglion. The Eustachian tube mucosa was also innervated by fibres originating in the pterygopalatine ganglion, but not by those originating in the otic ganglion. – Oyagi et al., 1988
The pharyngeal orifice of the eustachian tube is innervated by branches from the otic ganglion, the sphenopalatine nerve, and the pharyngeal plexus. The remainder of the tube receives its sensory innervation from the tympanic and the pharyngeal plexuses. The glossopharyngeal nerve probably plays the predominant role in tubal innervation. Sympathetic innervation of the tube depends on the sphenopalatine ganglion, otic ganglion, paired glossopharyngeal nerves, petrosal nerves, and caroticotympanic nerve (Proctor, 1967). Mitchell suggested that the parasympathetic nerve supply is derived from the tympanic branch of the glossopharyngeal nerve (Mitchell, 1954). Nathan and Jackson provided experimental evidence for a secondary parasympathetic innervation by the vidian nerve from the sphenopalatine ganglion (Nathan & Jackson, 1976). – Bluestone & Klein, Otitis media in infants and children, 2001
Fig. x
Endolymphatic fluid volume
Studies show that the endolymph fluid volume, and thus also its hydraulic pressure increases when the ear is exposed to loud noises (Salt, 2004). It would thus make sense to assume, that both contraction of the stapedius and tensor tympani, increased endolymphatic fluid secretion and perhaps also increased tympanic cavity pressure, are all protective mechanisms to shield against excessive sounds, i.e the acoustic reflex, as they reduce vibratory motion, as well as a part of the main auditory regulatory mechanism.
The reason increased endolymphatic volume shields against loud sounds, is because it will somewhat overfill the endolymphatic cavity (the scala media), causing rigidity of the scala media and thus restrict vibration of the Reissner’s and basilar membranes. As you probably remember, movement of the Reissner’s and basilar membranes is what cause the stereocilia hair cells to rub against the tectorial membrane, which in turn produces sound signals which are sent to the brain through the cochlear nerve. Likewise, decrease of endolymphatic volume will increase the mobility of these membranes and thus, similar to the tympanic membrane, make it more sensitive to vibration (sound). The pressure in the endolymph and perilymph ducts should be equal during normal circumstances, according to Böhmer (1993).
Endolymphatic fluid is regulated in several ways. The main production site of endolymphatic fluid is the stria vascularis and labyrinthic dark cells, as mentioned earlier. However, the endolymphatic sac (controlled by the Bast’s valve) is thought to regulate the endolymphatic homeostasis by allowing fluid to enter the endolymphatic ducts when volume is low, and return when volume is high (Corrales and Mudry, 2017). Furthermore, venous drainage, i.e. removal of the bygone endolymphatic fluid occurs via the inferior cochlear vein (through the canal of Cotugno) and the vein of the vestibular aqueduct (through the paravestibular canaliculus). Arterial supply comes via the labirynthine & meningeal arteries. Eckhard (2015) also showed that parasympathetic fibers regulated fluid levels in the three cochlear ducts, and seeing as the only cranial nerves that have parasympathetic fibers are the CN3, 7, 9 and 10; i.e. the oculomotor, facial, glossopharyngeal and vagus nerves, it is likely that one or more of the three latter ones control this process, as they also have been shown to innervate the rest of the tympanic cavity. Both the round and oval windows are innervated by the tympanic plexus.
Fig. x – Cross section of the cochlea, showing the two perilymph chambers and the middle endolymph, housing the organ of Corti
The vein of the paravestibular canaliculus (VPVC) runs parallel to the endolymphatic duct and drains the major portion of the semicircular canals and part of the utricle. – Scaramella, 2003
Previous studies suggest that the endolymphatic sac plays an important role in the homeostasis of endolymph. Factors that influence blood flow in the sac may affect its function. This blood flow may be influenced by autonomic innervation; however, no such innervation has been demonstrated. The purpose of this study was to demonstrate catecholaminergic and cholinergic fibers on the endolymphatic sac. Light microscopy of the whole-mounted endolymphatic sacs revealed tyrosine hydroxylase-positive and acetylcholinesterase-positive fibers. Some of the acetylcholinesterase-positive fibers were clearly associated with vessels. This innervation, which has not been described previously, may significantly influence blood flow and function of the endolymphatic sac. – Brechtelsbauer et al., 1992
The results indicate that sympathetic neurons from the superior cervical ganglion and to a certain extent trigeminal somatosensory neurons innervate the endolymphatic sac or perisaccular tissue. If these findings reflect the existence of a sympathetic functional reflex unit remains to be elucidated. – Birgersson et al., 1992
The main arterial supply of the ED and ES appears to be the occipital artery (24). The paravestibular canaliculus, or accessary canal of the VA, is an often duplicated, diminutive bony canal that carries a vein from the vestibule, parallel to the VA (6, 16). Venous blood from the sac drains into this vein near the external aperture of the VA, as well as through venules directly into the sigmoid sinus (25). Studies suggest that the ED and ES perform both absorptive and secretory (7, 22, 26, 27), as well as phagocytic (28) and immunodefensive, functions (29). – Lo et al., 1997
The endolymph which fills the membranous labyrinth is produced by the marginal cells of the stria vascularis in the cochlea. – Lo et al., 1997
It is generally believed that endolymph flows, when the volume is increased, towards the endolymphatic duct and sac where it is reabsorbed as part of inner ear homeostasis (Guild, 1927). Studies have shown that obstruction of the absorptive ability of the endolymphatic duct and sac, for example by obstruction of the endolymphatic duct, results in endolymphatic hydrops (Lohuis et al, 1999). – Lo et al., 1997
In normal ears, hydrostatic pressure in the perilymph equals pressure in the endolymph, and pressure changes applied to one compartment are immediately transmitted to the other one. A high compliance of Reissner’s membrane seems to be the cause of this endolymphatic-perilymphatic pressure equalization. – Böhmer, 1993
In normal ears, endolymphatic pressure always approximated perilymphatic pressure. Endolymphatic pressure exceeded perilymphatic pressure in all ears with hydrops, except one in which these pressures were equal. The effect of postural inversion on inner ear pressures were studied in both normal and hydropic inner ears. Normal ears showed endolymphatic and perilymphatic pressure to rise equally during this maneuver. In hydropic ears, the difference between endolymphatic and perilymphatic pressure was notably reduced from measurements obtained in the prone position. – Andrews et al., 1991
Sympathetic innervation of the middle ear mucosa was accomplished by fibers originating in the ipsilateral SCG, but not by those originating in the MSG or StG. Parasympathetic innervation was by fibers originating in the ipsilateral PpG, but not by those originating in the OtG. – Ito et al., 2009
Two different systems of sympathetic nerve supply to the inner ear are demonstrated by the histochemical method of Falex and Hillarp: The perivascular adrenergic innervation, which is a continuous plexus around the vertebral, basilar, inferior anterior cerebellar and labyrinthine arteries reaching as far as the modiolar branches. A blood-vessel independant innervation-system which forms a rich terminal plexus in the area of the habenula perforata. On the basis of a larger serie of degeneration studies on cats it appears that the postganglionic fibres of this bloodvessel independent system originate in the superior cervical ganglion and reach the inner ear either via tympanic plexus — facial nerve — internal acoustic meatus or via auricular branch of X — facial nerve and internal acoustic meatus. Clinical implications of these findings are discussed. –
It is conceivable that cholinergic-sympathetic nerves might exist in the human middle-ear mucus membrane, and that these autonomic nerves, in conjunction with the neuropeptides, may play an active role in the pathogenesis of human middle-ear effusion. – Nagaraj & Linthicum, 1998
In rodents at least, the main sources of the perilymph fluid are (1) influx of CSF through the cochlear aqueduct, and (2) blood flow dependent local production within the cochlea. – Kellerhals, 1979
The abundance of AQP5 water channels was increased in vitro by perilymphatic hyperosmolarity and muscarinic (M3) receptor stimulation in OSCs, which indicates the regulation of transcellular water permeability in the OSCs by osmolarity changes in the cochlear fluids and autonomic stimuli. – Eckhard et al., 2015
The multifactorial pathophysiology of hearing disorders
As we have seen until now, the ear alone is a very intricate complex of structures. However, the structures within the ear, and especially those within the tympanic cavity, are largely innervated by nerves other than the vestibulocochlear nerve. Often this nerve, i.e the vestibulocochlear nerve, though innocent, is blamed for aural disorders. The regulation of endolymphatic fluids and tympanic pressures are also regulated by factors that have a high potential for being influenced outside of the ear itself. Therefore, once again, the main focus in this article is to shed light on other potential mechanisms that may alter sound perception, by impairing the systems that were just discussed.
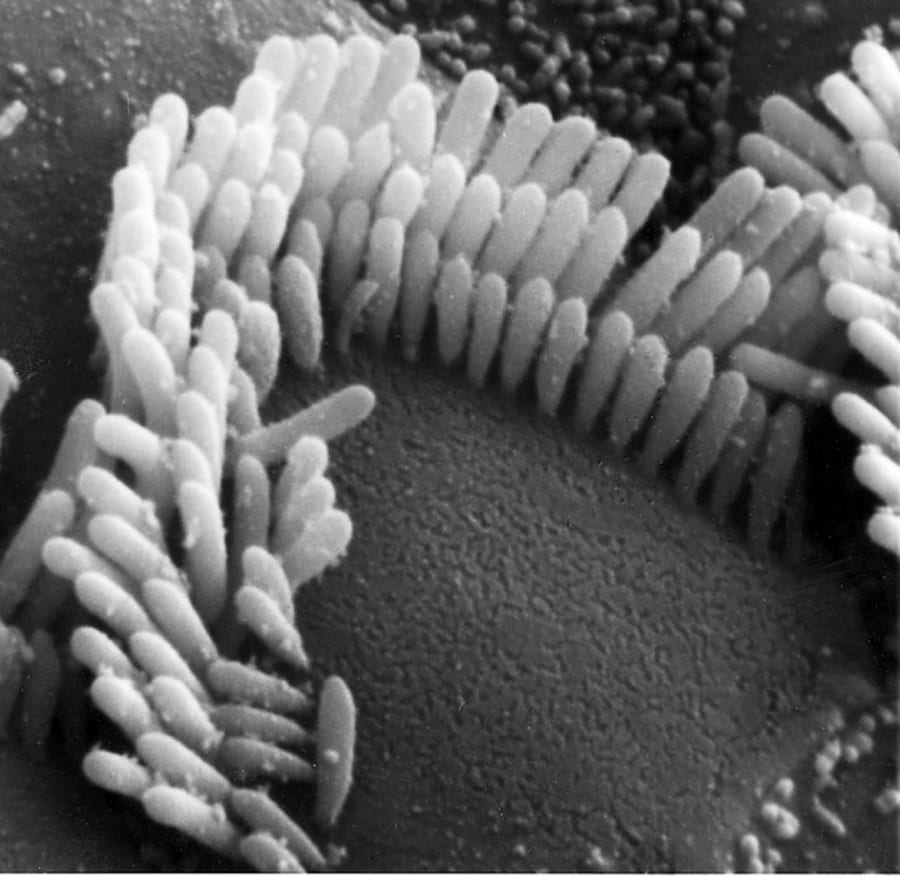
The most common explanation of tinnitus and other hearing disorders, briefly, is exposure to excessive sounds, perhaps prolonged exposure of such. It has been shown that the hair sensors in the organ of corti may be damaged excessive sounds, ototoxic drugs or similar. When they are damaged, they bend, thus preventing them from being stimulated by the tectorial membrane, and also from generating electrical impulses for interpretation in the brain. The picture below show both healthy (straight) stereocilia hair sensors, and damaged (bent) ones.
Because bent hair cells will reduce sound perception, it is reasonable to believe that either decrease in endolymphatic fluid, and/or decrease in tension of the tensor tympani and stapedius muscles, or even tympanic pressure may occur as a compensation, to increase amplification of the sound waves that hit the eardrum. This will cause more vibration to be delivered to the cochlea, but as the tympanic membrane becomes more mobile and thus more sensitive to sound waves, it will pick up sounds that should be blocked out as well. Consequently one may get improved hearing, but also an increase in unwanted noise. Now, briefly, it has been shown that endolymphatic fluid has a high prevalence of being excess in patients with hearing disorders, so the latter factors or are more probable suspects when searching for dysfunction. We will get deeper into this later.
A slight digression, but it is interesting to note that dopamine (a ‘happiness’ neurotransmitter) has been shown to reduce susceptibility to stereocilia damage induced by excessive noise.
It was shown in animal experiments that dopamine agonists reduce cochlear damage by noise or ischemia [55–57] and that this transmitter may protect hair cells in inner ear stress (e.g. ischemia) [58]. – Ciuman, 2013
Fig. x
On another note, many patients with tinnitus or similar disorders may often not been exposed to ototoxic drugs, nor loud sounds or similar known factors that kill stereocilia, and have been screened and found negative of tumors, aneurysms and such known pathologies. Furthermore, a massive number of patient stories testify that they may modulate their hearing disorder by mandibular motion, head postures, and more. Similarly, many studies show that hearing disorders develop post whiplash, for instance, implying a large possibility of external dysfunction contributing to or even causing the hearing disorders. This is, of course, extremely interesting, because although broken hair cells may not be healed, the neck and jaw certainly can be, in many circumstances. This means that improvement, and sometimes even complete reversal of the respective hearing disorder may take place.
Tinnitus and other types of sounds may also have a musculoskeletal etiology. Specifically, cervical factors and mandibular postural factors have been seen in subjects with tinnitus. A combination of physical medicine and dental mouth guard therapy has been effective in some patients with a history of trauma or childhood growth affecting proper expansion of the maxilla. Ear pain that is sharp and jabbing on movement of the mandible is frequently seen in patients with internal derangement of the TMJ. This type of pain is generally unilateral and ipsilateral to the joint in question. Ear pain and symptoms such as stuffiness in the absence of positive otologic findings are among the most common reasons for evaluation of dental- and maxillomandibular-related imbalance. Treatment can often alleviate the symptoms completely or reduce their impact on the patient in conjunction with standard medical intervention.29-34 – Benzon et al., 2013, Practical management of pain 5e.
Frequently, patients report the development of tinnitus after traumatic injuries. However, to which extent this specific etiologic factor plays a role for the phenomenology of tinnitus is still incompletely understood. – Kreuzer et al., 2012
Tinnitus is a significant symptom that commonly occurs as a result of head or neck trauma. The fact that tinnitus resulting from head or neck injuries tends to be more severe (and is often accompanied by a greater number of co-symptoms) than tinnitus resulting from other causes should be taken into account by clinicians treating these patients. – Folmer & Griest, 2003
The contribution of nonauditory centers in the pathogenesis and regulation of tinnitus is reinforced by studies showing that many patients have somatic tinnitus whereby movements and manipulations of the eyes, head, neck, jaw, and shoulder can modulate the loudness and pitch of their tinnitus. In most cases, the maneuvers lead to increases in tinnitus loudness or pitch rather than decreases. Our results indicate that most tinnitus patients experience only a modest change in loudness or pitch when performing these maneuvers. However, some patients report that these maneuvers significantly modulate the loudness or pitch, sometimes by a factor of 2 to 3. The high prevalence of somatic tinnitus serves to illustrate the complex multimodal interactions that exist between the auditory pathway and other sensory-motor systems innervating the head, neck, shoulders, and eyes. – Simmons et al., 2008
Sudden deafness, also called idiopathic sudden sensorineural hearing loss (ISSHL), includes all causes and diseases for sudden hearing loss with unknown etiology. Discussed etiologies include vascular compromise, viral infection, endolymphatic hydrops, autoimmune diseases, and disruption of endolymphatic homeostasis triggered by stress hormones or other hormones. Noise, in contrast to a temporary threshold shift, also called auditory fatigue, which usually recovers in 24–48 hours, permanent threshold shift is characterized by degeneration of hair cells and ganglion cells with a higher vulnerability of outer hair cells than inner hair cells. Sound pressure levels (SPL) over 150 dB and 1.5 ms duration at minimum result in mechanical damage to the middle and inner ear (e.g. hemorrhage, rupture of the basilar or Reissner’ membrane, and damage to the organ of Corti). Damage to the middle ear leads to combined hearing loss patterns. The pathophysiological mechanisms of hearing loss caused by noise, ototoxic agents, in presbyacusis, or ISSHL are alike. – Ciuman, 2013
Many older individuals with impaired hearing do not have tinnitus, possibly because age-related changes in inhibitory circuits are better preserved. – Roberts et al., 2010
Differential aetiologies
Conservative treatment of hearing disorders are, as most chronic ailments, considered controversial and poorly understood. As mentioned, many patients have no history of exposure to loud sounds, yet still develop tinnitus or other related hearing disorders. The disorder may for example develop post whiplash, or the patient may have a history of migraine, and other neck or jaw disorders. The same nerves that regulate audition may become impaired in these areas, due to diverse causes which we are about to look at. Furthermore, vascular relations to the ear may also become compromised.
With regards to the nerves, we know that nerve pain tends to spread out. For example, it is very well known that a disc herniation in the neck or back may cause radiative or shooting types of pain all the way out in the extremities. Dealing with entrapment of autonomic nervous structures, in my experience, it may or may not cause pain, but may also cause spreading symptoms of dysautonomia, causing dysregulation of cochlear fluids, sensory of the tympanic membrane, contraction of the stapedius and tensor tympani muscls, etc. The main point is that we have to be aware that autonomic nerve compression / entrapment will not always cause pain, its dysfunction may also be indicated by dysautonomia, just like parasthesia (cutaneous sensory dysfunction) is indicative of nerve dysfunction, although not painful.
In practice this means, that let’s say the trigeminal nerve is compressed in the temporomandibular joint, its branches as well as distal connections may become affected. The trigeminal nerve innervates the tear canals, and thus may cause tear secretions when yawning, for example, or tinnitus in relation to chewing (as it’s related to the tympanic plexus via the otic ganglion), etc. It may of course also cause ‘mere’ (i.e. well known) pain to develop in the same regions in which it innervates. The possibilities are many, and thus it is crucial to be at least generally aware of innervation as well as common mechanisms.
Because the differential causes of tinnitus and other hearing disorders are so many, I must keep focus on explaining the mechanisms rather than in-detail explanations with regards to treatment. There will be a brief treatment section in the end of this article, but in all majority I must refer you to other articles explaining aetiology and treatment of these complicated pathologies.
The temporomandibular joint
Several studies have noted quite conspicuous correlations between temporomandibular disorders and aural disorders. This section will address the in-depth reasons of why this is, briefly why TMD occurs in the first place, as well as what the research says.
Fig. x
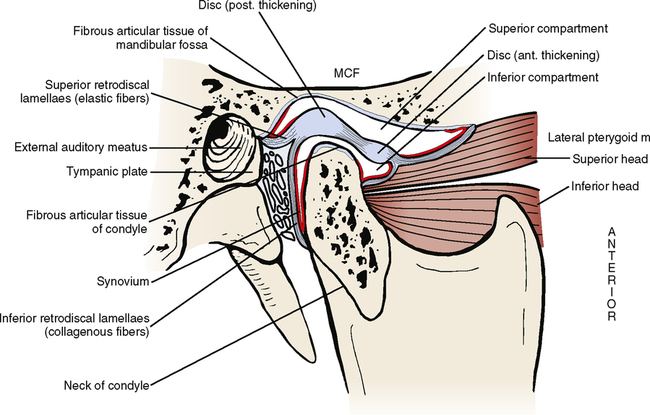
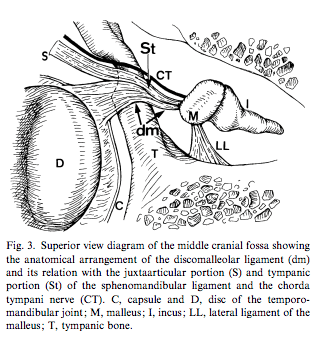
The TMJ is connected to the ear in several ways. Firstly, the superior head of the lateral pterygoid muscle may in some people be directly attached to the ossicles (the malleus / hammer) via the retrodiscal tissue and discomalleolar ligament, which is also known as Pinto’s ligament. In adults, it has been shown be to variably present in cadavers, and currently there is currently no consensus with regards to how common its attachment to the malleus really is. Some relevant studies are cited below. Either way, this shows that there is a definitely possibility of direct manipulation of the malleus via the mandible, in certain predisposed people.
Fig. x
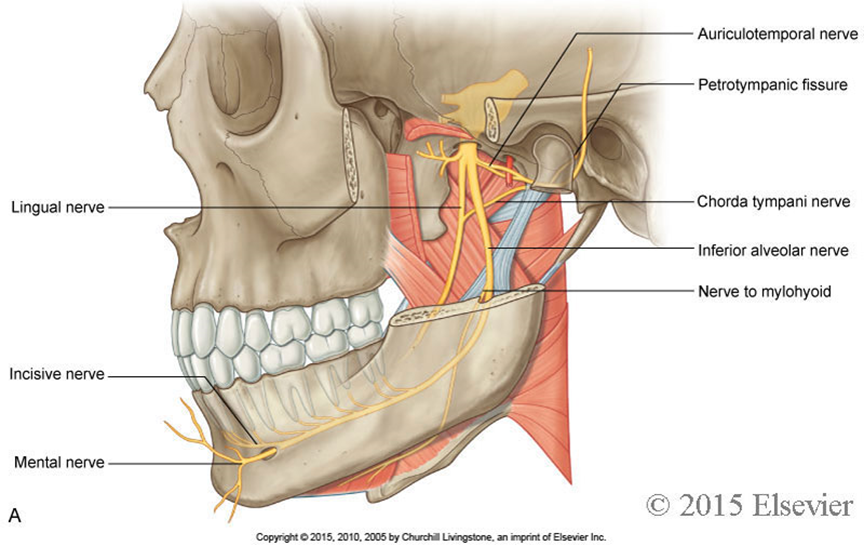
Moreover; between the mandibular cavity (i.e glenoid fossa) and the mandibular condyle, lies the auriculotemporal nerve, which is a branch of the trigeminal nerve. Several studies have noted the relationship between TMD and trigeminal nerve dysfunction, and some have also noted the specific mechanism of why this occurs. Because the trigeminal nerve greatly contributes to innervation of both the external and middle ear, its impairment can and often will lead to aural symptoms, such as tinnitus, hyperacusis, and even hearing loss.
Temporomandibular joint disorder is caused by an overly retracted position of the mandibular condyle (usually due to improper growth of the maxilla and/or open mouth postures), which in turn cause shearing forces to occur within the TMJ. Between the condyle and the joint socket lies an articular disc, which helps the condyle slide through the joint spaces easily. When the condyle is resting too far back, and/or being retracted as the mouth opens (it should protract), this will once again impose compressive forces on the disc and its retrodiscal tissue, causing it to deteriorate. Ultimately, the retrodiscal tissue that holds the disc in place may partially or fully rupture, causing anterior disc displacement. When the disc displaces anteriorly, this will allow the mandibular condyle to translate even further back into the joint socket, and in many circumstances lead to compression of the auriculotemporal nerve, along with the perhaps more conspicuous TMJ pain symptoms that occur. Auriculotemporal nerve compression may also occur without discous displacement, but it is much, much rare, seeing as its compression and disc displacement have the same cause.
The auriculotemporal nerve branch, as we have discussed briefly, innervates parts of the tympanic membrane as well as parts of the external ear. Its compression may cause symptoms of pain and/or dysautonomia to spread through the nervous network in which it is connected, to variable extent (Stack & Sims, 2007). The trigeminal nerve also innervates the tensor veli palatini (which opens the eustachian tube), the tensor tympani muscle, and endolymphatic sac. The eustachian tube’s mucosa is innervated by the pterygopalatine ganglion, which also connects directly with the mandibular (trigeminal) nerve. It also connects to the tympanic plexus, which control the middle ear.
Thus, impaired signalling through these nervous pathways may alter the position of the ossicles (via the tensor tympani and stapedius muscles), endolymphatic regulation (via the endolymphatic sac), pressure regulation of the tympanic cavity, and thus also tension and mobility of the tympanic membrane. Based on this information, one may start to understand why so many tinnitus sufferers feel that their jaw is an important piece of the puzzle!
TMD may, of course, also be responsible for a whole lot of other symptoms, which are outside the scope of this article. Read my TMD article which is linked at the end of this section.
Fig. x
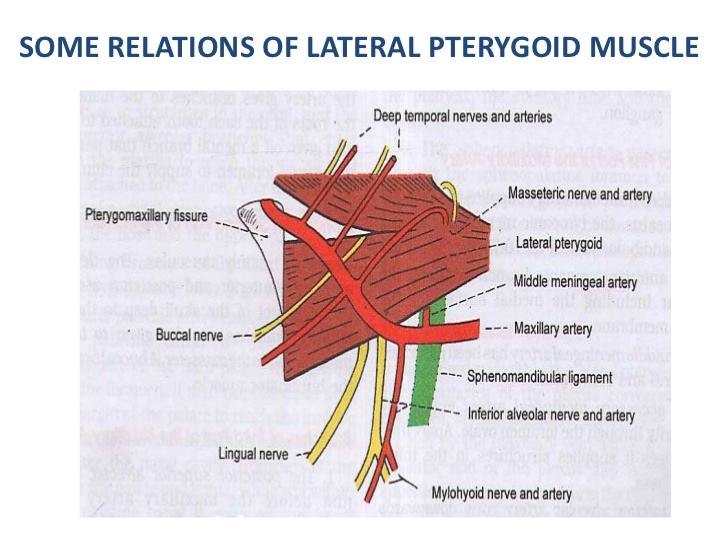
Subsequently, as the mandible is resting and moving in more or less constant excessive retraction, this will inhibit the lateral pterygoids (which perform mandibular protraction / contralateral deviation), and cause them to atrophy. This is a problem if left unaddressed, because the pterygoids are extremely important for healthy TMJ mechanics, as they prevent excessive posterior translation of the mandibular condyle and thus also joint shearing.
Such muscular dysfunction would certainly affect the discomalleolar ligament, which is once again attaches to the malleus via the upper head of the lateral pterygoid and retrodiscal tissue (if present). However, we also need to be aware that additional branches of the trigeminal nerve pass through the lateral pterygoids, the buccal and lingual nerves. These nerves may become entrapped within the weak muscle’s fibers, contributing to the dysfunction.
It is well known that many tinnitus sufferers as well as others suffering from auditory disorders, can alter their perception of sound by moving the mandible around. This movement generally involves using the pterygoids, as the mandible is already stuck in retraction (i.e. there’s no where else to go than forward), which may offer an explanatory mechanism as to why this occurs. It also involves movements which may intermittently compress or decompress the auriculotemporal nerve.
With regards to pulsatile tinnitus, there is a consensus that vascular irregularities are the main cause of this issue. I have often found that strengthening the lateral pterygoids may reverse this condition (of course, if other serious pathologies have been excluded, such as tumors and aneurysms). The reason for this is that the maxillary artery may become compressed within the two heads of the lateral pterygoid, and when it does, blood pressure and flow will increase through the proximal branches (such as the anterior tympanic artery, which supplies the cochlea) as there is partial occlusion distally. It has also been postulated that the anterior tympanic artery may become compressed by the mandibular condyle, but in my experience, the compression of the maxillary artery within the pterygoids is more common. It should be mentioned that the maxillary artery also supplies the eustachian tube, but it is unclear whether or not the E.T. would be significantly affected.
Fig. x
Treatment of the temporomandibular joint involves strengthening the pterygoids, teaching the mandible to open with protraction rather than retraction, and moving it forward in posture, all to decompress the joint and nerves. It is also important to address the neck, which I’ll get to next. You can, however, read more in-depth information about TMD, its mechanisms and treatment in my TMD article. Just scroll right down to the “Correction” section if you only want to learn what to do to treat it. You can find the temporomandibular joint disorder article here.
If treatment of the pterygoids, or for that matter, if there are no indicators for TMJ implication in the patient’s tinnitus problem, then an MRA and MRV of the head and neck can be pursued. Venous sinus stenosis is a known cause of pulsatile tinnitus. Sigmoid sinus diverticulae, if reaching the vestibular chamber, can cause pulsatile tinnitus. Damage or aberrancy of the supplying arteries, such as an arteriovenous fistula or malformation, can cause pulsatile tinnitus. As can frank damage, such as a vertebral or carotid dissection, though much more sinister, and also rare. A plain MRI of the head along with TOF (“time of flight”, non-contrasted, computer-simulated flow sequences) MRV and MRA sequences for starters. Follow-up with contrasted MR or CT of either venous or arterial phases can be done if something more specific needs to be evaluated.
There is debate over the factual existence of the DML due to the variation of its presence among specimens and/or the difficulty of dissection and visualization of the structure using modern imaging techniques. Loughner et al. (1989) found the ligament in only 15 out of 52 dissections; Rowicki and Zakrzewska (2006) observed the ligament by endoscope as a band of thickened, flaccid tissue in the posteromedial aspect of the upper joint compartment in only 4 out of 14 specimens. – Stevens-Sparks & Strain, 2014
Since the structures of the middle ear and the temporomandibular joint are derived from the first branchial arch or mandibular arch, they can be considered as being both anatomically and ontogenetically associated (Richany et al. 1956; Rodrıguez-Vazquez et al. 1993). In our study we consistently observed the existence of a very thin fibrous fascicle connecting the temporomandibular joint disc with the malleus of the middle ear. This structure is not described in anatomy textbooks (Sappey, 1867; Paturet, 1951; Crepy, 1967; Pelletier, 1969; Testut & Latarjet, 1975; Romanes, 1987; Rouviere & Delmas, 1987; Dubrul, 1990; Williams, 1995). It has been given a variety of names including discomalleolar band (Rees, 1954), ‘ tiny ligament’ (Pinto, 1962), discomalleolar ligament (Coleman, 1970), middle and inferior fascicle of the anterior ligament of the malleus (Toledo Filho et al. 1985) and articular portion of the anterior ligament of the malleus (Cesarani et al. 1991).- Rodríguez-Vázquez et a., 1998
According to the author’s hypothesis, the lack of posterior support of the alveolar ridge led to mandibular vertical height loss which caused a slipping backward of the condyles over the articular disc thus resulting in TMJ discal damage, erosion of the glenoid fossa bone, compression of the Eustachian tubes and tympanic plates and consequent impingement of the auriculotemporal nerve (ATN), which runs on the postero-medial aspect of the TMJ capsule, and chorda tympani nerve4 . – Paparo et al., 2008
When the maxilla and mandible do not achieve their genetic potential in length, width, or vertical position, the effects are seen in mal-relationships and dysfunctions in the patient’s tissues, bones, muscles, and nerves. The temporomandibular joint (TMJ) relationship may then become compromised when this occurs, as it compensates for the discrepancies in normal growth and development. Normal spacing between the roof of the glenoid fossa of the temporal bone and the condyle of the mandible should be approximately three mm to support the disk between them. The retrodiskal tissues originate from the distal portion of the glenoid fossa and are inserted into the posterior portion of the disk. This tissue contains a matrix of blood vessels and nerves, particularly fibers of the auriculotemporal nerve, cranial nerve V, an afferent branch of the trigeminal nerve. If this space is insufficient or reduced or restricted and the condylar head grows posterosuperiorly or is iatrogenically repositioned posteriorly or posterosuperiorly, the condyle will pinch this tissue and usually the result will be pain. – Sims & Stack, 2007
This case demonstrates that reversal of flow in the occipital artery may be an important cause of pulsatile tinnitus. Flow reversal in an aberrant occipital artery secondary to a carotid stenosis was rectified, leading to complete cessation of subjective and objective tinnitus. – Cowley et al., 2009
When a primary otologic cause is discarded in the diagnostic workup for tinnitus, vertigo, hypoacusis, hyperacusis, ear pain, or sensation of occluded ear, TMD may be the cause of these symptoms. Among patients with this dysfunction, the prevalence of ear pain, tinnitus, and dizziness varies between 33 and 76%.25 – de Moraes Marchiori et al., 2014
This study was undertaken in a retirement town, and the mean age of these TMD study patients was a mature 49.1 years. The data likely underrepresent the occurrence of TMD in younger adults. In the Figure, the statistical mode in the study group was 40 to 49 years; it was 60 to 69 years in the control group. The older control group would be expected to have an increased prevalence of recruitment hyperacusis, tinnitus, hearing changes, disequilibrium, and dysesthesias because these conditions increase with age. – Cox, 2008
50 patients were subjected to complex examination. In bite lowering the head of the condyle is displaced backwards and upwards into the depth of the glenoid fossa. The pressure of the displaced mandibular joints upon the arterial cord and the tympanic vein as well as upon the venous network around the mandibular joint capsule may produce disturbed blood supply to the mucosa of the middle ear and of the auditory tube, and finally, obstruction of the auditory tube. Disturbances in the blood supply of the middle ear irritate the tympanic cord and tympanic plexus, which causes burning of the tongue, taste and salivation troubles, and also ear complaints. Since the sympathetic fibres of the tympanic plexus and of the eye are closely interrelated, this leads also to an irritation of the dilator muscle of the pupil. The reflectory irradiations from the tympanic plexus and mandibular joint explain many other neurologic symptoms. In bite lowering these symptoms are not always associated with joint disturbances. – Chwatowa & Kurljandsky, 1977
It has been stated that when a pathological process occurs around the temporomandibular joint, the auriculotemporal nerve and the anterior tympanic artery can be involved into this process. This can produce appearance of the “Costen syndrome” components. – Mikheev & Tsybul’kin, 1988
The syndrome of symptoms (Table 1) as first described by Costen, an American otolaryngologist, was discussed. Costen attributed the symptoms to temporomandibular joint dysfunction consequent upon mandibular overclosure with distal condylar displacement. He assumed that the displaced condyle might lead to any of the following: Compression of the eustachian tube, erosion of the glenoid fossa or tympanic plate, pressure on the chorda tympani, or pressure on the main trunk of the auriculotemporal nerve. – Clarke, 1962
posteriorly translocated mandibular head (due to missing teeth, pathological teeth attrition, or trauma) may compress the tympanic artery and vein, leading to blood supply disorders within the middle ear and constituting an important cause of hearing disorders. At the same time, compression by the articular head may damage the tympanic cord, leading to contracture of the stapedius muscle in a reflex mechanism transmitted via the facial nerve. In addition, the course of the auriculotemporal nerve in the temporomandibular joint region promotes its compression by the mandibular head, generating an impulse for reflexive contracture of the tensor tympani muscle and leading to hearing impairment or tinnitus symptoms. Anatomical fissures between the articular cavity and the middle ear, such as petrotympanic or petrosquamous fissures, are routes for transmission of inflammatory infections. Another possible reason for the concomitance of both types of symptoms is the transmission of excess mechanical forces by the discomalleolar ligament or direct compression on the auriculotemporal nerve [3, 4]. – Ferendiuk et al., 2014
Constant stimulation of the auriculotemporal nerve (CN V) may then result in the stimulation of CN’s V, VII, IX, X, via crossover interneurons (ephapses) and other neural elements in the reticular formation. All of these nerves are intimately involved with movement disorders. In summary, we find that chronic noxious input via the auriculotemporal nerve causes reflex reactions with CN’s V, VII, IX, and X via the crossover pathways at various segmental levels within the spinal cord. All patients showed a total discontinuance of their movement disorders immediately. All patients stated that their breathing was improved and better. All patients stated they did not have the urge to tic or make their involuntary movements. An upper appliance was made for the seven-year-old patient and again, the movement disorder ceased. – Sims & Stack, 2007
We surveyed 1032 patients: 338 had TMD and 694 served as two age-matched control groups. Tinnitus and vertigo symptoms were significantly more prevalent in the TMD group than in either of the control groups. – Chole & Parker, 1992
A few cases of tinnitus have been relieved temporarily by novocain block of the auriculotemporal nerve. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus
TMD patients with coexisting tinnitus report 46 to 96 percent have tinnitus improvement or resolution from TMD therapy (Table 1).9-15 A survey taken two years after TMD therapy suggests the tinnitus improvement is sustained over time – Wright & Bifano, 1997
The findings indicate that TMD patients with otological complaints have hearing impairment at low frequencies and also perhaps, at high frequencies. – Pekkan et al., 2010
As can be seen, the TMJ is a small compacted structure with vascular and neurological tight components that can easily be injured during TMJ disorders. Ash & Pinto reasoned how the otic symptomatology can be generated by injury of the parasympathetic nerve fibers of the auriculotemporal nerve that travel from the otic ganglion and tympanic plexus (glosopharyngeal nerve). When irritated can produce a reflex vascular spasm in the labyrinthine system secondary to abnormal stimulation of these fibers. (Kopp, 2001). The irritated auriculotemporal nerve can produce otalgia because it profusely innervates articulation as well as the tympanic membrane, the anterosuperior zone of the external ear, the tragus and the external part of the ear among other structures that can explain the auricular pain experienced. (Fernández et al., 2003 and Schmidt et al., 1998). Johansson explained that in the nerve entrapment etiology (auriculotemporal nerve) is important not only to anatomical mobility and bone deformities but also inflammation of vascular and muscular structures that can injure closely situated nerves since inflammation can alter and reduce the normal contour and size of the anatomical passages. Loughner et al. (1990) confirmed that during lateral pterygoid spasm and hypertrophy, it can injure auriculotemporal nerve – Ramirez et al, 2005
Temporomandibular disorders are associated with symptoms such as tinnitus, vertigo, sensation of hearing loss, ear fullness and otalgia. The connection and dysfunction of the tensor tympani and tensor veli palatini muscles seems to be associated with the aforementioned symptoms. – Ramirez Aristeguieta et al., 2010
Pain, stuffiness, and tinnitus may have a musculoskeletal etiology.29-34 Mandibular posture related to the maxilla affects the masticatory elevator muscles. The medial pterygoids are intimately related in the left-to-right balance of the mandible on tooth closure. The tensor tympani and tensor palatini are actually one muscle with a raphe that wraps around the hamular notch of the maxilla. Improper growth of the maxilla during development may affect eustachian tube function and contribute to middle ear infections in children and stuffiness and changes in ear pressure in adults. – Mehta & Spierings, 2014
Symptoms consistent with TTTS can include: a sharp stabbing pain in the ear; a dull earache; tinnitus, often with a clicking [11,12], rhythmic or buzzing quality; a sensation of aural pressure or blockage [8,9] tympanic flutter [13] pain/numbness/burning around the ear, along the cheek and the side of the neck; [7,8], mild vertigo and nausea [8,9]; a sensation of “muffled” or distorted hearing [14] and headache. Central pain sensitization can develop from chronic trigeminal neuralgic TTTS-induced pain. Tensor tympani spasm has been implicated in a range of conditions including Meniere’s disease, for which sectioning of the tensor tympani muscle has been a suggested treatment [15,16] and the secondary otologic symptoms, such as tinnitus, ear pain and other symptoms in and around the ear, which can develop in myofascial pain syndrome [16,17] temporomandibular disorder (TMD) and TMJ dysfunction [8,9,18,19]. – Westcott et al., 2016, Hyperacusis-induced Pain: Understanding and Management of Tonic Tensor Tympani Syndrome (TTTS) Symptoms
TMD patients often have associated complaints. Many of these patients complained of masticatory fatigue (40%), stiffness (20%), swelling (12%), and weakness (18%) in spite of no observable cranial nerve deficit. Otologic symptoms are also commonly reported among TMD patients. Many of these patients reported tinnitus (42%), ear pain (42%), dizziness (23%) and diminished hearing (18%). – Wright & Bifano, 1997
The cervical complex
The cervical complex is complicated, because the regions for potential problems are many, and the treatment is difficult as well. I will try to give a detailed description of the potential mechanisms for auditory impairment. The treatment, however, and as mentioned, will only briefly be discussed, but can however be read in detail in linked articles.
Impaired neural signaling
The cervical region has several definite influences on the aural complex through innervation, because of the potential for entrapment of the cervical, brachial and sympathetic plexuses, along with the vagal nerves. I will describe each of these entrapment sites in detail, repeat its relation to the ear.
As I mentioned priorly, a lot of patients develop hearing disorders post whiplash and similar injuries. Reasonably, a hyperextension injury is more likely to trigger tinnitus, as most of the susceptible tissues lie on the ventral side, except for the cervical (Cruveilhier’s) plexus, on the dorsal side. However, general neck pain is also associated with tinnitus, and the reason why is similar to that of injury.
Studies show that the cervical musculature degenerates in patients with whiplash. In general chronic neck pain, studies are somewhat more conflicting. However, my own clinical experience leaves no single doubt that the cervical musculature also atrophies (perhaps without fatty infiltration, as with whiplash patients) and is extremely weak. As I’ve talked about in numerous articles and other posts, weak muscles cause pain and irritate nerves, not strong muscles, which is why it’s critical to understand that when nerve entrapment is detected, the responsible muscles require strengthening. Of course, the cause of the muscles’ detriment will require identification and addressment as well, which usually implies postural factors and correctives to get them out of the position that inhibits certain structures (read more about this, especially about the cervical ‘hinge’, in my neck pain article).
And, once again, we also need to be aware that nerve irritation spreads out to other structures, as mentioned earlier. I reiterate this because it is crucial to understand, in order to connect the dots.
Fig. x
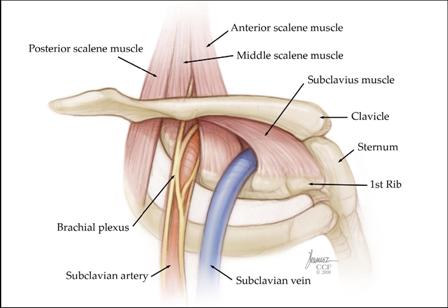
Now, let us talk about these entrapment sites, and we can start with the well known brachial plexus.
Many are aware that the brachial plexus may become entrapped between the anterior and medial scalene muscles, which is also known as the interscalene space. What is not often spoken of, however, is that the sympathetic chain is connected to each of these nerve roots via the ramus communicans, which are communicating branches between the spinal nerves and autonomic nerves. Studies have shown that severe TOS (thoracic outlet syndrome) patients may develop autonomic disorders such as pseudoangina, atrial fibrillation, and chest for instance. These mechanisms are, of course, very controversial and poorly undestood, as you can read more about in my thoracic outlet syndrome article. Thus, thoracic outlet syndrome may affect the sympathetic chain, i.e. cervical ganglia plexus.
Now, a common cause of TOS is hyperextension whiplash injuries, as the scalenes become injured, atrophy, and thus entrap the nerves. Another very common cause is ‘neck hinging’, as hinging at the neck, which you can read more about in both my TOS and neck pain articles, will cause a tremendous inhibitory reaction to occur in the cervical spine, due to instability. Instability of the neck (either caused by hinging or by injury) will prevent the muscles from activating properly, thus potentially leading to a very evil circle of dysfunction. Muscle injury or poor posture, and even stress, may all lead to muscular dysfunction and atrophy. Atrophy, once present, exacerbates the poor posture, which furthers the potential for problems.
Whatever the cause, be it neck hinging, whiplash or similar; as the muscles gradually weaken, the greater the potential for nerve entrapment and subsequent dysautonomia, such as tinnitus, hearing loss, etc.
The rami communican nerves connect the spinal nerves to the sympathetic plexus, as I explained. However, the sympathetic plexus also reside between the alar fascia of the neck and the longus colli and longus capitis muscles. These muscles are virtually always injured in whiplash type incidences, but may also atrophy in poor postures. In some circumstances, it may be entrapped (varying in severity) between the alar fascia and the weak longus colli & capitis muscles. Thus these nerves are susceptible to a ‘double crush’ nerve entrapment, both indirectly by TOS and directly in the ventral cervical spine.
Fig. x
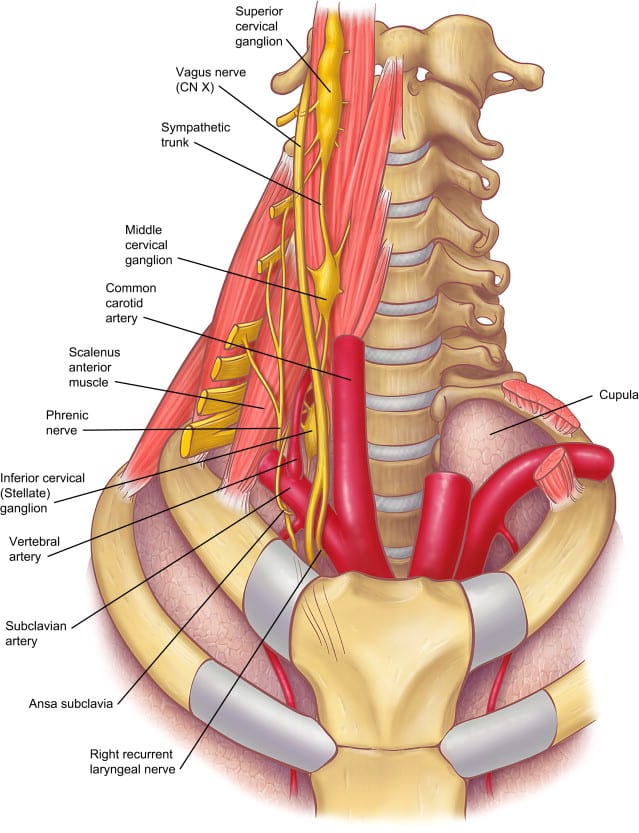
The sympathetic cervical plexus wraps around the internal carotid artery and branches off from it, into the tympanic cavity, where it along with other nerves form the tympanic plexus. If you remember, the glossopharyngeal nerve also adds to the tympanic plexus, and this nerve has a very intimate relationship with the vagus nerve. Also, between the anterior scalene muscle and the clavicular portion of the sternocleidomastoid, lies the vagus nerve. The vagus nerve may become entrapped between these muscles. Because these nerves innervate the organs, all kinds of weird and seemingly unrelated symptoms may occur, although outside the scope of this article.
As you may remember, the sympathetic and parasympathetic nerves innervate or partly innervates the tympanic cavity’s & eustachian tube’s muscosal transport mechanism, the tympanic membrane, cochlear fluid regulation via the stria vascularis, the endolymphatic sac, and vestibular arteries. The vagus nerve also innervates the salpingopharyngeus and levator veli palatini muscles, which aid in opening the eustachian tube. Studies show that stimulus of some of these nerves may alter blood flow to the cochlea, as well as other regulatory mechanisms.
Fig. x
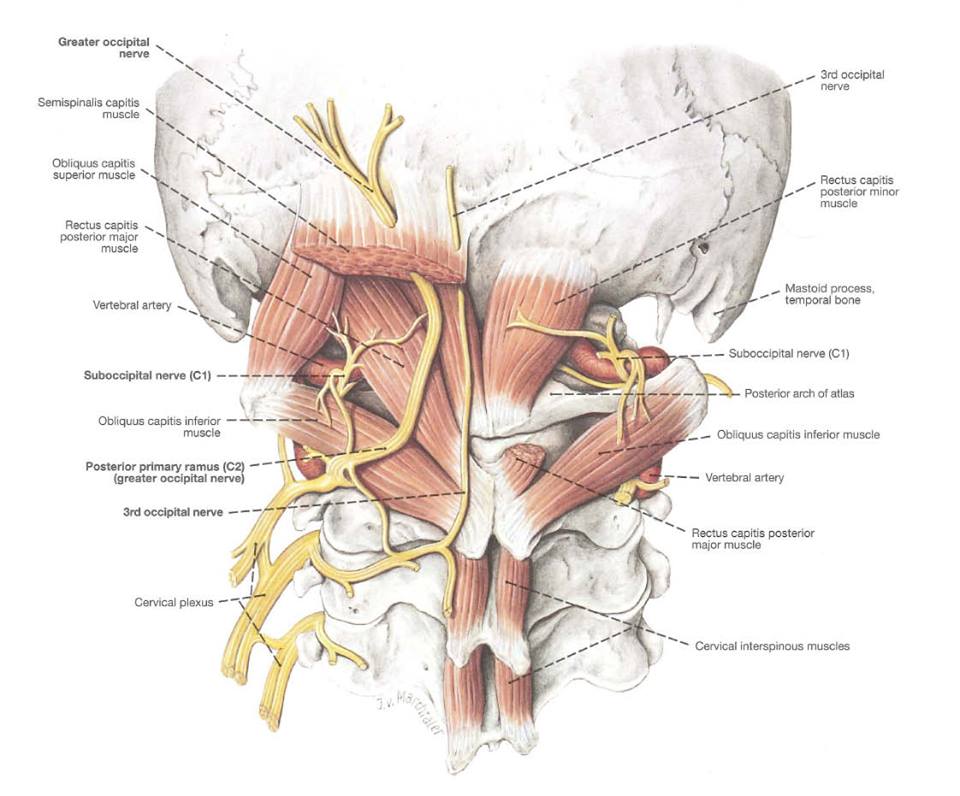
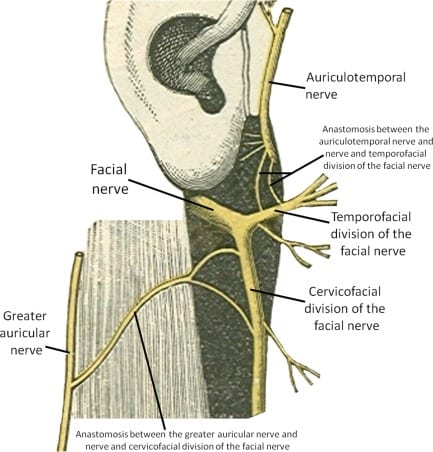
On the dorsal side, we may find the cervical plexus, which is also known as the Cruveilhier’s plexus. These are the dorsal rami nerve bundles originating from the C1 to C3 nerve roots. The main branches of this nervous network include the greater and lesser occipital nerves, suboccipital nerves, third occipital nerve, as well as the anterior and posterior auricular nerves. The cervical plexus’ roots and/or branches anastomosis (connection) with the cervical sympathetic plexus, the hypoglossal nerve, accessory nerve,vagus nerve, and the facial nerve, and may thus have great influence on the aural complex.
The below illustration shows how the greater auricular nerve is connected to the ‘TMJ nerves’ (i.e. the auriculotemporal nerve) through anastomosis via the facial nerve. Again, all of these nerves have great influence on both the auditory and vestibular systems.
The upper cervical spine is susceptible to injury, especially post whiplash and similar. It is also often problematic in moderate to severe chronic neck pain sufferers. The most common problem that develops in this regard is atrophy of the musculature. Once the muscles atrophy, their work capacity become extremely limited, and may inflame even in when exposed to very low work loads. In turn, the cervical plexus which pierce these muscles may become entrapped.
The nerves’ course vary somewhat anatomically, but generally, some of them pierce the suboccipitals, semispinalis capitis and trapezius muscles. Sometimes it may also pierce the sternocleidomastoid. Thus all of these muscles will require strengthening, and the neck posture needs to be optimized.
Fig. x
As mentioned initially, and I’ll also come back to this later on, the treatment is based on strengthening the muscles which are in contact with the nerves, as well as optimizing postural patterns. For this section, we are especially talking about the trapezius, sternocleidomastoid, suboccipitals, scalene complex, longus colli and longus capitis muscles. The atlas joints may also addressing, which is outside the scope of this article. Furthermore, the patient needs to learn to be ‘long in the neck’, i.e stop hinging at their neck, and stop dropping down their shoulders, as this exacerbate the muscular dysfunction.
Contraction of the smooth muscle cells in the spiral modiolar artery is hypothesized to be tightly regulated to meet the demand of cochlear tissues (Wangemann, 2002b). Contraction of the smooth muscle cells of the vascular wall reduces its luman diameter with the effect of decreasing blood flow, while relaxation of the smooth muscle cells increases blood flow. Smooth muscle cell contractility is signaled both with central neural and local metabolic signals. Sympathetic (peptidergic and adrenergic) nerve fibers have been found in the spiral modiolar artery of the gerbil and guinea pig (Brechtelsbauer et al., 1990; Carlisle et al., 1990; Rauchegger et al., 1981). Norepinephrine-induced vasoconstriction in the spiral modiolar artery is mediated by α1A-adrenergic receptors (Gruber et al., 1998). Stimulation applied in the sympathetic ganglia, stellate ganglion, or superior cervical chain in the guinea pig has been shown to alter CoBF (cochlear blood flow) in situ (Laurikainen et al., 1994; McLaren et al., 1993; Ren et al., 1993). In addition, distribution of vasoactive intestinal peptide (VIP), neuropeptide Y (NPY), substance P (SP), and calcitonin gene-related peptide (CGRP) are also found in the spiral modiolar artery (Carlisle et al., 1990; Qiu et al., 2001). These findings support a hypothesis that CoBF is controlled by neuronal signals at the level of the artery (Gruber et al., 1998; Herzog et al., 2002; Sadanaga et al., 1997; Scherer et al., 2005; Wangemann, 2002b; Wangemann et al., 1998; Wonneberger et al., 2000). – Shi, 2011
Vestibular dark cells and strial marginal cells are regulated by purinergic-, adrenergic-, and muscarinic receptors, steroids, vasopressin and atrial natriuretic peptide (ANP). There is evidence that the stress hormones noradrenaline and adrenaline, corticosteroids, and mineralocorticosteroids possess a key role in inner ear homeostasis and sensory transduction (Table 7). – Ciuman, 2013
I have had two cases in whom a mere novocain block was sufficient to stop the tinnitus permanently. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus, 1951
Tinnitus.-16 cases in which tinnitus was the predominating symptom were examined and 13 were subjected to sympathectomy and one to removal of Meckel’s ganglion (sphenopalatine ganglionectomy through the posterior wall of the maxillary antrum). Results Temporarily Obtained by Novocain Block of Sympathetic Partial relief: 8 Complete relief: 5 Unaltered: 3 After local anesthetic was applied to the facet joints, patients reported within 10 minutes that their tinnitus had diminished significantly. Simultaneously, mydriasis disappeared. In one patient, tinnitus was controlled completely. Tinnitus can temporarily be reduced by the application of local anesthetic to Cl-C2 facet joints and buprenorphine analgesia of the superior cervical ganglion in patients with Cl-C2 facet joint disorders. – Franz et al., 1998
Consistent with previous evidence, muscle degeneration occurs soon after injury but only in those patients with poor functional recovery. – Elliott et al., 2016
The findings showed higher levels of global muscle fatigability and smaller size of deep neck extensor muscles in CNP patients. Disability and extensor endurance were found to be associated with extensor muscle size. – Kahlaee et a., 2017
Structural changes such as higher concentration of fat within the muscle, variable cross-sectional area and higher proportions of type II fibres have been observed in the deep cervical extensors of patients with neck pain compared to healthy controls. – Schomacher & Falla, 2013
All otologists are familiar with the clinical signs of deafness, giddiness and tinnitus, which are associated with herpes of the geniculate ganglion. I feel that its direct influence on the cochlea and labyrinth has been greatly neglected. We are hoping to carry our research further with this ganglion. – Garnett Passe, Sympathectomy in Relation to Meniere’s Disease, Nerve Deafness and Tinnitus, 1951
Chronic subjective tinnitus of a 20 years duration completely disappeared within 4 weeks with an intermittent short time application of CC. Thereafter, tinnitus was deliberately again induced by head inclination, set on with anterior tilt of 14°, reaching maximum strength by 23°. Tinnitus stopped with return to neutral head position. – Bechter et al., 2016
The vestibular sympathetic fibers were examined in 20 guinea pigs by the immunohistochemical demonstration of tyrosine hydroxylase and dopamine B-hydroxylase. The vestibular sympathetics originated in the ipsilateral superior cervical ganglion and entered the internal auditory meatus along the labyrinthine artery. At the Schwann–glial border, some of the sympathetic fibers left the artery and went into the superior and inferior divisions of the vestibular nerve and formed a loose meshwork among the Scarpa’s ganglion cells, while other fibers continued to follow the labyrinthine artery. Both groups of fibers entered the cristae ampullares and saccular and utricular maculas after several bifurcations in the cribrose areas and terminated either near the capillaries beneath the sensory epithelia or among the vestibular nerve fibers. These fibers traveled freely in the vestibular labyrinth without being restricted to following blood vessels or vestibular nerve fibers. Some sympathetic fibers made direct contact with the vestibular efferent fibers or the vestibular afferent fibers at the node of Ranvier. Sympathetic fibers were not observed in the sensory epithelia or semicircular canals, and were rarely found in the vicinity of the dark cells. – Hozawa & Kimura, 1989
All adrenergic nerve fibres consisted of postganglionic axons from the ipsilateral superior cervical ganglion. In rabbit, postganglionic nerve fibres passed via the carotic plexus. Probably because of the anatomical difference, the feline internal carotic artery being rudimentary, all sympathetic nerve fibres to the inner ear in cat passed via the tympanic plexus. In the vestibular ganglion there was a uniform distribution of adrenergic nerve fibres and there was no difference in distribution patterns between rabbit and cat. There was a continuous blood vessel innervation and an innervation independent of blood vessles. – Densert, 1975
Symptoms of cervical spine disorders, such as head and neck/shoulder pain, were all significantly more frequent in the patient group than in the control group. Most of the patients (75%) reported a strong association between head neck movements in the atlanto-occipital and atlanto-axial joints and triggered attacks of vertigo. Also, 29% of the patients could influence their tinnitus by mandibular movements. Signs of cervical spine disorders, such as limitations in side-bending and rotation movements, were significantly more frequent in the patient group than in the control group. Tenderness to palpation of the transverse processes of the atlas and the axis, the upper and middle trapezius, and the levator scapulae muscle were also significantly more frequent in the patient group. The study shows a much higher prevalence of signs and symptoms of cervical spine disorders in patients diagnosed with Meniere’s disease compared with control subjects from the general population. – Bjorne et al., 1998
Compression of the sympathetic nerves in the thoracic outlet may occur alone or in combination with peripheral nerve and blood vessels. The sympathetics are intimately attached to the artery as well as adjacent to the bone. They may be compressed or irritated in primary or recurrent TOS. Atypical chest pain (pseudoangina) simulates cardiac pain (48). Major indications for dorsal sympathectomy include hyperhidrosis, Raynaud’s phenomenon or disease, causalgia, SMPS, reflex sympathetic dystrophy, and vascular insufficiency of the upper extremity. – Urschel & Kourlis, 2007
Vascular insufficiency
Another potential cause of degeneration of the stria vascularis, is vertebrobasilar insufficiency. I can say right away that I do not consider this a very common cause, especially because there seems to be plenty of fluid in the endolymphatic canals (suggesting, at least seemingly, that there is adequate nutritional influx via arteries & CSF), but it is still important enough to be mentioned.
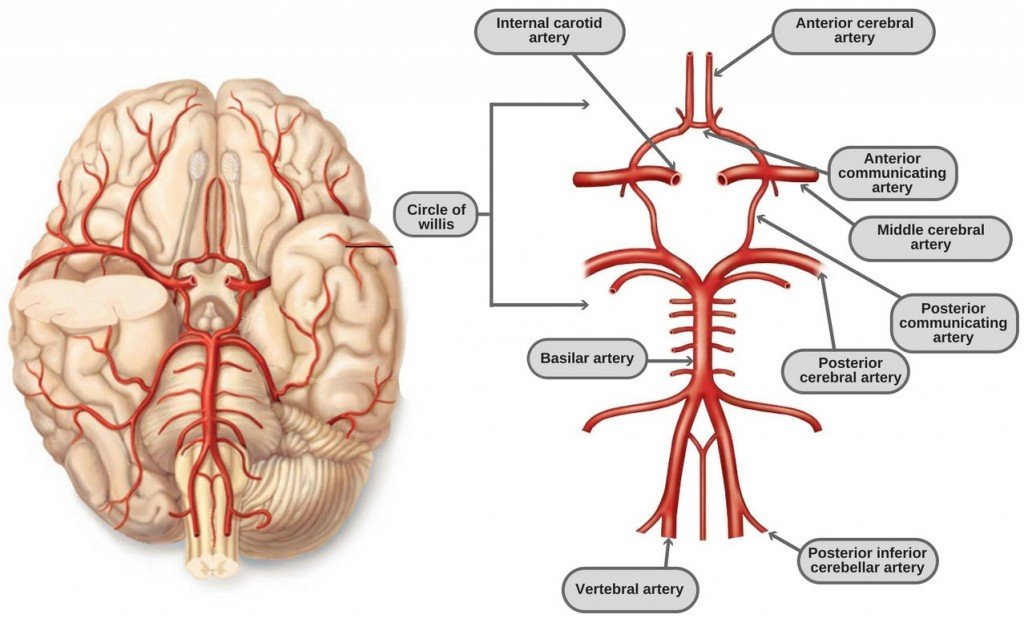
The labyrinth and cochlea are both mainly supplied blood via the labyrinthine artery, which branches off the basilar artery. It also has a minor supply occipital and ascending pharyngeal arteries, as shown below. The maxillary artery, as discussed in the TMJ section, may become compressed within the pterygoid muscles, but this will cause increased inflow via the anterior tympanic artery rather than ischemia.
Fig. x
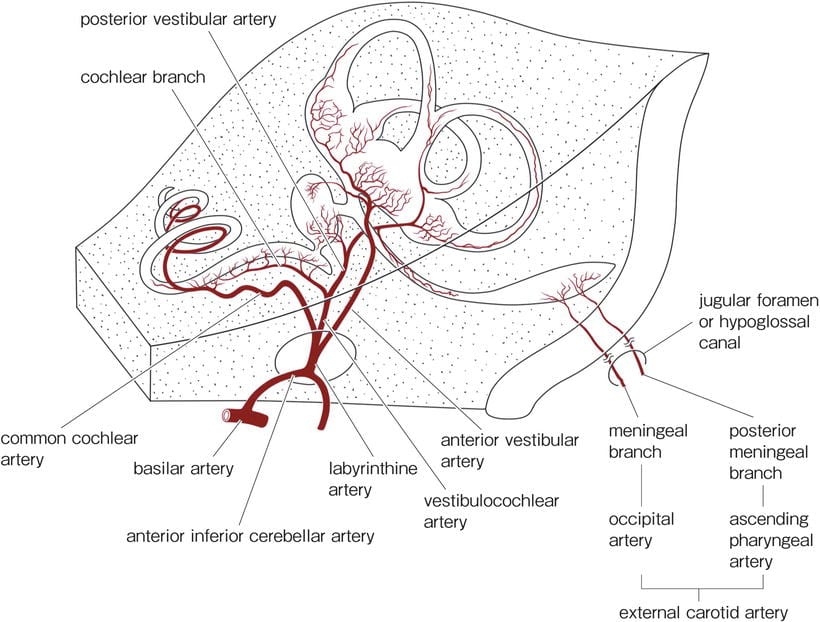
The basilar artery, however, which is formed by the vertebral arteries posteriorly, is the main supplier of the vestibulocochlear complex. It has been shown that bilateral occlusion of the vertebral arteries may cause ischemia of the stria vascularis, and consequent hearing loss.
It is claimed that, because the circle of Willis connects the two sides, a bilateral occlusion is necessary to cause ischemia. However, there are studies that show e.g. blindness in relation to intermittent occlusion of just one vertebral artery in TOS patients. It has also been noted that in transcranial sonography, the circle of Willis may sometimes be separated, as an anatomical anomaly (Pellerito & Polak, Introduction to Vascular Ultrasonography 6th Edition, 2012). Thus, one can not definitely say that there must be a bilateral occlusion of the vertebral arteries to cause hearing disorders, or at least influence hearing.
Fig. x – Vertebral artery
I briefly mentioned TOS above, in relation to vertebrobasilar insufficiency. It is not well known, yet very real, that thoracic outlet syndrome (TOS) may also cause partial, or in extreme circumstances, complete occlusion of the vertebral arteries (usually unilaterally), as in the mentioned blindness case above (Sell, 1994), and in other less conspicuous cases which you may read more about in my TOS article. The point, however, is that vascular (as well as neurogenic) TOS may contribute to hearing disorders. Subclavian steal which is caused by subclavian stensosis may also cause compromised flow in the vertebral artery, although this is much more likely to be detected by typical examinations.
Within the vascular sonographic community, it is well known that vascular TOS (although generally controversial elsewhere, and ignorantly claimed to be extremely rare), is a very common finding. My personal experience is that TOS, especially neurogenic TOS, is extremely underreported, as there are no good diagnostic criteria, not to mention no consensus with regards to treatment. I have seen patients with TOS so severe that putting them in the vertebral artery dissection (DeKleyn’s) test position, led to symptoms of stroke! Upon CT angiography, no damage to the vessel nor stenosis was found; it was ‘mere’ TOS.
Treatment of vascular thoracic outlet syndrome involves optimizing cervical and scapular postures, along with strengthening the scalene complex and spinal stabilizers such as the longus colli and longus capitis. Read more about this in my thoracic outlet syndrome article.
Normally functioning cochlear microcirculation is critically important for maintaining ion and fluid balance in the inner ear, as sensory hair cells are strikingly vulnerable to ischemia (Nuttall, 1999b; Wangemann, 2002b). The inability to measure cochlear blood flow (CoBF) in humans has limited the investigation in human subjects, but numerous studies using different animal models have aptly demonstrated physiological changes with the alteration of CoBF, including changes in leukocyte dynamics. Vascular permeability and deformation have been shown to be contributing factors in various hearing disorders including presbycusis, noise-induced hearing loss, and ear hydrops (Brown et al., 1995; Chen et al., 2005a; Gratton et al., 1996a; Gratton et al., 1997; Hawkins, 1971; Kellerhals, 1972; Lamm et al., 1998; Mazurek et al., 2006; Miller et al., 2003; Nuttall, 1999a; Ohlemiller, 2009; Prazma et al., 1990; Seidman et al., 1999a; Shi et al., 2003). Capillary and stria vascularis degeneration have also been shown in presbycusis patients (Nelson et al., 2006; Wagenaar et al., 2000). One mechanism for hearing loss is disruption of the vascular barrier in the stria vascularis (Cadoni et al., 2002; Fattori et al., 2001; Naarendorp et al., 1998; Ottaviani et al., 1999), with subsequent loss of endocochlear potential (Lin et al., 1997; Ruckenstein et al., 1999). – Shi, 2011
Over the past 15 years, we have investigated the mechanisms of ischemic-induced hearing loss using a gerbil model of transient cochlear ischemia. In the gerbil, cochlear ischemia can be induced by occluding the bilateral vertebral arteries simultaneously at the neck, because the posterior communicating arteries of the Circle of Willis close spontaneously around 1 mo after birth. When 15 min ischemia was loaded on this animal, permanent hearing loss of about 25 dB and the death of hair cells, especially inner hair cells were induced. – Kiyofumi, 2012
The number of vessels in the stria vascularis in ears with Ménière’s disease was smaller than in normal controls in all cochlear turns. The number of vessels in the contralateral stria vascularis in patients with unilateral Ménière’s disease was smaller than in normal controls in all cochlear turns. There was no significant difference between the area of the vessel lumen in the stria vascularis in patients with Ménière’s disease and that in normal controls. – Kariya, 2009
Vestibular function studies were performed in 20 children with symptoms suggesting basilar artery migraine. Sixteen children had abnormalities on bithermal caloric testing. Labyrinthine preponderance was found in 1 child with labyrinthine concussion and in 6 children with symptoms suggesting ischemia of the territory supplied by the basilar artery and the occipital branches of the posterior cerebral arteries. Directional preponderance was found in 4 children with symptoms suggesting ischemia of the posterior temporal branches of the posterior cerebral arteries. Five children had both labyrinthine and directional preponderance. normal electronystagmographic findings were present in 4 children and correlated clinically with a milder illness. Head trauma was the triggering factor for the migraine in 5 children. – Eviatar, 1981
Thoracic Outlet Syndrome (TOS) causes dizziness because of positional compression of the vertebral artery with resultant symptoms of vertebrobasilary insufficiency. Compression of 7,C8,and T1 nerves fibers is responsible for the neck pain. – Selmonosky, 2007
Subclavian steal symptoms presents secondary to arterial insufficiency, created by a retrograde flow that “steals” blood from the brain circulation, more specifically from the basilar artery via the vertebral artery. Classically it presents with neurological symptoms from the posterior brain and cerebellum [4,6]. Decreased flow over the basilar artery gives rise to symptoms like lightheadedness, ataxia, vertigo, dizziness, confusion, headache, nystagmus, hearing loss, presyncope and syncope, visual disturbances, focal seizures, and in extremely rare cases, death [6–10]. However the vast majority of patients are asymptomatic and rarely require any intervention [3,5,11]. – Alcocer et al., 2013
This article describes migraine without aura since childhood in a patient with bilateral cervical ribs. In addition to usual migraine triggers, symptoms were triggered by neck extension and by arm abduction and external rotation; paresthesias and pain preceded migraine triggered by arm and neck movement. Suspected thoracic outlet syndrome was confirmed by high-resolution bilateral magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) of the brachial plexus. An unsuspected aberrant right subclavian artery was compressed within the scalene triangle. Left scalenectomy and rib resection confirmed the MRI and MRA findings; the scalene triangle contents were decompressed, and migraine symptoms subsequently resolved. – Saxton et al., 1999
Thoracic outlet syndrome (TOS) refers to the compression of the neurovascular bundle within the thoracic outlet. Cases are classified by primary etiology-arterial, neurogenic, or venous. In addition to the typical symptoms of arm swelling and paresthesias, headaches have been reported as a potential symptom of TOS. In this report, we describe a patient with debilitating migraines, which were consistently preceded by unilateral arm swelling. Resolution of symptoms occurred only after thoracic outlet decompression. Patients with migraines and concomitant swelling and/or paresthesias, especially related to provocative arm maneuvers, should be considered a possible atypical presentation of TOS and evaluated in more detail. – Chahwala et al., 2017
It is also noteworthy that the hypertrophied and contracted anterior scalenus muscle exerts a strong although intermittent compression of the vertebral artery, causing in severe TOS diverse symptoms that are very characteristic of vertebrobasilary insufficiency. – Silva & Selmonosky, 2011
Reports of transient blindness resulting from this condition are even more rare. The authors describe the case of a middle-aged woman who presented with transient blindness when she turned her head excessively to the left. She also exhibited other less severe brainstem symptoms. Arteriography demonstrated occlusion of the left vertebral artery only when her head was rotated to the left. Surgical exploration revealed entrapment of the left vertebral artery by a tight anterior scalene muscle, release of which resulted in complete resolution of her symptoms. – Sell et al., 1994
Leftward head rotations in a patient with a rotational vertebral artery occlusion syndrome elicited recurrent uniform attacks of severe rotatory vertigo and tinnitus in the right ear. These attacks were accompanied by a mixed clockwise torsional downbeat nystagmus with a horizontal component toward the right. – Strupp et al., 2000
Restricted venous drainage
Increased endolymphatic volume, which is termed endolymphatic hydrops when very volumous, has been greatly associated with tinnitus and other hearing disorders, as well as vestibular disorders. This section will explain why poor postures may be responsible for this occurrence, as it may compress the internal jugular vein and thus prevent normal venous drainage from the vestibulocochlear complex.
Firstly, it has been shown that excessive endolymphatic fluid volume within the scala media may cause so much pressure onto the stria vascularis that ischemia and cell death occurs, leading to hearing loss. Also, in endolymphatic hydrops, the pressure may become so high that the Reissner’s membrane ruptures, creating a fistula (i.e. abnormal connection / gateway) between the canals, and the endolymphatic fluid will drain into the perilymph canals. The sacculus and utricle of the vestibular labyrinth may also rupture from this pressure. As a result, the stereocilia (hair cells) may be destroyed, both in the labyrinth as well as in the cochlea, resulting in temporary or sometimes permanent damage.
An endolymphatic fistula may possibly, in some circumstances cause the perilymphatic chambers to, in similar fashion, also develop pressures that are so great that the oval window ruptures, and cause perilymphatic fluid to pour into the tympanic cavity. Oval window rupture has also been associated with head trauma and barotrauma of other origins, such as diving, so it is not always caused by endolymphatic fistulae. Therefore it is important to keep in mind that an ENT should exclude all typical aetiologies before considering differential diagnosis.
Fig. x
Although studies show that the Reissner’s membrane heals on its own, it may trigger an attack as it occurs, usually symptoms of vestibular and/or auditory nature. Furthermore, if there are constantly excessive levels of endolymphatic fluid, the Reissner’s membrane will have difficulty healing. Also, because the endolymphatic fluid has a high percentage of potassium and is very low in sodium, and the perilymphatic fluid a high percentage in sodium and very low in potassium, it will cause chemical imbalances in both the cochlea and the vestibular labyrinth. Endolymph is also higher in chloride than perilymph. Many patients feel that increased sodium intake makes their aural (and/or vestibular) disorders worse, but reasonably this should not be a problem unless the Reissner’s membrane has ruptured, implying that the sodium sensitivity is caused by communication between the endolymphatic and perilymphatic ducts.
Briefly, because both perilymph and endolymph is similar to cerebrospinal fluid (CSF), it has been proposed that disturbances in CSF may cause or influence the cochelar ducts. Studies, however, show that its influence is minor.
Endolymphatic hydrops, vestibular dysfunction and migraines
As we have seen already, there is little to no doubt that impairment of the respective nerves that innervate the inner ear may cause fluid imbalances such as increased endolymphatic production, however for the endolymphatic pressure to become so great that the Reissner’s membrane ruptures, it is reasonable to expect that additional, and perhaps greater forces are involved than ‘mere’ dysregulation of fluids, i.e dysregulation of neurogenic origin.
It is much more likely that a combination of reduced venous drainage and neurogenic dysfunction is causing the extreme buildup of endolymphatic fluids. Especially considering the vast amount of hydrops sufferers who also suffer from migraines. Let me explain:
The vestibulocochlear venous system drains into the sigmoid sinus, which proximally becomes the internal jugular vein. It has been shown that the internal jugular vein has reduced outflow in migraine patients. It has even been demonstrated by means of CT venography (see below), that the internal jugular vein may be compressed by the transverse process of the atlas vertebrae. Restricted venous outflow will cause craniovascular hypertension, and migraines. It may also restrict outflow via the vestibular and cochlear veins, quite possibly being responsible for the extreme buildup of endolymphatic fluids.
Fig. x
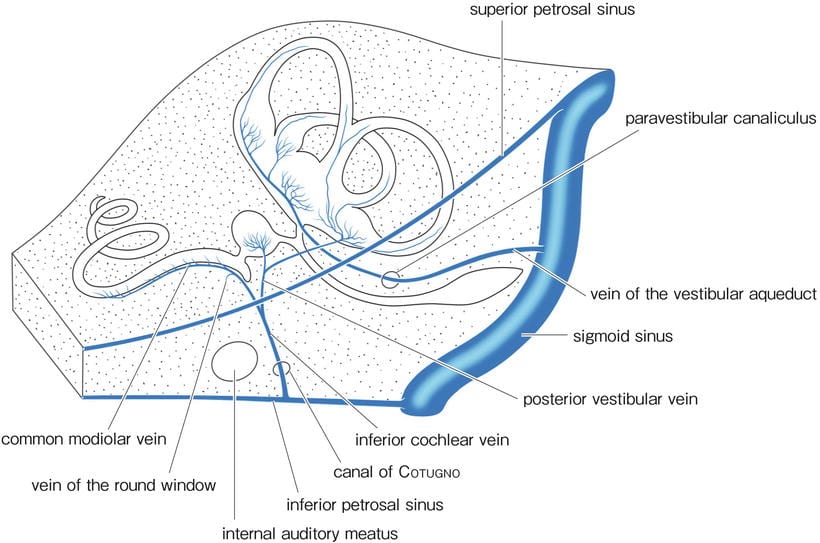
I performed a survey on a patients who have a high prevalence of endolymphatic hydrops (Meniere’s disease patients). This patients also have a very high prevalence of neck and jaw disorders, which I, of course, also find relevant. However, the survey was to whether or not 1: They have migraines, and 2: if cardiovascular strenuous activies triggered their attacks. There was some confusion of definitions, but roughly, these were the results:
Meniere’s disease with migraine: 138 / 176 = 78,4%
Meniere’s disease who had car sickness as kids: 110 / 143 = 76,9%
Meniere’s disease that’s triggered by higher heart rate: 14 / 16 = 87,5%
These results are interesting, because it shows that the majority of patients with a high prevalence of hydrops, also have a high prevalence of migraines. Now as I said, migraines an be caused both by craniovascular hypo- and hypertension, but hypertension is the most common cause. This, both in regards to statistics, and my own experience.
Consider the following: Long standing hydrops will injury the stria vascularis as well as the dark cells, both responsible for endolymphatic production. Yet, longstanding sufferers still have hydrops upon examination. If production is impaired, why are endolymphatic levels not dropping? This indicates the possibility of severe drainage restrictions, of course, probably along with neural dysregulation.
How the internal jugular vein becomes compressed
In my clinical experience, most patients who struggle with auditory, vestibular or migraine disorders have significant postural and muscular problems. Antonaci & Sjaastad (2011) wrote a review where they correlated tinnitus, vertigo and visual disturbances with cervicogenic headaches. I consider it no coincidence that so many of these patients are experiencing many of the same symptoms, as they often have one or more of the same causes, some of which I have already demonstrated.
Fig. x – Note how the spinous processes of 3-5 are squished together

Briefly, it has been postulated that idiopathic trigeminovascular dysfunction is causing migraines, but I could not possibly disagree more with this. The trigeminovascular system will identify craniovascular hypertension or hypotension (hypotension occurs if there is reduced inflow via the vertebral arteries, for instance, which you can read more about in my migraine article).
As I mentioned, the there are two main causes of true migraines of vascular nature which is related to posture and muscular function.
The first and most common reason, is compromised cerebrovenous drainage, caused by compression of the internal jugular vein. The IJV is very easily compressible, and thus very sensitive to abnormal positions, especially when prolonged. When in a hinge-neck posture (i.e. grossly improper cervical or thoracic posture), the IJV may be squeezed into the transverse process of the C1. Furthermore, rotation or forward translation of the atlas, which is a controversial yet sad reality for many severe neck pain sufferers, may also cause compression of the IJV, as it resides in immediate proximity anterior to the transverse process.
This may go relatively unnoticed while bed lying or similar, at least in less severe cases, but when increasing cardiovascular demand and thus also the requirement for venous drainage, attacks frequently occur. The reason for this is that the degree of jugular compression may not be great enough to create craniovascular hypertension during rest, but it will do so when unable to drain out adequate levels fluid when the heart rate rises. In severe patients, they may have a feeling of pressure within the skull at all times, often indicative of craniovascular hypertension if they are neck-hinging, and most likely also severe enough to continuously restrict venous drainage from the inner ear. This would certainly explain why so many Meniere’s patients both have migraine and hearing disorders.
The image below shows that the atlas has rotated to the right, which is roughly identified in imaging by measuring the distance between the mandibular ramus and the transverse processes. In practice, you’d measure the transverse process vs. the mastoid process of the temporal bone. Either way, we see that the transverse process which is anteriorly positioned, also compresses the IJV (arrow).
Fig. x – From Gweon et al., 2011
The second most common cause of migraine is vertebrobasilar insufficiency due to TOS or similar pathology that may affect the vertebral arteries. I have yet to see a single migraine patient who didn’t have some degree of thoracic outlet syndrome as well as severe neck-hinging posture. Furthermore, summing up all the migraine cases I’ve seen, only one did not hinge at the neck – but she did have TOS.
Research shows that vertebral artery compression may occur in the interscalene triangle, as explained earlier. However, the vertebral artery branches off the subclavian artery proximal to the scalenes. Logically, compression of the subclavian artery at the area of the scalenes, should restrict flow into the arm and increase flow to the vertebral artery, causing basilar artery hypertension. It may be anatomical anomalies that cause some of these patients to get increased flow in the vertebral artery when TOS is present, while others get reduced flow.
If the flow increases and the IJV is compressed, this will case a scenario where increased inflow and restricted outflow is more or less continuously present, if untreated. Reduced flow, however, may cause symptoms of cerebral ischemia as explained earlier. Either way, both of these scenarios may cause migraines, and is in my experience caused by vascular factors, which of course are treatable.
The treatment for compression of the internal jugular vein is mainly to stop hinging at the neck. It makes a dramatic difference. Some patients will be required to treat the atlas as well. If there is TOS, this will also need addressment. Follow the instructions in the next ‘Treatment’ section further down.
Normal venous drainage of the vestibular organs through the vein of the paravestibular canaliculus (PVC) may be crucial to inner ear fluid mechanics. It is proposed that increased venous pressure, with resultant venous insufficiency of the vestibular organs, may result in endolymphatic hydrops unless collateral venous circulation develops. Certain variations in pattern of venous drainage where the vestibular organs drain predominantly through the PVC vein may be a predisposing factor. In patients with Meniere’s disease, different mechanisms can cause venous insufficiency. One suggested mechanism is morphologic change in the microcirculation of the intermediate portion of the endolymphatic sac. Microcirculation changes may be associated with fibrosis of the perisac tissues or shortening of the intermediate sac region or might be physiologically determined. Venous insufficiency may also result from anomalies of the PVC vein – Gussen, 1983
Overall, 30 ears were evaluated. Endolymphatic hydrops (EH) in the cochlea was present in 14 of 25 symptomatic ears (56 %) in patients with tinnitus as the major complaint. Significant hydrops was present in 7 of 14 ears and mild hydrops in the other ears. Patients with fluctuating tinnitus had EH more frequently than patients with stable tinnitus. Furthermore, the presence of ear fullness also correlated with the presence of EH in the cochlea. – Yoshida et al., 2013
Secondary endolymphatic hydrops (SEH) has clinically been found to have a significant incidence of occurrence in patients with subjective idiopathic tinnitus (SIT) of a severe disabling type. – Shulman & Goldstein, 2006
Early descriptions pinpoint the characteristic symptoms as dizziness, visual disturbances, tinnitus, and «posterior» headache, conceivably as a consequence of arthrosis, infliction upon the vertebral artery, or with a «migrainous» background and occurring in «advanced age». Cervicogenic headache (mean age of onset, 33 years) displays a somewhat different picture: unilateral headache, starting posteriorly, but advancing to the frontal area, most frequently the main site of pain; usually accompanied by ipsilateral arm discomfort, reduced range of motion in the neck, and mechanical precipitation of exacerbations (eg, through external pressure upon hypersensitive, occipital tendon insertions). – Antonaci & Sjaastad, 2011
All three patients with bilateral Ménière disease showed endolymphatic hydrops (excess of volume over normal limits) in both ears. Of eight patients with unilateral Ménière disease, five had no symptom in the contralateral ear, whereas three patients had histories of progression from uni-lateral to bilateral Ménière disease 13–21 years after the initial onset. All of the diseased and three of eight contralateral ears showed endolymphatic hydrops. In contrast, no hydrops was observed in any part of the membranous labyrinth in asymptomatic ears. – Morita et al., 2009
The stria vascularis is the main vascular supply to the cochlea and is responsible for endolymph production needed for maintenance of the health and function of the hair cells. – Handbook of Veterinary Neurology (Fifth Edition), 2011
All had the sudden onset of hearing loss and other neurologic phenomena that could be attributed to vasospasm, including vertigo, amaurosis fugax, hemiplegia, facial pain, chest pain, and visual aura. We suggest that vasospasm of the cochlear vasculature was the cause of the sudden hearing loss in these patients. A personal and family history of migraine should be sought in patient; with sudden heating loss and when found, a trial of antispas modic agents should be considered. – Viirre & Baloh, 1996
The diameter of IJV and distance between the styloid process and lateral mass of the atlas at IJV obstruction side in obstruction group were 1.6 ± 1.0 mm and 4.1 ± 2.1 mm respectively, which resulted in statistical significance (p<0.01). The maximum area of lateral mass of the atlas at IJV obstruction side in obstruction group was 103.4 ± 25.3 mm2 which is significantly larger than in control group (p<0.05). – Gweon et al., 2011
It has been demonstrated that internal jugular vein (IJV) compression aggravates headache intensity in patients of migraine. In the result, the venodilatation of IJV in response to each level of Valsalva pressure in patients with migraine was significantly less than that in normal individuals. – Chung et al., 2010
Patients with acute migraine thus appear more sensitive to increased cerebral venous pressure or intracranial pressure. – Chou et al., 2004
We aimed to assess whether migraine is associated with changes in the distribution of the venous drainage through primary and secondary pathways by using phase-contrast magnetic resonance imaging (MRI). Cine-phase contrast scans with high-velocity encoding were employed to quantify arterial inflow and flow in the primary venous channels (right and left jugular veins), whereas scans with low-velocity encoding were employed to quantify flow in the secondary venous channels (epidural, vertebral, and deep cervical veins). CONCLUSION: Migraine patients showed a significantly larger percentage of venous outflow through secondary channels. The mechanism of this alteration remains to be elucidated. Potential mechanisms include repeated release of vasoactive substances or growth factors. – Koerte et al., 2011
Advanced magnetic resonance venographic techniques used in strictly selected subjects disclose transverse sinus asymmetries in as many as 50.6% of patients with chronic migraine, even when mild differences in physiological caliber are excluded. The unexpected correlation between transverse sinus aplasia and some risk factors for migraine chronification requires confirmation in larger studies. – Fofi et al., 2012
Migraine and hypertension are common conditions that frequently coexist. The relationship between the two is usually coincidental, but some evidence suggests that poor control of blood pressure may exacerbate the frequency and severity of migraine. In patients with migraine and established hypertension, good control of blood pressure may be beneficial in controlling their headache. – Prentice & Heywood, 2001
Another consequence of the distension of the saccular membrane in endolymphatic hydrops is the resulting contact the membrane makes with the undersurface of the stapes footplate. This is thought to lead to a positive Hennebert’s sign (induction of dizziness or nystagmus when the stapes is displaced by pneumo-otoscopy) in approximately 30% of patients (Nadol, J. B., Jr., 1977). – Harris & Salt, 2008
Long-standing, stable elevation of CSF pressure with the cochlear aqueduct blocked induced a slowly increasing perilymphatic pressure, always stabilizing at a pressure rise significantly less than that of CSF. The results do not suggest any major pressure transfer via perineural or perivascular routes. The endolymphatic sac is postulated to mediate a reduced and delayed transfer of increased intracranial pressure to the labyrinth. – Carlborg & Farmer, 1983
The pathogenesis of isolated headache in CVT (cerebral venous thrombosis) in the absence of intracranial hypertension, SAH, meningitis or intracerebral lesion is unknown but may involve changes in the walls of the occluded sinus. Hence MRI/MRV should be used to look for signs of CVT in all patients with recent headache (progressive or thunderclap) even when the CT scan and CSF examination are normal. – Cumurciuc et al., 2005
The author describes the case of a 68-year-old woman who experienced severe symptoms of Ménière’s syndrome. Ultrasonography of the neck detected a clot in the left internal jugular vein. The patient was hospitalized and anticoagulated, and her symptoms soon resolved. – Scaramella, 2003
Stria vascularis has a higher oxygen consumption than brain tissue, and the strial capillaries are larger in diameter, with a higher hematocrit and a slower flow than the capillaries of any other tissue types [41]. Schuhknecht defined the strial type of sensorineural hearing loss that is characterized by a flat stria vascularis [42,43] and reduced stria vascularis function; it has been implicated in the pathogenesis of presbyacusis [44,45] – Ciuman, 2013
The sudden left-sided deafness likely resulted from ischemia, possibly due to migraine- associated vasospasm. Presumably, the right ear suffered only minimal damage when the patient was 50 years old, but this damage later led to the development of delayed endolymphatic hydrops on the right. Otolithic crises are thought to result from pressure changes across the utricular macule. We speculate that loss of hair cells in the utricular macule resulted from a collapse of the utricular membrane onto the macule. – Lee et al., 2000
The fact that migraine can be associated with endolymphatic hydrops (EH) is important and demonstrates a potential relationship between the pathophysiology of migraine and that of EH. Given this patient’s previous association of migraine and hearing loss at age 12, it appears that migrainous attacks occur simultaneously with the hearing loss, and may be potentially causative of the fluctuating hearing loss, mediated possibly through the development of EH – Liu et al., 2017
The duration of [Meniere’s] disease significantly correlated with the extent of both cochlear and vestibular hydrops, but not with the number of definite vertigo days. – Jerin et al., 2018
The pathophysiology of vestibular migraine and Meniere disease has yet to be completely defined. As such, there is a great deal of overlap between the two disorders in terms of presentation and diagnostic criteria. While endolymphatic hydrops is still thought to be the cause of Meniere disease, this theory has been challenged and migraine has been implicated as a common etiology between vestibular migraine and Meniere disease. – Liu & Xu, 2016
In 1965, Kimura and Schuknecht published a guinea pig model of chronic endolymphatic hydrops with ablation of the endolymphatic sac [4]. Although extreme, the model proved effective in inducing chronic endolymphatic hydrops, as demonstrated by histologic findings of endolymphatic fluid inflation after sacrifice. The experimental chronic hydrops was associated with impairment of vestibular function (notably nystagmus) and hearing. – Mom et al., 2015
Perilymph fistula (PLF) is defined as a leak of perilymph at the oval or round window. It excludes other conditions with “fistula” tests due to a dehiscent semi circular canal from cholesteatoma and the superior canal dehiscence syndrome. It was first recognized in the early days of stapedectomy as causing disequilibrium and balance problems before sealing of the stapedectomy with natural tissue became routine. It then became apparent that head trauma and barotraumatic trauma from flying or diving could be a cause of PLF. – Hornibrook, 2012
Menière’s Disease (MD) is defined as the idiopathic syndrome of endolymphatic hydrops, characterized by sudden spells of rotatory vertigo and hearing loss, tinnitus and aural pressure, caused by a distension of the endolymphatic space of the inner ear. – Gürkov et al., 2016
Perilymphatic or labyrinthine fistula is a condition in which an abnormal communication is present between the perilymphatic space of the inner ear and the middle ear or mastoid. The manifestations of this disease vary in severity and complexity, commonly ranging from very mild to incapacitating. Perilymphatic fistulas (PLFs) may induce hearing loss, tinnitus, aural fullness, vertigo, [1]disequilibrium, or a combination of these symptoms. The vagueness of symptoms caused by perilymphatic fistula (PLF) and the overlapping symptoms of other disease processes make the diagnosis elusive. – Kutz et al., 2016
The diagnosis of perilymph fistula must always be considered in the appropriate clinical setting of head trauma, barotrauma, and in patients with unresolved and undiagnosed episodes of recurrent vertigo or hearing loss. Surgical treatment with patching of oval and round windows remains the mainstay of therapy for this condition. – Maitland, 2001
LO (labyrinthitis ossificans) was associated with significant cochlear damage (to the spiral ganglion cells, cochlear hair cells, stria vascularis, and spiral ligament) and with increased intensity of endolymphatic hydrops. – Kaya et al., 2016
Hydrops acts as a variable Starling resistor upon the inner ear vasculature that is capable of inducing ischemic attacks only in people with reduced perfusion pressure in the ear. The unique characteristics of the attacks (loss of vestibular response and hearing acutely followed by a return to apparent normalcy over hours) are explained by the differential sensitivity of the inner ear tissues to transient ischemia, with the sensory tissues (dendrites, hair cells) vulnerable to hours-long ischemia/reperfusion injury, and the stria vulnerable to ischemia due to its high metabolic rate. Permanent hearing loss and vestibular damage after many attacks would result when small areas of irreversible sensory cell damage accumulate and become confluent. – Foster & Breeze, 2013
In guinea pigs with experimental endolymphatic hydrops, however, pressure gradients between the endolymph and perilymph remained preserved after rupture of the round window membrane. This is considered as further evidence that after long-standing distention of Reissner’s membrane the membranous labyrinth loses its ability to equalize endolymphatic and perilymphatic pressure. – Böhmer, 1989
Excess pressure accumulation in the endolymph can cause a tetrad of symptoms: (1) fluctuating hearing loss, (2) occasional episodic vertigo (usually a spinning sensation, sometimes violent), (3) tinnitus or ringing in the ears (usually low-tone roaring), and (4) aural fullness (eg, pressure, discomfort, fullness sensation in the ears). – John C. Li, 2017
The levels of the adenine nucleotides ATP, ADP, and AMP in the stria vascularis were measured under normal conditions, and following various durations of ischemia. The concentrations of these compounds were used for the calculation of the adenylate energy charge, the energy status and the phosphorylation state of the stria. Following 10 min of ischemia the adenylate energy charge had decreased three fold, the energy status seven fold and the phosphorylation state 14 fold. Recovery of the endolymphatic potential following brief periods of ischemia was paralleled by a corresponding increase of the ATP levels and a drastic decrease of the AMP levels of the stria vascularis. Preliminary results on the effects of substrate-free perfusion are presented. – Thalmann et al., 1979
The examination of a case of unilateral Menière’s disease confirms the previously expressed opinion that the frequently observed circumscribed herniations of the saccular and utricular wall are not healed ruptures of the entire wall but only ruptures of the inner layer with outward bulging of the outer layer. – Altmann & Zechner, 1968
No rupture was seen in any part of membranous labyrinth in normal temporal bones. The volume data of the cochlear duct, saccule, and utricle in the normal temporal bones fitted the pattern with a normal distribution. The rupture was seen in 13 of 22 temporal bones with Ménière disease. The most common site of rupture was utricle (nine of 22), followed by ampullae of the semicircular canals (six of 22). Rupture of saccular membrane was seen in only two temporal bones. – Morita et al., 2009
Rupture of Reissner’s membrane or the presence of perilymphatic fistulae may also cause SSHL. – Salomone et al., 2008
The pathophysiology of idiopathic sudden sensorineural hearing loss (SSNHL) is poorly understood. Few case reports have proposed a possible link between migraine and SSNHL. This population-based study demonstrates that migraine is associated with an increased risk of idiopathic SSNHL, which, however, is a rare condition. – Chu et al., 2013
Identification and treatment
As I have hopefully been able to reliably demonstrate, the temporomandibular and cervical complexes may greatly contribute to auditory dysfunction. Treating these complexes can be difficult, especially in whiplash patients. For detailed information on these topics, you will probably need to read through the articles that I have linked. The greatly multifactorial nature of tinnitus makes it infeasible to fit all the detailed treatment options in this one article. I will however outline a gross approach.
Identification
In order to know what to treat, you will first need to estimate the likelihood of certain disorders being present. In other words, you need to examine the patient to find the problem.
First of all, based on the patient’s structure it is at least possible to get a basic theory of what might be going on. And, this is presuming that the patient already went to exclude serious pathologies via imaging and the ENT. Ask about the patient’s history / examine them:
Do they have or priorly had neck or jaw pain? Stiffness is also relevant to some degrees. Clicking in the jaw (indicating that the TMJ disc is displacing)? Car accident or similar neck trauma? Are there signs of fullness of the ears or aural clicking (indicating eustachian tube dysfunction)? Is there a history of migraines, either present or priorly? Does the patient have vertigo or headaches? Does their external jugular vein distend as they sit or lie supine (indicative of increased secondary venous drainage, and potential IJV compression)? Do they hinge at the neck or have significant forward head posture or thoracic kyphosis (hinging is implicated by finding an indent / divot between the spinous processes at one level)? Is there underdevelopment of the maxilla (a big nose and/or receded chin is indicative of poor maxillary development (i.e. cheek line)? History of trigeminal neuralgia or similar neurologic disorder? Is there a dropped hyoid bone (lower than C3 – indicative of poor cervical stability and inhibition of the deep neck flexors)? Is the mandible maximally retracted in resting position (there should be a minimum 3 mm clearance between the socket and condyle)? Is there atlas torsion (the C1 transverse process should be located directly and symmetrically beneath the mastoid process of the temporal bone, bilaterally)? Are they clenching the hyoidal musculature in posture or during neck loading?
Fig. 2

Fig. 8

Next, try to find out which movements the patient can do to modulate the pitch of their hearing disorder. For tinnitus, it is usually possible to find a trigger by moving in and out of positions. For hyperacusis, hearing loss and similar disorders, it is not always possible to find a dynamic (movement) correlation in the moment, and thus an elimination approach must be used to find the triggers.
Generally, at least for tinnitus, a periodic stretch of the muscles that are thought to entrap a certain nerve may be performed. If this does not yield any pitch change, try squeezing your thumb into them for 10 seconds. The most painful muscles (upon squeeze) are usually also the weakest ones, so pain is a relatively good indicator of dysfunction. If still no sound, try to strengthen them for one week. If no response in pitch by any of these, presuming the patient performed their exercises (if prescribed) correctly, the respective muscle(s) may possibly be excluded, i.e. eliminated from consideration.
The (Cruveilhier’s) cervical plexus can be grossly tested by pulling the chin down to the sternum for a good 30 seconds. Does the pitch change? For the trigeminal nerve, forward or backward movement of the jaw, as well as manual pressure into the auriculotemporal nerve between the ear and mandible, or into the lateral pterygoids. For the vagus nerve and brachial plexus, perform ipsilateral rotation and dorsal cervical movement to pull the ipsilateral ear toward the spine (as in the DeKleyn’s test as shown below), once again for thirty seconds. For the sympathetic cervical plexus, have the patient pull the head back toward the dorsum (spine) with a nasty cervical hinge, leave it for thirty seconds. In the latter, you are looking for both pitch changes as well as a feeling of intracranial hypertension, as the jugular vein most likely compresses against the atlas.
For vascular testing, these are once again similar to the DeKleyn’s test for the vertebral artery and posterior cevical hinging to see if intracranial hypertension occurs (simply ask the patient if they feel pressure building up fast). Generally, because vascular symptoms tend to show up after higher demand of cardiovascular activity, these tests may seem negative unless the patient has severe dysfunction, and may be done right after a short jog or similar. Evaluating the patient’s posture, musculature and history (migraines etc) are usually greater indicators of possible dysfunction than just doing these tests. Thus, just because a test is negative, this doesn’t necessarily mean that no relevant musculoskeletal dysfunction is present.
Fig. x – DeKleyn’s / Vertebral artery dissection test

Treatment
Once you have identified one or more areas of dysfunction, you will of course need to treat them.
The neck is the foundation, and it needs to be stable in order for the regional musculature to function properly. For example, it is relatively well known that a lot of people develop jaw disorders after neck trauma. The reason for this is that these patients start to clench the hyoidal muscles to make up for poor function of the deep neck flexors. Although this compensation to some extend may help to stabilize the neck, it will often cause the mandible to jam into the TMJ socket, causing an array of problems both in the neck and jaw, such as TMD, and further exacerbation of the cervical musculature.
Moreover, scapular and thoracic positioning will greatly influence the neck as well. A dropped scapula and/or excessive kyphosis of the thoracic spine will promote cervical hinging, which once again causes utter inhibition of the deep neck flexors, scalenes, sternocleidomastoid and more. Spinal integrity (alignment) is necessary for these muscles to work properly and reflexively. Read more about why the shoulder affect the neck in my atlas and TOS articles, or more specifically in my scapular dyskinesis article.
Therefore, learning to maintain ‘long neck’ posture, with proper cervical, thoracic and scapular positioning, and without clenching the hyoidal musculature, is the first and most important step to stop things from getting worse, and setting the foundation for proper rehabilitation. Furthermore, regarding posture, you need to be aware that it is a common MIS-conception that exercises fix posture, but they do not. They are absolutely NOT capable of fixing our poor habits. Only hard, conscious work will fix poor structural habits.
Fig. x

In these videos I will show you how to properly address your posture.
If there is significant maldevelopment of the maxilla (less than 3mm margin between the dental occlusion resting position and the joint socket), these patients may also need to move their jaw forward in posture. They will also need to learn how to open the mouth properly. Once again, read more about this in my TMD article.
Once proper posture has been achieved, rehabilitation of the musculature that has been found related to nerve entrapment or similar, must be rehabilitated, which basically means carefully strengthened. A rough exercise program for injured muscles will result in severe pain and loss of motivation. 5-10 repetitions per day is usually a good starting point. If no symptoms, increase a little, gradually.
For the various nerve entrapment syndromes we have been discussing, strengthening the pterygoids, trapezius, longus colli, longus capitis, scalenes, sternocleidomastoid and suboccipital muscles will be a good start, presuming the adeuqate postural correctives have been implemented already. This will, once the muscles are once again strong and healthy, cause the vagal and trigeminal nerves along with the brachial, cervical and cervical sympathetic plexuses to un-entrap. This approach will also decompress the internal jugular vein and vertebral arteries. Although this may seem simple, maybe even too simple to be true, you will see that implementing all of these correctives after (often) a lifetime of dysfunction is extremely hard work, and requires significant dedication and patience from the patient. Thus, not that simple after all.
Exercises for the muscles mentioned may be found in the various articles I have linked, as well as on my YouTube channel.
It is also rarely a pain free protocol, as the weak muscles cause exacerbate before they get better. Thus the importance of starting gently, as stated.
Now, regarding potential atlas torsion. As I said earlier, anterior translation or torsion of the C1 may compress the internal jugular vein, usually unilaterally, under more serious circumstances. It may also affected the cervical and sympathetic cervical plexuses. The process for correcting this is way outside the scope of this article, and also not very common. Read about this in my atlas article.
Summary
Tinnitus and other hearing disorders are often associated with specific musculoskeletal factors, and these may be treated with good results. The nerves that control the structures of the middle ear, such as the eustachian tube, ossicles and tympanic membrane may become entrapped within the neck or jaw, causing faulty signalling to the ear and thus varying degrees of dysautonomia, which may in turn result in hearing and vestibular disorders. It is therefore important to examine these structures before prematurely concluding that the cause of the disorder must be vestibulocochlear nerve dysfunction or idiopathic hair cell destruction.
Furthermore, endolymphatic regulation in the inner ear may be disturbed both by nervous entrapment in the same regions, as well as impaired venous drainage. Sometimes also by compromised arterial supply, although a little less common. The most common endolymphatic pathology is excessive endolymphatic fluid, which may cause ischemia of the stria vascularis as well as destruction of the stereocilia (hair cells) of the main hearing organ (the organ of Corti). Buildup of endolymph has been demonstrated even when the stria vascularis is damaged (which produces endolymph), indicating that impaired drainage is the most likely culprit. In line with this, patients who have been shown to develop endolympathic hydrops, also also have a very high prevalence of migraines, which has been correlated with venous restrictions as well. It is thus likely that endolymphatic hydrops (or ‘mere’ excess) is caused by a combination of poor neural regulation (possibly due to entrapment), as well as venous outflow restrictions.
In most circumstances, multiple factors contribute to the hearing disorders, and many of these can be treatable. This can in most cases lead to improvement of the disorder, and sometimes also lead to complete reversal.
Technically, the main structures to be aware of, are the trigeminal and vagus nerves, as well as the cervical sympathetic plexus and Cruveilhier’s plexus, which may become entrapped in the neck and jaw, causing diffuse symptoms, often of aural nature. The internal jugular vein may become compressed by neck hinging or atlas torsion, causing restricted outflow, as the tympanic complex’ veins drain into the sigmoid sinus, which in turn drain into the jugular vein.
Hei, veldig spennende lesing! Lurte på om denne artikkelen finnes i en Pdf versjon? Slik at det er enklere å få printet den ut og lest?
Nei, dessverre.
Hei, veldig spennende lesing! Lurte på om denne artikkelen finnes i en Pdf versjon? Slik at det er enklere å få printet den ut og lest?
Superbly written article/ synopsis.
I am a physician/ Internist from India.
My son is having bilateral tinnitus close to 6 weeks.no vertigo and deafness for range up to 8000 KHz. Except for deflected nasal septum,sensory loss beyond 12000 kHz on both sides: ;
Has a bad neck pain and an episode of numbness in left arm and a part of forearm.was listening to music th ear phones for a few years.
Since no relief by ENT surgeons approached a physiotherapist trained in Australia who has promised some relief looking at his neck and posture.
Is there by any means you can evaluate him?
Superbly written article/ synopsis.
I am a physician/ Internist from India.
My son is having bilateral tinnitus close to 6 weeks.no vertigo and deafness for range up to 8000 KHz. Except for deflected nasal septum,sensory loss beyond 12000 kHz on both sides: ;
Has a bad neck pain and an episode of numbness in left arm and a part of forearm.was listening to music th ear phones for a few years.
Since no relief by ENT surgeons approached a physiotherapist trained in Australia who has promised some relief looking at his neck and posture.
Is there by any means you can evaluate him?
Hello
Sounds like cochlear hydrops. It is an ICP problem. Book a skype session and send me magnetic resonance images of his head.
I was 18 when this started. I’m 41 now. I haven’t had a moment of relief. It’s excruciating.
It began as odd but fleeting sensations in my ears. A flutter here, a crackle and tugging sensation there. Soon it became the oddest sensation of “openness” or hollowness in my ears, as if a seal separating the inner ear from the external environment were somehow vanishing.
Anyone who’s had their ears clog up in an airplane knows the sensation of too much pressure in the ears. The feeling I was experiencing was the opposite of that; a vacuous and balloon-ish feeling. Although the opposite of the feeling of excess pressure, this feeling was no less uncomfortable or distressing.
A good example I give people is that of the “vasalva maneuver” which is when you pinch your nostrils and try to blow air out of your nose to pop your ears when you’re experiencing an excess of pressure. That moment when your ears pop and, for a moment (until you stop blowing) there is total openness between your inner ear and the outer environment; that’s how I now feel 24/7/365.
I was freaking out. Day by day it would get worse, never improving, always deteriorating.
Around this time sounds began to grow louder. Normal sounds such as keys being tossed on the counter, or plates colliding in the sink became unbearable. It’s as if someone had turned the volume up on the world! How is this even possible – I thought. What is happening to me?
Then came the sensitivity to changes in air pressure. Things like driving up or down hills, slamming a door, going up or down in elevators; these things caused extremely unpleasant and somewhat painful sensation of tugging at my inner ear (as well as other intense sensations that I find very difficult to describe). Again, as if some kind of seal were not present to shield against this.
There were other symptoms too such as tinnitus, vertigo episodes and momentary losses of balance.
When I read above about the role that the endolymphatic fluids have on inner ear homeostasis, it really caught my attention. I find that the severity of my symptoms is often tied to the presence of a transparent, jelly-like substance that comes from the back of my throat. I will feel it there and notice that when I clear it by swallowing, my symptoms instantly worsen. In fact, once I notice that I have some of this fluid ‘in danger’ of being brought down and swallowed I will often lie down and rest because that seems to prevent this from happening.
I have no idea if this is related to endolymphatic fluids but I thought I would mention it.
Little by little, I was forced to change my behavior to avoid aggravating my symptoms. If I needed to go 10 flights in an elevator, I would break it up into 2 trips, stopping on the 5th floor for a break. I stopped driving anywhere at elevation, etc.
Before this began, I was an aspiring musician with a very promising career. Playing music was the thing that made me happiest and the only path I could imagine for my life. Soon enough that would be taken from me as the sensitivity to sounds and the effect it had of aggravating my symptoms became too unbearable.
I decided to go on this new thing called the internet to try and find out what was happening to me. I came across all kinds of conditions such as Meniere’s Disease, dehiscence of the semicircular ear canal, the effect of tumors in the brain or ears, and on and on. One by one I began to go to doctors and be tested for each of these. And each time the tests came back negative. “You’re fine. Everything works ok. Have you tried just taking anxiety medication?” Urrgg!
Two possible diagnosis seemed particularly promising: Patulous Eustachian Tube Dysfunction (PET) and Temperomandibular Joint Dissorder (TMJ).
PET was the one I was most excited about. People with PET reported many of the same symptoms I had. Aha! – I thought. This must be it!!
It wasn’t easy to find but I found an ENT in Puerto Rico, where I lived, who tested for PET. The results? Negative.
How could this be? I was positive this was it! I’d been searching for three years and was back to square one.
But I brushed myself off and went “all in” on TMJ.
My TMJ dentist gave me an orthotic device to wear all day around my teeth to create the right alignment. I wore it as prescribed and waited. Nothing. No improvement whatsoever. If anything it made things feel worse.
Another dead end.
The months turned into years. I visited countless doctors to rule out every single thing I could find online that could be causing my issue. It all began to feel pointless after a while.
My personal life became severely impacted. I lost jobs due to there being days when I could simply not get out of bed. In fact, I had to learn a skill that would allow me to work from home.
At first it would be just one day that I would be unable to leave my house due to the immense pain and discomfort. Then it became two, then three, then four. Nowadays I stay in my apartment more days than I leave it.
About 20 years into this I moved to Florida and decided to get tested again for PET. Who knows, maybe there had been some advancements during that time.
I get to the doctor and he places some device in my ear. I recognized this as being the same test I had had back in Puerto Rico. “This is it.” I thought, “It’s now or never.” After some poking and prodding the doctor says. “Nope, this is normal. No issues there.”
I was crushed. Back to square one again…
“Now I’m going to do the PET test.” Said the doc.
“What?? That WASN’T the PET test?”
“No, that was just to see if you had a perforated ear drum. The PET test is totally different.”
For 20 years I thought I had ruled PET out and now it turns out that I had never even been tested for it!
He takes me to a different room and proceeds to shove a camera up my nose all the way to be back of my ears. This fun little pastime is called a nasal endoscopy and with it the doctor can actually see the eustachian tube.
“Oh wow.” Said the doc. “Nassim, come look at this!”. An eager intern named Nassim came and peered.
“Yep. You definitely have PET. It’s as clear as day. I can see it right here.”
Nassim seemed to agree.
“Really??”. I said, my vision blurring from the tears of joy.
“Yes. Without a doubt.” Said the doc.
This was the happiest day of my life. I was beside myself with pure joy.
But I wanted a second opinion. So many years of disappointment had turned me into somewhat of a hardened cynic.
I get to the second doctor’s clinic. Same test. Same result. “Yep. You got PET.”
I won’t even attempt to describe how happy I was. This was the new, best day of my life!
“We can do surgery and you’ll be fixed. It’s simple and takes just 30 minutes.”
Yes, yes, yes! Of course I want this. Total no-brainer.
I decided to seek out the world’s top expert in PET to do my surgery. A man by the name of Dr. Dennis Poe in Massachusetts. If I was going to do this, I wanted the expert to do it. The guy who’s done it a million times.
“Dr. Poe’s current waiting list is 12 months. Is that OK?” Said his secretary.
“Absolutely. Put me down.”
A year later I traveled from Florida to Boston (by train because, I’m not able to fly… Did I mention that. Anyway…)
There I was on the examining table of the world’s authority on my condition. He did the nasal endoscopy.
“You don’t have PET.” He said.
“What??”
He proceeded to tell me how I definitely did NOT have PET and that doctors often misdiagnose it because they don’t know the nuances of it.
“It’s probably the TMJ that’s causing this” he said. He then explained that when the mandible sits too far back into its condyle, which is right next to the ear, all sorts of weird sensations can be triggered.
After explaining that the TMJ treatment I had tried didn’t help, he told me to try a “neuromuscular dentist”. That one of them would be able to help.
I was able to find a neuromuscular dentist and after a month and $5,000 spent on an orthodic, there have been no improvements. I know that it will take time for this to work but I’m concerned because my dentist tells me I should be experiencing some improvement already.
I’m writing this post in the hopes that you might be able to point me in a helpful direction. I would love so very much for your thoughts on my symptoms. I feel very much at the end of my rope. I don’t know what else to try if the TMJ orthodic does not work.
Darkness is setting in.
Thank you so much for reading.
There’s other things that make my symptoms worse which I didn’t mention above. I’ll include those below in case anyone’s interested.
– Lying face up
– Straining as when going to the bathroom, exercising or lifting heavy objects.
– Strong scents (I don’t get this one at all!)
– Yawning
– Cold temperatures
– Driving
– Even talking, due to the pressure that’s created in the head.
I have had pulsing tinnitus for over 20 ,years. Mri scans, all sorts of tests . Had a perforated ear drum 45 ,years ago and numerous operations to repair. My pulsing tinnitus is now unbearable and I am extremely dizzy. Dr just prescribes anxiety meds.
I was 18 when this started. I’m 41 now. I haven’t had a moment of relief. It’s excruciating.
It began as odd but fleeting sensations in my ears. A flutter here, a crackle and tugging sensation there. Soon it became the oddest sensation of “openness” or hollowness in my ears, as if a seal separating the inner ear from the external environment were somehow vanishing.
Anyone who’s had their ears clog up in an airplane knows the sensation of too much pressure in the ears. The feeling I was experiencing was the opposite of that; a vacuous and balloon-ish feeling. Although the opposite of the feeling of excess pressure, this feeling was no less uncomfortable or distressing.
A good example I give people is that of the “vasalva maneuver” which is when you pinch your nostrils and try to blow air out of your nose to pop your ears when you’re experiencing an excess of pressure. That moment when your ears pop and, for a moment (until you stop blowing) there is total openness between your inner ear and the outer environment; that’s how I now feel 24/7/365.
I was freaking out. Day by day it would get worse, never improving, always deteriorating.
Around this time sounds began to grow louder. Normal sounds such as keys being tossed on the counter, or plates colliding in the sink became unbearable. It’s as if someone had turned the volume up on the world! How is this even possible – I thought. What is happening to me?
Then came the sensitivity to changes in air pressure. Things like driving up or down hills, slamming a door, going up or down in elevators; these things caused extremely unpleasant and somewhat painful sensation of tugging at my inner ear (as well as other intense sensations that I find very difficult to describe). Again, as if some kind of seal were not present to shield against this.
There were other symptoms too such as tinnitus, vertigo episodes and momentary losses of balance.
When I read above about the role that the endolymphatic fluids have on inner ear homeostasis, it really caught my attention. I find that the severity of my symptoms is often tied to the presence of a transparent, jelly-like substance that comes from the back of my throat. I will feel it there and notice that when I clear it by swallowing, my symptoms instantly worsen. In fact, once I notice that I have some of this fluid ‘in danger’ of being brought down and swallowed I will often lie down and rest because that seems to prevent this from happening.
I have no idea if this is related to endolymphatic fluids but I thought I would mention it.
Little by little, I was forced to change my behavior to avoid aggravating my symptoms. If I needed to go 10 flights in an elevator, I would break it up into 2 trips, stopping on the 5th floor for a break. I stopped driving anywhere at elevation, etc.
Before this began, I was an aspiring musician with a very promising career. Playing music was the thing that made me happiest and the only path I could imagine for my life. Soon enough that would be taken from me as the sensitivity to sounds and the effect it had of aggravating my symptoms became too unbearable.
I decided to go on this new thing called the internet to try and find out what was happening to me. I came across all kinds of conditions such as Meniere’s Disease, dehiscence of the semicircular ear canal, the effect of tumors in the brain or ears, and on and on. One by one I began to go to doctors and be tested for each of these. And each time the tests came back negative. “You’re fine. Everything works ok. Have you tried just taking anxiety medication?” Urrgg!
Two possible diagnosis seemed particularly promising: Patulous Eustachian Tube Dysfunction (PET) and Temperomandibular Joint Dissorder (TMJ).
PET was the one I was most excited about. People with PET reported many of the same symptoms I had. Aha! – I thought. This must be it!!
It wasn’t easy to find but I found an ENT in Puerto Rico, where I lived, who tested for PET. The results? Negative.
How could this be? I was positive this was it! I’d been searching for three years and was back to square one.
But I brushed myself off and went “all in” on TMJ.
My TMJ dentist gave me an orthotic device to wear all day around my teeth to create the right alignment. I wore it as prescribed and waited. Nothing. No improvement whatsoever. If anything it made things feel worse.
Another dead end.
The months turned into years. I visited countless doctors to rule out every single thing I could find online that could be causing my issue. It all began to feel pointless after a while.
My personal life became severely impacted. I lost jobs due to there being days when I could simply not get out of bed. In fact, I had to learn a skill that would allow me to work from home.
At first it would be just one day that I would be unable to leave my house due to the immense pain and discomfort. Then it became two, then three, then four. Nowadays I stay in my apartment more days than I leave it.
About 20 years into this I moved to Florida and decided to get tested again for PET. Who knows, maybe there had been some advancements during that time.
I get to the doctor and he places some device in my ear. I recognized this as being the same test I had had back in Puerto Rico. “This is it.” I thought, “It’s now or never.” After some poking and prodding the doctor says. “Nope, this is normal. No issues there.”
I was crushed. Back to square one again…
“Now I’m going to do the PET test.” Said the doc.
“What?? That WASN’T the PET test?”
“No, that was just to see if you had a perforated ear drum. The PET test is totally different.”
For 20 years I thought I had ruled PET out and now it turns out that I had never even been tested for it!
He takes me to a different room and proceeds to shove a camera up my nose all the way to be back of my ears. This fun little pastime is called a nasal endoscopy and with it the doctor can actually see the eustachian tube.
“Oh wow.” Said the doc. “Nassim, come look at this!”. An eager intern named Nassim came and peered.
“Yep. You definitely have PET. It’s as clear as day. I can see it right here.”
Nassim seemed to agree.
“Really??”. I said, my vision blurring from the tears of joy.
“Yes. Without a doubt.” Said the doc.
This was the happiest day of my life. I was beside myself with pure joy.
But I wanted a second opinion. So many years of disappointment had turned me into somewhat of a hardened cynic.
I get to the second doctor’s clinic. Same test. Same result. “Yep. You got PET.”
I won’t even attempt to describe how happy I was. This was the new, best day of my life!
“We can do surgery and you’ll be fixed. It’s simple and takes just 30 minutes.”
Yes, yes, yes! Of course I want this. Total no-brainer.
I decided to seek out the world’s top expert in PET to do my surgery. A man by the name of Dr. Dennis Poe in Massachusetts. If I was going to do this, I wanted the expert to do it. The guy who’s done it a million times.
“Dr. Poe’s current waiting list is 12 months. Is that OK?” Said his secretary.
“Absolutely. Put me down.”
A year later I traveled from Florida to Boston (by train because, I’m not able to fly… Did I mention that. Anyway…)
There I was on the examining table of the world’s authority on my condition. He did the nasal endoscopy.
“You don’t have PET.” He said.
“What??”
He proceeded to tell me how I definitely did NOT have PET and that doctors often misdiagnose it because they don’t know the nuances of it.
“It’s probably the TMJ that’s causing this” he said. He then explained that when the mandible sits too far back into its condyle, which is right next to the ear, all sorts of weird sensations can be triggered.
After explaining that the TMJ treatment I had tried didn’t help, he told me to try a “neuromuscular dentist”. That one of them would be able to help.
I was able to find a neuromuscular dentist and after a month and $5,000 spent on an orthodic, there have been no improvements. I know that it will take time for this to work but I’m concerned because my dentist tells me I should be experiencing some improvement already.
I’m writing this post in the hopes that you might be able to point me in a helpful direction. I would love so very much for your thoughts on my symptoms. I feel very much at the end of my rope. I don’t know what else to try if the TMJ orthodic does not work.
Darkness is setting in.
Thank you so much for reading.
There’s other things that make my symptoms worse which I didn’t mention above. I’ll include those below in case anyone’s interested.
– Lying face up
– Straining as when going to the bathroom, exercising or lifting heavy objects.
– Strong scents (I don’t get this one at all!)
– Yawning
– Cold temperatures
– Driving
– Even talking, due to the pressure that’s created in the head.
Wow, I just wanted to reply since no one had and take my hat off to you for persistence. I too have similar symptoms and haven’t got half as far as you. I believe mine is to do with either allergies or muscles (neck or TMJ). Both confuse and bewilder the best of our medical practitioners. I think muscles especially are so underrated and many specialists deny they can cause such issues.
Anyway, hope you found some relief.
Hi Fernando
Have you had a high resolution CT scan (0.6mm slices) for Superior semicircular canal dehiscence? A normal head CT scan won’t detect it.
Hello Fernando I too have had a lifetime of very similar symptoms to you I sympathise
I was diagnosed with menieres at age 18
I won’t go into all the false diagnosis, frustration, etc etc living only an existence sometimes rather than a life, I am now 55, but I am now determined to find a decent doctor who has commitment to pursue a illness to a cure, or at.least a valid diagnosis.
So did you go for the high resolution ct ? Please tell me you are getting somewhere .
Hooe you are feeling more positive
Paul
Thanks for the very comprehensive article. I’ll be re-reading this a few times.
In my case I’ve had tinnitus and aural fullness for several months now after a head-hit in the gym. Both tinnitus and aural fullness are mainly uni-lateral on the left but get bi-laterally sometimes. I’m getting a lot of physio around the left TMJ at the moment which seems to have a lot of modulation on both tinnitus and aural fullness and can often get both to settle for short periods.
Have you had much experience before with head trauma being linked to tinnitus and aural fullness?
Thanks for the very comprehensive article. I’ll be re-reading this a few times.
In my case I’ve had tinnitus and aural fullness for several months now after a head-hit in the gym. Both tinnitus and aural fullness are mainly uni-lateral on the left but get bi-laterally sometimes. I’m getting a lot of physio around the left TMJ at the moment which seems to have a lot of modulation on both tinnitus and aural fullness and can often get both to settle for short periods.
Have you had much experience before with head trauma being linked to tinnitus and aural fullness?
yes I do have bilateral tinnitus since I was 18(now 62) high-pitched whistle 24/7 ,shame on medical field they haven’t
found no tx for this anomaly
What about pulsatile tinnitus caused by impaired venous drainage of the transverse, sigmoid & internal jugular sinus? How is that caused? Is it also related to neck diseases?
Pulsatile tinnitus has also been associated with craniovenous drainage dysfunction
Hello,
I have read your article on the association between tinnitus, neck, and TMJ and all of the neural sensations that can and do occur. It’s such a frustrating and exhausting condition because doctors, dentists, and neurologists don’t seem to work as a team to treat patients effectively – it’s haphazard at best and most shake their heads in disbelief. I have an MRI showing bilateral TMJ degeneration with disc displacement without recaputure, have a cervical MRI showing degeneration at C5-C6 and experience 24/7 tinnitus, vibrations and tingling in feet, but no jaw pain, only tightness. Chronic neck and shoulder pain. Likely a whiplash condition as well from multiple car accidents over the years. I am currently in PT for postural improvement, also seeing a cervical chiropractor, and wear a oral acrylic appliance at night to keep teeth apart but it is not a “stabilization split” (not sure if I need that or who to go to ). I am seeing “some” symptom relief but am not sure if there is more I can do and what will happen as my TMJs further degenerate (I’m 57 yrs old). I am looking for cervical and TMJ expertise in the USA if you have any colleagues who are well versed in this area to deal with the neurological symptoms that are resulting and long-term management for the TMJs. I would willingly participate in a scientific study to help better understand this condition which seems to be a combination of SCM syndrome and TMJ dysfunction.
What should one with TMJ do for sleeping position?
Lie on your side and use a splint (that advances the mandibule) if you’re worse in the morning than in the evening.
Hello,
I has a tinntius in the left ear 1 year and half ago.
I found 2 disc hernias c5-c6 and c6-c7 with artrithis it is pressing some nerves in the back. Do you think this cause my tinnitus? Thanks in advancd
No, this does not cause tinnitus.
Just read this and had to reply. It’s been over two years since my tinnitus(high frequency whistle in left ear) began to be a problem. Finally after two disc replacements, c6-c7 one year and c5-c6 the next year, the volume of the tinnitus has dropped by two thirds and on some days it is almost completely gone. But it does come back it seems when I sleep and my neck gets itto funny positions. I’m getting ready to start some more imaging to figure out what is causing this last bit of tinnitus. I suspect it is c7-t1 and I will be requesting that my neurologist order me a weight bearing mri because normal supine mri I believe leads to misdiagnoses which is why I had to have two separate disc replacements. I knew after several doctor visits to different doctors that kept telling me that my tinnitus was caused by high frequency hearing loss that they were wrong. Mainly due to my daily experience with the tinnitus being better in the morning when I first got out of bed versus late in the evening when it would be at its loudest. So I can without a doubt say cervical tinnitus is real. In addition to the tinnitus the disc herniation’s were causing numbness and sensitivity in my toes along with many other symptoms such as hearing sensitivity, light headiness, balance problems, low blood pressure, heart rate regulation, thermal regulation, atrial fibrillation, heart palpitations, shoulder and elbow pain, shoulder and bicep weakness and other symptoms. All my symptoms have been atypical, the orthopedic surgeon said that out of all his years I’m his first patient with such symptoms.
Radiculopathy does not cause tinnitus.
I have a c5 c6 radikulopaty and severe tinitus. Do you think in can be Just coincident, and the reason of tonnisus is different eg stress or TMJ.
Radiculopathy not related
Hi, any Ideas, I have blocked ears on and off, crackling and popping in ears when eat and swallow, pain in ears and pain in jaw joint sometimes. I all so have had tinnitus start i the left ear, Every ENT person I see tells me something different is wrong. thanks
Usually an upper cervical problem.
Wow- I have been trying to do Research on tinnitus since I myself suffers of it. I have been working now with My own self care treatment practice in Belgium and your insight on muscle and nerve function in relation to tinnitus was an eye opening for me since I believed and have the same theory. Thank you. Forever grateful
Your article is incredibly detailed and fascinating, and maybe even hopeful.
I have had very distressing bilateral steady and pulsatile tinnitus of varying intensity and shifting symptoms for 3 years now, with an incredible list of somatic movements that change or even nearly eliminate the sound. An MRV showed stenosis in the distal left transverse sinus but the somatic movements that change the sound seem likely to rule out that being the cause of the tinnitus according to a neurosurgeon here at MA General in Boston.
I do have potential TMJ issues, and even clenching of my jaw nearly eliminates the tinnitus, and the tinnitus is always worse in the morning.
I have been seeing a Physical Therapist and Chiropractor, and sometimes the treatments seem to help (temporarily) but also can stir up the tinnitus and seem to make it worse.
Do you know of anyone here in the Northeast US who has your kind of knowledge regarding this problem? Most ENT’s seem clueless.
Also, any thoughts on the possibility of neck/head/jaw issues causing PULSATILE tinnitus would be very helpful.
I thank you very much for any thoughts you can provide.
Hi—wondering if you have input. I have fluttering in my right ear that is triggered by yawning. Sometimes it starts in the evening and continues all throughout the night and then miraculously stops when I get up for the day. It feels like a twitch and is extremely distracting. I’ve suspected it has something to do with my neck or jaw. I am currently waiting to see someone about it but for now am reading through info I can find online.
Could be either eustachian tube dysfunction or a TMD sequela
I have this same thing! It sounds like someone tapping morse code in my ear. Really anxiety inducing. I have tinnitus and eustachean tube dysfunction in my left ear as well, and my jaw definitely opens the wrong way (as demonstrated in the video). Thanks so much for this article!
Could an inflammation or irritation of the inferior alveolar nerve cause endolymphatic hydrops and tinnitus?
Tinnitus yes, hydrops no. If there’s hydrops, look into intracranial hypertension. See my article on the topic.
Hi there, can hydrops go away ?
Depends on the cause. “Can”, yes. It can.
Hi Kjetil! I got tinnitus out of nowhere in before christmas. Ive not been exposed to any extreme loud sounds. Its a high pitched ringing in both ears, it started with one ear. Its always worse in the moment Im yawning or doing the Valsalva maneuver (goes from high pitched to LOAD high pitched) in the moment I pinch my nose while expelling air out. Do you have any ideas? I also have an history with pain (an inflammation) in my jaw (duration of 6 months) before I got the tinnitus. But I was painfree from the jawpain in several weeks before I got the ringing ears. Hope you have some uplifting words!
Thank you for this article! I have very bad tinnitus in my right ear. I have seen an ENT and his response was basically “deal with it.” I have had head and neck trauma so I recently asked my family doctor to refer me to a spinal specialist. Today, he has but it will be some time before I see the specialist.
Today after reading this article I pushed my lower jaw forward and noticed the tinnitus gets louder. Also, I noticed today if I press on my right side of my head just above the jaw connection forward of my right ear the tinnitus gets louder. To me, it sounds like I may have TMJ / TMD related tinnitus. I have been recently told by my dentist that I may be grinding my teeth while I sleep.
I will try the TMD stretching and strengthening until I see the spinal doctor.
Again, thank you VERY much for this article. I have searched the Internet extensively and just found this article. You may change my life! My tinnitus is so bad that I hardly sleep and I am always physically and mentally tired.
Hi. Been suffering TMD for 1 months now. Both of my ears are clogged, vertigo, tinnitus, pain in the neck, jaw and back. Eyes are blurred and eye floaters. Please help me. Its getting worse and worse.
Articolo fantastico! Molte grazie
I’m 21 and have had tinnitus in right ear for a few weeks. Hearing test is normal. I don’t have pain but can change the sound by clenching my jaw and my neck muscles seem stiffer on the right side (can’t do lateral flexion as far as with left side). Had a cold the week before it started but that’s cleared up. Is there a chance this will go away, should I see a physio/osteopath? Thanks
Hi, I found this article incredibly helpful! I started suffering from Pulsatile tinnitus in both ears out of the blue about 8 months ago, followed by high pitched hissing tinnitus. I then developed Eustachian tube dysfunction a couple of months later – and hear popping in my ear every time I yawn, swallow and sometimes at random. ENT couldn’t find any issues with imaging. I realised my jaw was extremely clicky and I got a mouth guard from the dentist which helped. I also have had neck pain and limited mobility of the neck, and I can modulate the sound of the high pitched tinnitus when I move my jaw outwards. Do you think this is all being caused by the neck/jaw?
Thank you for the comprehensive article. So many roads lead to tinnitus. Wish you all the very best on your journeys.
I was diagnosed with TMD in 2011. Forward positioning splint, physical therapy helped alleviate most of the classic symptoms for ~4 years. But, I stupidly thought I was stabilized and stopped seeing my dentist. Splint wore out during that period, but continued to wear.
Scoliosis, forward neck tilt from sitting at a computer desk, you name it.
In October 2021 after 3 weeks of silent reflux that radiated to my nose/right side of my jaw, experienced ear ringing/fullness/pressure/underwater like muffling in left ear. Resolved by the time I woke in the morning. ~2 weeks later, ringing started in right during work call and hasn’t stopped. Tone changes throughout the day. Also experience crackling/popping/pressure/fullness feelings in both ears, but only right experiences consistent tinnitus. Suspect hyperacusis in right ear. Right side neck pain, cervical pain. Turning my head to the right loudens the tinnitus pitch.
ENT suspects ETD, noticed nose congestion, cobble stoning in throat from reflux. Currently on 20mg esomperazole, flonase for 2 months.
Recent MRI rated my TM joint as PIPER 5B, but according to dentist no change in the 3 MRIs conducted over the last 10 years. Dentist outfitted me with new forward advancing splint 3 weeks ago. Botox injections in masseter, trapezius planned for this Friday to address tender jaw muscles. Appt booked with spinal doctor to address cervical pain, constant knots Jan 6. Kjetil – are you available for a skype session, could use your assistance. I am bewildered and don’t know how to go about this fact finding mission.
My vertigo then tinnitus developed after the Phizer vaccine. There is still constant noise and a loss if 25% hearing in one ear.
Likely vestibulocochlear neuritis. CTA to exclude thrombosis can also be helpful
My mom is 85years old and since 2018 she has had a loud crackling (like someone stepping on glass)in her right ear that comes and goes in LOUD clusters and this has been very intense and overwhelming. She has to hold onto walks to walk in her house! Is this even consider tinnitus because it’s not ringing or buzzing or whooshing etc?
2019 we found a surgeon that said middle ear resectioning of the tensor tympani and the stapedius and has helped with some patients so we went with that. IT WAS A MIRACLE!! It helped!! That was in August 2019..but it only lasted a few months and dealt with it on and off but it was “in a distance” sounding she said, And for the past 2 months its sooo loud it has incapacitated her, making her hv to use a walker in home . She lives alone and its breaking my heart that there seems to be no real answers . CT and MRI of brain and IACS are negative. Trying trileptal anti-seizure as dr said it may help. MY mom is normally constantly on the go and now she holds on to walls and gets dizzy with the crackling. She can’t sleep or live like this..any thoughts? thank u-God Bless, Kare
I need much more information. You’ll have to book a consult
Hi. 9 days ago I had a MRI for my tmj with my mouth open. My doctor found that I have TMD. But since the MRI I have a constant burning pain in my right ear and it’s worse with sound, like a noise sensibility. The audiologist said the noise from the MRI is safe for my hearing and I had earplugs during the test. Can TDM or the fact that I kept my jaw open for too long can cause my symptoms?
Probably just worsened by the mouth opening. No big deal if you follow the steps in this article.
Thanks for your quick response. Can tmd cause or mimic hyperacusis. Because I’m scared to have hyperacusis, since noise increase pain in my ear. The doctor said i have really bad tmd
Hi do you respond To me? Because your response date from 2019
Can bad tmd cause hyperacusis. And if i follow the steps in the article it will go away. Thank you.
Yes; impingement of the auriculotemporal nerve. Read my TMD article
Hello,
The past 2 months I have had some weird symptoms and some anxiety of course. Basically, I have aural fullness/pressure in both my ears — intensity changes. I have tinnitus in both ears, the left is loud and pretty much blocks out the right. I also have jaw tenderness where I get pain in my left ear and tenderness under my lobe. I also have neck pain and sensitivity to sound – both ears. Running water, crackling water bottles — pretty much high frequency sounds. I have seen an ENT, said ETD without much testing. I also feel dizzy, even sitting at my computer right now. I do have cervical spine spondylosis with disc degeneration of C5,6,7. Had a hearing test done at ENT, came back normal. I have crackling sounds in my ears when I swallow, sometimes I get a popping sound without doing anything. It feels like my ear canal is swollen or something – ENT says ears look fine. I went to the dentist who said I have some wearing on my enamel (not much) and had a mold done for a night guard. I don’t get that back for another week. I feel best at night and worse in the morning — intermittent neck pain and have pressure in the head. I do have mega tension in neck, shoulders, etc. and I do notice I tend to tense my jaw — working on that and trying to adjust when I notice and keep my tongue in between my teeth trying to relax my jaw. It is really affecting my quality of life, particularly the sound sensitivity or hyperacusis.
Currently pending a neck MRI and looking into scheduling an appt with a TMD specialist. Anyway, could TMD cause all these symptoms? Or could it be a combo of TMD and cervical problems?
hi karla any updates? when you say sensitivity to sound do you mean you feel your ear reacting to sound? one of my ears thumps in reaction to sound including to my own voice. it also has pressure on and off. and CONSTANT diziness like im being pushed. i think what i have is tonic tensor tympani but not sure what to do, dizziness is debilitating. i know there is surgery where they cut the muscle but not sure if it will make my dizziness worse.
Anna
Hello,
I have read that splints can make the problem worse. When thinking in terms of having a splint that is helpful, should it be designed to maintain protraction for short periods of time, maybe a few times a day, to give the joints a rest, and to create a scenario where the muscles get used to new positioning? If so, who would be the best person to make such a splint? If not, what type of splint would be the best? There are so many people claiming to be TMJD “Specialists,” and it would be easy to spend a lot of money on things that can potentially worsen the situation.
Thank you greatly.
I usually recommend a mandibular advancement splint that protracts the mandible by at least 3-4mm while in use.
Hello, What diagnostic tests should be ordered for TMD issues (MRI, CT, Ultrasound)? Is there an order of which they should be ordered? Can you avoid CT scan (radiation) and just do an MRI and Ultrasound? What tests would you personally need to do an adequate consultation? I have a known and obvious TMD issue. I have had so many CT scans in my life (2 as a child), and I would like to avoid radiation if the MRI would suffice. I also have C-Spine spondylosis which would be part of my consultation. I do believe for that it would be an MRI, correct? Please advice. Thank you greatly.
TMD is easily diagnosed clinically and an MRI is generally not needed. If significant damage to the joint is suspected, you can do a jaw MRI. The main purpose of this is to exclude complete perforation and tearing of the retrodiscal ligament or the disc’s attachment to the upper head of the lateral pterygoid.
Hello and thank you for responding: I appreciate it.
In preparation to consult with you regarding my C-Spine, would an MRI without contrast be sufficient?
I had nerve function tests at a neurology office, and I will also have those findings.
Thank you greatly.
Hi Larsen,
Thank you for writing such a great description of association of TMJ with hearing. I have hearing problem since last 4 years. The pattern is strange as it affects one ear at a time. I never had problem in both ears at a time. I observe the following symptoms in my affected ear:
1. First and most important symptom is fullness of the ear
2. Muffled hearing (I can understand the loudness of somebody’s speech but can not identify many words).
3. Crapitation/fluttering/fluid movement sounds when I bow my head down and take it up.
4. Crapitation/fluttering sounds when I push my ear up from the back side (the cartilage of ear).
5. Always hear popping or crepitation sounds in ear when I yawn or open my jaw mediumly or maximum wide, and sometimes during eating.
6 My multiple pure tone audiogram tests suggest that I have hearing loss at high frequencies in both ears through air and bone conductance. At lower frequencies, my hearing is normal.
7. My affected ear listens to the normal sound of a person as very sharp.
8. I never had pain or discharge from my ears in my life. Neither do I have pain in jaws or TMJ joint. Very rarely, I feel pain that seems somewhere inside between back of TMJ and ear.
9. I weigh 85 kg, when I use a course of Prednisone (37.5 mg /day for first 5 days, 25 mg/ day for second 5 days, and 12.5 mg/day for third 5 days) my hearing improves and I clearly start identifying all words of people’s speech. These improvements also reflect in pure tone audiogram test.
10. CT and MRI scans of brain and MRA and MRV say that all anatomical structures are preserved. No abnormal fluid is detected in ears.
11. Just to add some history of my lower jaw, I had two last molars on both sides grown horizontally which used to cause food impaction frequently, so I had food chewing habit using only one jaw only for many years.
12. Clicking sound on my right jaw in TMJ region when I open my mouth wide.
13. I have my incisors grown outwards, due to which since my childhood, I was unable to keep my mouth shut. So my mandible always used to be hanging down.
14. I also have habit of chewing the food very fast.
Do you think that my hearing problem can be associated with my TMJs or associated neck muscles?
If so, Can I please have some consultation with you through zoom meeting or so?
Your guidance and help in this regard will be highly appreciated.
Sajid
Hi Larsen,
Thank you for writing what is possibly the most in-depth TMJ/tinnitus article available online.
I’d kindly ask for your opinion about my case. I developed tinnitus after my jaw locked open and I forcefully closed it (that was in 2009). I have tinnitus ever since.
While my bite and my posture were fixed in the meantime, the tinnitus remains. What helps is physical therapy, tho. What I wonder is, what do you think has happened when I closed my jaw and if botox would help?
I’ll gladly reserve a consultation with you if you think that it would make sense.
Thank you!
Hi Brian, yeah you’d need to book a consultation.
Your article is fascinating. I have been experience otologic symptoms since June 2022. It started with a unilateral feeling of fullness, then went on to metallic sounding voices, tinnitus, hyperacusis, and intermittent audible clicking sound in that ear. In October I suddenly felt a change in my hearing in that ear, and indeed an audiogram showed that hearing dropped in the low frequencies by about 20-30 DB. I have been monitoring the hearing and I see it fluctuates very regularly, sometimes even going back to normal. I have been to quite a few doctors including ENT’s, neurotologists etc. It seems that they believe it is likely choclear hydrops. What they have not been able to explain is the clicking sound and why EXACTLY the same day that the ear symptoms really began did I start feeling neck crepitus when rotating from left to right, as well as a clicking sound when I open my jaws. I did not have these before. Two doctors even told that I probably had it before but did not pay attention to these symptoms. Am I understanding your article correctly that this could all be related? I also had a cervical MRI which showed Diffuse disc bulge at C5-C6 resulting in contact the right ventral cord, mild to moderate right and minimal left neural foraminal narrowing. They don’t think this is related but would like to hear your thoughts. I would be happy to book a session with you, but I want to confirm that according to your understanding there is relationship between the different symptoms. Thank you very much!
I have had ear noise since I was 16 years old, I am now 64 and the noise is so loud that it makes me nauseated and discouraged by family doctor that said no one knows what causes it. And because of that there is no cure. Your article is interesting but with my simple knowledge it’s as it’s said “Chinese too me”. Please advise me if there are any physicians in the Abilene Texas area that can at least tone the noise down. It is about to drive me crazy and have fallen into depression and anxiety trying to hang on to anything or anyone. Thank you in advance.
Excellent article. I’m practicing physician/internal medicine for 27 years, but haven’t come across such a thorough and well written and explained article about tinnitus. Hats off.
Unfortunately, I am the patient also.
I have pulsatile tinnitus RT ear triggered by drinking cold water, bending, and straining. Crickets sound 24/7/365, and rumbling sound LT ear 24/7/365 for about 2 years was mild 10 years back which was pronounced when sleeping at the time. Used Invisalign for different reasons and may have helped. Stopped using them for about 2 years and have severe tinnitus affecting my quality of life.
All imaging normal. CT temporal were normal.
Do have tense muscles/knots requiring frequent massages. Massage therapists have told they haven’t seen knots like this. Do work long hours, bad posture, and long drives to work.
Cause unknown at this time. Will need your expertise on this.
Forgot to mention,
Had vertigo in 2016 lasted few months, but still have that floating feeling at times.
Hear frequent cracking of neck on movement and clicking in the ear while chewing. Clenching of teeth and jaw very frequent from stress.
RT severe septal deviation, almost closed. Frequent RT temporal headaches, waking up with headaches, RT aural fullness.
I am suspecting TMJ disease, but ENT in NY ( 4 of them) I had seen say they don’t know the cause. Haven’t seen aTMJ specialist yet.
Audiogram x3 showed significant RT side loss and mild left side. Mixed hearing loss.
I tried to access the link to the “ temporomandibular joint disorder” article but was blocked. Can you give me a link?
Probably because I shut down the old domain. Just click jaw in the right toolbar subjects section and you’ll find it.
Hi I’ve massaged my jawbone area too hard for a previous tinnitus problem that has turned out to be caused by something else but after massaging for a few days has caused a new tinnitus which is high pitched and gets worse if I bite something hard. I have tried neck stretching which has helped a bit and a soft food diet which also helps but hasn’t stopped it. I don’t have the usual tmj symptoms but have always had a clicking jaw. Can you recommend doing anything to relieve this?
My tinnitus started during a period of orthodontics: elastics were used, in combination with braces, that drastically shifted my bite. I began developing extreme neck and jaw pain during the process and then the strange stuff started happening…
I started hearing the weirdest stretching noise deep inside my ear (like and elastic band stretching); the stretching noise eventually climaxed into a ping or a sharp snapping/vibrating sound. This was followed by the sharpest pain inside my ear (a stabbing feeling). The ringing started shortly after, along with periodic bouts
Of rapid clicking (Tensor tympani syndrome).
My perception of the “ringing” is not so much auditory in nature, rather it feels more centralized in my cranium. Since my braces were removed, my bite has always felt off (for roughly a decade now); I developed chronic neck tension, a winging scapula, hip and knee distinction and a myriad of muscle imbalances.
For the last decade, I’ve done countless hours of research into possible causes and treatments for my tinnitus, deep down knowing that it all started with my orthodontics. I’ve seen ENTS, neurologists, TMJ specialists and everyone in between — none of them willing to acknowledge the connection as a possible cause.
Over the years I’ve tried to manually stretch my jaw and neck back into the position I feel it should be in: I’ve experienced quite a lot of numbness and tingling during the process (most likely nerve aggravation), but I slowly started to see improvement. I’ve since corrected most of my muscle imbalances and neck tension by researching anatomy and biomechanics: scapular control playing a crucial role in my upper body recovery. Hip and knee issues seemed to have stemmed from a collapsed arch on my left foot (my best guess is this was either caused by modern footwear or a lateral shift created from my neck torsion.
As I continue to improve my symptoms, I’m still holding out hope for my tinnitus to either improve or stop completely. My neck and jaw are slowly releasing and I often feel a stretch deep inside my ear during certain movements. If I silence my tinnitus using my methods, I will return here to share my results.
One question I haven’t been able to figure out is: what was that elastic band stretching noise I kept hearing just before the ringing started?
All the best,
Mike
Hello, I did my MRI and I got to I have bulging disc posterior c5c6, for last 2 months, I have ringing in ears like cracky sound in both ears, when I do massage on neck muscle or swallow or yawning anything that make sound. I did my brain mri hearing test but everything is normal. I don’t know what to do, I have seen so may ENT dr and TMJ specialist but they said everything normal. I don’t know where this sound coming from? I have been doing physiotherapy but minimal improvement. I’m tired with this noise. Please give me some advice.
I have pain in the neck. Vision problems on the left eye, when the pain is strong. My left TMJ pops when eating food. I’ve tried several doctors in Germany. Pain medicaments, amitriptyline, gamapentine etc. I have a mouth guard for the night. But symptoms does not easy. CT, MRi, from head, neck,molars extrusion. One MRI showed trigeminal neuralgia. But my neuro surgeon said it’s not. What do I have? Thanks for the article. I’m training the exercises and to let my mandible in protrusion. Thanks for any comment.
Kjetil, this is a fantastic article! I wish it brought me joy …
I thought I had bilateral tinnitus, but later on I understood that there are 2 unilateral ones (or more) with different origins. The right one corresponds to the left head stratching of the scalene and upper trapezius muscles, I guess. After 5 minutes of stretching, the silence comes. Unfortunately, nothing helps the left one. I have to stress it – I have no pain, nowhere! I have blocked the buccal, lingual nerves and SCM and got no result at all. I tried a bracket for a week, along with posture tools and exercises, TMJ and deep cervical muscle exercises, trigger points, dry needling, and lasers, among other treatments. The ENT is fine, and hearing is fine. No balance problems. 11-13KHz constant frequency, which doesn’t change. Sometimes, rarely, on a slight right and downward turn, it changes to 8000Hz, which for me means it’s switching to a different source of tinnitus. Now I read about the middle facet joints of the third nerve (maybe other facet joints, such as C1-C3, also sing in the same choir).
I’m discharged by every referral I’ve been sent to because of a lack of pain.
I have a number of MRIs and CT scans, with and without contrast, and I am seeking a specialist who can review them.
Kjetil, your opinion is very important.
Kindest regards,
Peter